Chinese Journal of Tissue Engineering Research ›› 2018, Vol. 22 ›› Issue (2): 281-287.doi: 10.3969/j.issn.2095-4344.0019
Previous Articles Next Articles
Graft healing and functional recovery after anterior cruciate ligament reconstruction: a case study of rehabilitation training
- Tianjin University of Sport, Tianjin 300381, China
-
Received:2017-08-13Online:2018-01-18Published:2018-01-18 -
About author:Fu Tao, M.D., Associate professor, Tianjin University of Sport, Tianjin 300381, China -
Supported by:the Innovation Team of Tianjin University of Sport (13th National Games Technology Services); the Scientific and Technological Subject of Tianjin Sports Bureau, No. GY201606
CLC Number:
Cite this article
Fu Tao, Wu Peng, Zhao Lin-liang, Cheng Ji.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
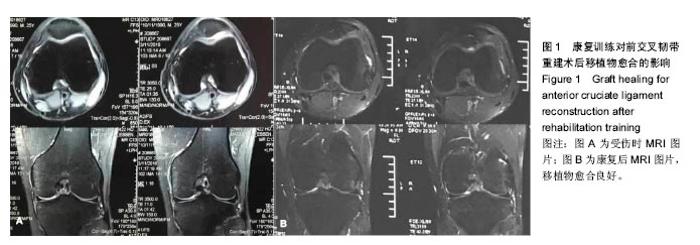
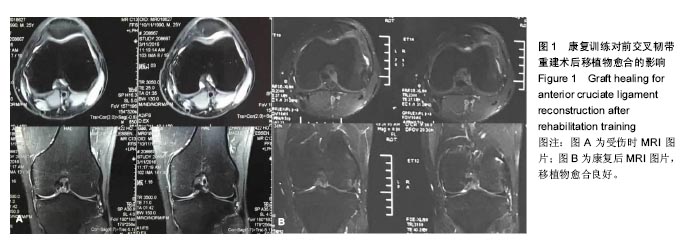
受试者术后至第7周在体育医院进行康复,于术后第8周在天津体育学院进行康复评估,结果如下:左侧髌骨活动度轻微不足;术后瘢痕轻微粘连、伤口甲级愈合;左侧膝关节较稳定,股四头肌内侧头肌力不足;双侧主动、被动屈曲角度不足;左侧膝关节皮温较高,双侧膝关节红外线热成像图,显示左侧膝关节正面温度31.56 ℃,右侧膝关节正面温度30.49 ℃,左右相差1.07 ℃,左侧膝关节侧面温度32.31 ℃,肿胀明显,仍处于明显的炎症期;左侧髂腰肌紧张,左侧臀大肌、臀中肌、腘绳肌、小腿三头肌、胫前肌主动抗阻肌力不足;行走步态正常,能以较正常的步态上下楼梯。于是制定了为期8周的第2阶段康复和各为期3个月的第3,4阶段康复,康复结果如下。 2.1 康复训练对前交叉韧带重建术后移植物愈合的影响 前交叉韧带重建术后8个月拍摄MRI观察移植物愈合的情况,通过影像学观察,移植物愈合良好,见图1。"
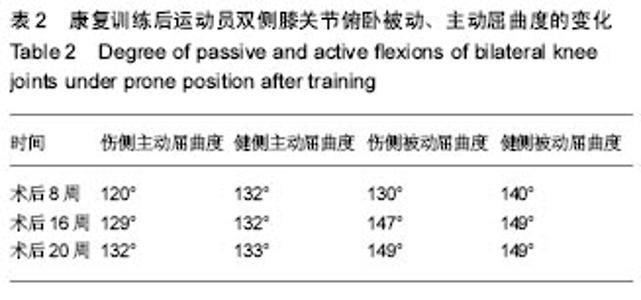
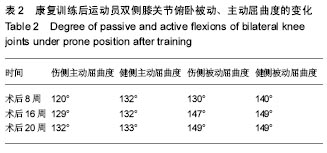
2.2 康复训练对运动员膝关节屈曲度的改善 经过第2阶段康复,受试者坐姿伤侧伸膝角度达到180°,伤侧膝关节俯卧位主动,被动屈曲度均有大幅度提高,在术后20周达到最大,达到预期康复目的,见表2。"
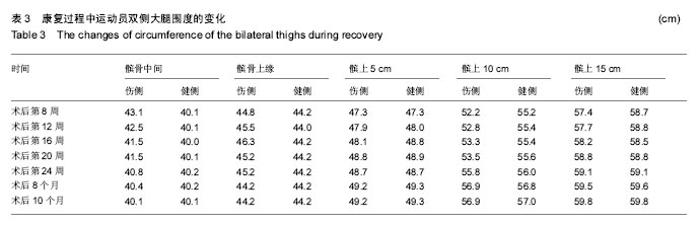
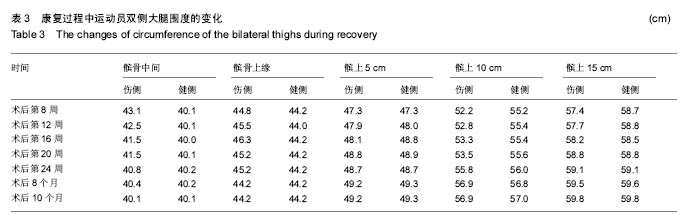
2.3 康复训练对运动员身体形态结构的影响 2.3.1 身体成分的改变 在整个康复训练过程中,身体成分显示体脂百分比明显降低,体脂百分比从第2阶段康复前的20.3%下降到17.9%,但体质量没有变化,这可能与在康复后半程中增加了大重量的力量训练,骨骼肌含量增加有关,上肢、下肢、腰背肌肉力量的增加也佐证了作者的推测。 2.3.2 双侧大腿围度的改变 分别选取了双侧髌骨中间,髌骨上缘,髌骨下缘,髌上5 cm、10 cm、15 cm来反映术后膝关节水肿和大腿股四头肌的变化,在髌骨中间和髌骨上缘由于膝关节存在水肿,伤侧的围度要大于健侧,康复后伤侧围度逐渐变小。康复初期,伤侧股四头肌由于萎缩,其围度明显小于健侧,特别是髌骨上缘10 cm,随着康复,伤侧围度逐渐变大,提示左腿因受伤引起的肌肉萎缩恢复效果优秀,见表3。 "
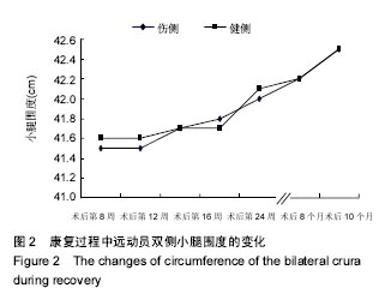
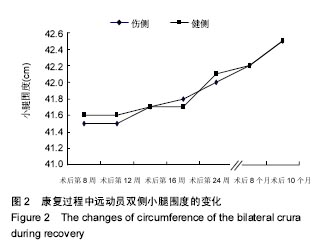
2.3.3 双侧小腿围度的改变 康复结束后,由于腿部训练结合双侧肌肉平衡性训练,双侧小腿腿部肌肉增加明显,左右腿小腿围度差距已经基本消失,提示该运动员下肢康复效果显著,见图2。"
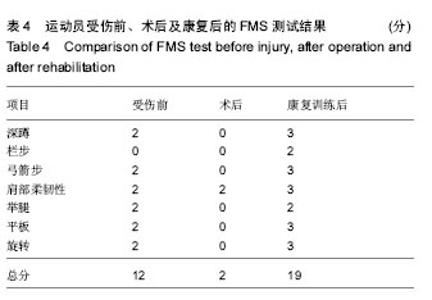
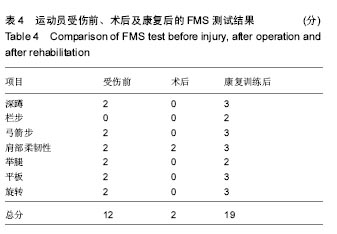
2.4 康复训练对膝关节功能的改善 2.4.1 FMS测试结果 FMS用以检测个体动作控制的稳定性,身体平衡能力、柔韧性及本体感觉等,识别个体的功能限制和不对称发展。受伤前、术后、康复后各项指标评分结果见表4,康复后FMS评分表明膝关节的稳定性和灵活性及整体功能都有了提高,远高出文献中优秀男子橄榄球12.6的得分[16]。"
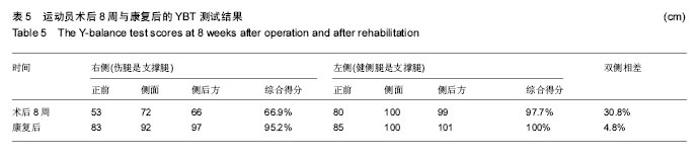
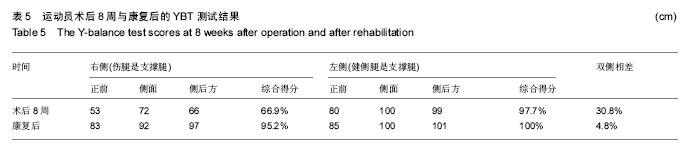
2.4.2 伤侧膝关节单脚跳前馈表现力 术后8周,第2阶段康复前,由于伤侧腿无力支撑,前馈测试未测;健侧腿单脚跳远距离146 cm,与身高比为78.5%。康复后左脚支撑有力,伤侧腿单脚跳远度178 cm,与身高比为95.7%,健侧腿单脚跳远度151 cm,与身高比为81.2%,单腿跳跃测试,男性应达到身高的80%-90%[17],康复后伤侧腿可完成单腿跳跃,健侧腿也较第2阶段康复前有所提高,且伤侧腿为该橄榄球运动员的优势腿,显示出比健侧腿能力更强。 2.4.3 YBT测试结果 下肢的Y平衡测试是一项力量、柔韧、核心控制和本体感觉共同参与的一种单腿动态测试,它被用来评估个体的运动表现,确定个体踝关节、前交叉韧带不稳等状况,还可对是否可参与运动进行筛查,综合评分应大于95%,双侧差异小于5%,测试结果见表5。"

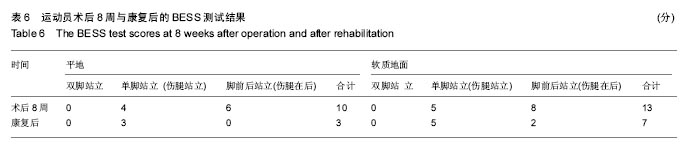
2.4.4 BESS测试评分的改变 BESS平衡纠错评分系统可用于老年人跌倒风险和运动员重返赛场的测试,20-29岁的年轻人,若得分在18-23分则评价为差,表现不好的运动员不能重返赛场,该运动员术后8周评估得分23分,评价为差;康复后评估得分为10分(表6),表现良好,具备重返赛场的可能。 2.4.5 单脚静态平衡能力增加 术后8周,在左右方向速度上,健侧要高于患侧9 mm/s;在前后方向速度上,患侧和健侧差异不大,故此,在康复过程中要着重左右方向的训练;在运动面积上健侧要明显高于患侧;在重心投影的测试中可以看到,患侧较健侧无论是X轴还是Y轴,患侧偏移的更大。通过8个月的康复,健侧与患侧的平衡能力都明显改善,在左右方向速度和前后方向速度上,患侧和健侧无差异;在运动面积上改善最为明显,运动长度改善非常显著,X轴和Y轴投影上,患侧和健侧差异都变小;重心投影由的第二象限变为第一象限,整体重心偏前,总体重心较术后8周有所恢复,证明康复训练后该橄榄球运动员单脚静态平衡能力明显提高。 "
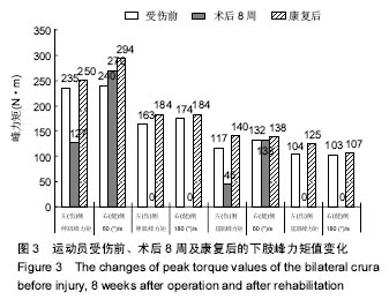
2.4.6 双脚动态平衡能力增加 在术后8周动态稳定性评估时,躯干左右晃动程度明显大于前后晃动,表明该运动员身体左右方向控制不稳定,而前后较好;在随后的康复训练中,加强了左右方向的动态性平衡训练,康复后,躯干左右晃动程度明显改善。 上述功能测试,提示康复训练后该运动员的膝关节功能恢复的较好,具备重返赛场的条件之一[18]。 2.5 康复训练对肌肉力量及爆发力的改变 下肢等速肌力功测试结果:对同一项目运动员,参与工作的肌群是相对固定的,通过等速肌力测试对运动员康复前后下肢肌肉的肌力的特征进行评价[16,19]。因出于对运动员的保护,术前未进行下肢等速肌力测试,术后第8周未进行180 (°)/s的等速肌力测试。 峰力矩是关节屈伸过程中最大力矩的表达,是肌肉力量的体现,有较好的重复性,被视为等速测试的黄金标准和参照值。术后8周下肢等速肌力的测试显示:角速度在 60 (°)/s时,健侧的伸肌、屈肌峰力矩值比受伤前(冬训前的数据)略高,但伤侧的伸肌、屈肌峰力矩值不及受伤前的一半,特别是屈肌峰力矩值,仅为受伤前的38%。与术后8周相比,康复后,无论是伤侧还是健侧的总功,60 (°)/s健侧、伤侧的伸肌、屈肌峰力矩值均有明显提高,甚至超过受伤前的水平(图3),有研究认为受伤前参与运动的水平作为评价返回运动的比较基线是较为可靠的[20]。测试时伸肌力矩曲线呈现正常,无平台期,认为可以归队正常训练,并为归队后灵敏性和本体感觉的训练提供基础。 关节最大可动范围,屈肌峰力矩角度只有健侧在 60 (°)/s时比受伤前降低了15°,其余的指标均有所增加。肌肉爆发力指标中到达峰力矩的时间,即伸屈膝部肌肉达到最大力量的时间。在时间参数上,无论是在60 (°)/s还是在180 (°)/s,伸肌和屈肌达到峰力矩的时间都变短,结合到达关节峰力矩的角度一同分析,发现屈肌峰力矩角度只有健侧在60 (°)/s时比受伤前变小,其余指标均接近或达到受伤前的数据,表明肌肉爆发力有所增加。 2.6 膝关节评分和膝关节稳定性检查结果 Lysholm膝关节评分由第2阶段康复训练前48分提高到85分,Lanchman试验和膝关节轴移试验均为阴性。 结合术后时间(6-9个月是再次损伤发病率最高的时间段,术后10个月后回归的风险降低明显[21])、等速肌力测试和膝关节功能恢复情况,认为该运动员的康复训练是行之有效的,具备重返赛场的条件。"

| [1]McIntoah AS,McCrory P,Comerford J.The dynamics of concussive head impacts in rugby and Australian rules football.Med Sci Sports Exerc.2000;32:1980-1984.[2]陈连旭,付立功.前交叉韧带断裂和重建的临床流行病学分析[J].中国组织工程研究, 2016,20(24):3602-3608.[3]Kiapour AM, Murray MM. Basic science of anterior cruciate ligament injury and repair.Bone Joint Res.2014;3(2):20-31.[4]Faude O,Junge A,Kindermann W,et al.Injuries in female soccer players: A prospective study in the german national league.Am J Sports Med.2005;33(11):1694-1700.[5]周长敬,刘卉,李翰君,等.前交叉韧带损伤预防手段研究进展[J].中国运动医学杂志,2015,34(1):82-90. [6]葛杰,周谋望,敖英芳,等.关节镜下膝前交叉韧带重建术后的康复[J].中国康复医学杂志,2003, 18(12):743-746.[7]杨涛,周敬滨,李国平.膝前十字韧带重建术后重返运动的研究进展[J].体育科学,2016,36(10):74-79.[8]Setuain L,Lzquierdo M,Ldoate F.Differential Effects of Two Rehabilitation Programs Following Anterior Cruciate Ligament Reconstruction.J Sport Rehabilition.2016;65:1-37.[9]Adams D,Logerstedt DS,Hunter-Giordano A,et al.Current Concepts for Anterior Cruciate Ligament Reconstruction: A Criterion–Based Rehabilitation Progression.J Orthop Sports Phys Ther.2012;42(7): 601-614.[10]张付,徐雁.终结膝痛[M].苏州:江苏凤凰科技出版社,2015.[11]Mather RC,Hettrich CM,Dunn WR,et al.Cost-Effectiveness Analysis of Early Reconstruction Versus Rehabilitation and Delayed Reconstruction for Anterior Cruciate Ligament Tears.Clin Sports Med.2015;34(2):301-312.[12]Hahn J,Shin S,Lee W.The effect of modified trampoline training on balance, gait, and falls efficacy of stroke patients.J Phys Ther Sci.2015;27(11):3351-3354.[13]Cook G,Burton L,Fields K.The Functional Movement Screen and Exercise Progressions Manual.2011:19-79.[14]Lee SM,Lee JH.The immediate effects of ankle balance taping with kinesiology tape on ankle active range of motion and performance in the Balance Error Scoring System.Phys Ther Sport.2017;25:99-105. [15]Sun L,Lin DE,Fan J.Editorial: Functional testing in the assessment of return to sports after anterior cruciate ligament reconstruction.Ann Transl Med.2015;3(16):225-226.[16]鲁智勇,李伟,解强.我国优秀橄榄球运动员身体功能特点研究[J].中国体育科技,2016,52(2):141-145.[17]DiFabio M,Slater LV,Norte G.Relationships of Functional Tests Following ACL Reconstruction: Exploratory Factor Analyses of the Lower Extremity Assessment Protocol.J Sport Rehabil. 2017;9:1-24.[18]Mayer SW,Queen RM,Taylor D.Functional Testing Differences in Anterior Cruciate Ligament Reconstruction Patients Released Versus Not Released to Return to Sport.Am J Sports Med. 2015;43(7):1648-1655.[19]刘晓鹏,安华,于长隆.应用等速肌力测试评价膝前交叉韧带断裂重建术后康复的效果[J].中国运动医学杂志, 2008,25(5): 286-289.[20]Feller JA,Webster KE.A randomized comparison of patellar tendon and hamstring tendon anterior cruciate ligament reconstruction.Am J Sports Med.2003;31(4):143-144.[21]Ardern CL,Webster KE,Taylor NF,et al.Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play.Br J Sports Med. 2011;45(7):596-606. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [3] | Liu Shaohua, Zhou Guanming, Chen Xicong, Xiao Keming, Cai Jian, Liu Xiaofang. Influence of anterior cruciate ligament defect on the mid-term outcome of fixed-bearing unicompartmental knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 860-865. |
| [4] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [5] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [6] | Ma Ziyue, Ju Xiaochen, Zhang Lei, Sun Rongxin. Tendon-bone healing in anterior cruciate ligament reconstruction with and without remnant preservation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 582-587. |
| [7] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [8] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [9] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [10] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [11] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [12] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [13] | Chen Siqi, Xian Debin, Xu Rongsheng, Qin Zhongjie, Zhang Lei, Xia Delin. Effects of bone marrow mesenchymal stem cells and human umbilical vein endothelial cells combined with hydroxyapatite-tricalcium phosphate scaffolds on early angiogenesis in skull defect repair in rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3458-3465. |
| [14] | Wang Hao, Chen Mingxue, Li Junkang, Luo Xujiang, Peng Liqing, Li Huo, Huang Bo, Tian Guangzhao, Liu Shuyun, Sui Xiang, Huang Jingxiang, Guo Quanyi, Lu Xiaobo. Decellularized porcine skin matrix for tissue-engineered meniscus scaffold [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3473-3478. |
| [15] | Mo Jianling, He Shaoru, Feng Bowen, Jian Minqiao, Zhang Xiaohui, Liu Caisheng, Liang Yijing, Liu Yumei, Chen Liang, Zhou Haiyu, Liu Yanhui. Forming prevascularized cell sheets and the expression of angiogenesis-related factors [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3479-3486. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||