Chinese Journal of Tissue Engineering Research ›› 2026, Vol. 30 ›› Issue (21): 5582-5588.doi: 10.12307/2026.697
Previous Articles Next Articles
Morphological measurement of anterior cervical pedicle screw placement assisted by Mimics three-dimensional CT reconstruction
Hu Yin1, Xing Le2, Han Kangen1, Li Junchao1, Qian Mengran1, Gu Hongwen2, Yu Hailong2, Wang Hongwei2
- 1Graduate School of Dalian Medical University, Dalian 116044, Liaoning Province, China; 2Department of Orthopedics, General Hospital of Northern Theater Command, Shenyang 110016, Liaoning Province, China
-
Accepted:2025-05-20Online:2026-07-28Published:2026-03-05 -
Contact:Wang Hongwei, MD, Associate chief physician, Department of Orthopedics, General Hospital of Northern Theater Command, Shenyang 110016, Liaoning Province, China -
About author:Hu Yin, MS candidate, Graduate School of Dalian Medical University, Dalian 116044, Liaoning Province, China -
Supported by:Shenyang Science and Technology Program, No. 22-321-33-35 (to WHW)
CLC Number:
Cite this article
Hu Yin, Xing Le, Han Kangen, Li Junchao, Qian Mengran, Gu Hongwen, Yu Hailong, Wang Hongwei. Morphological measurement of anterior cervical pedicle screw placement assisted by Mimics three-dimensional CT reconstruction[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(21): 5582-5588.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
2.1 参与者数量分析 收集63例因颈背部疼痛就诊完善颈椎CT检查的患者,排除伴有严重退行性改变患者5例、颈椎畸形患者4例、颈椎管内占位性病变2例、颈椎骨折患者2例,最终纳入分析共50例患者,将其颈椎C3-C7三维CT的形态学测量结果进行汇总分析。CT数据包括250个颈椎,测量过程共产生5 000个参数。 2.2 试验流程图 见图2。"

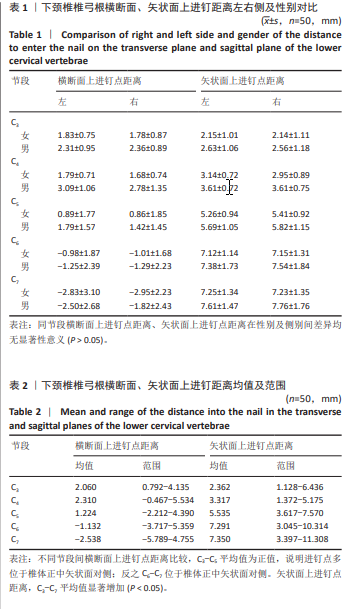
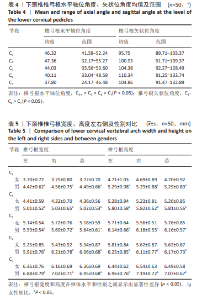
2.3 进钉点的定位 如表1,2所示,横断面上进钉点距离、矢状面上进钉点距离在男性与女性、左右两侧的总体均值差异无显著性意义(P > 0.05)。从C3开始,左、右侧椎弓根中轴线在椎体前壁的投影点有从对侧上终板走向同侧下终板的趋势。C4进钉点距离正中矢状线略大于C3,均在2 mm左右,C5进钉点到正中矢状线距离的平均值在椎弓根对侧,但从测量上看,C5既可在同侧也可在对侧(-2.212- 4.390 mm)。其次,矢状面上进钉点距离在所有椎体水平之间存在显著性差异(P < 0.000 1)。C3最接近上终板(2.362 mm),C7距离上终板最远(7.350 mm)。"
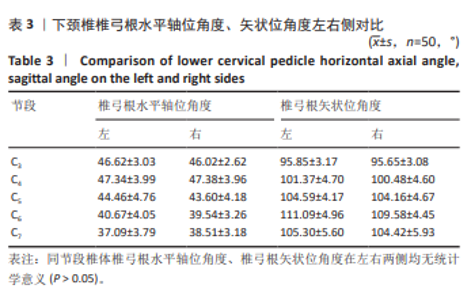
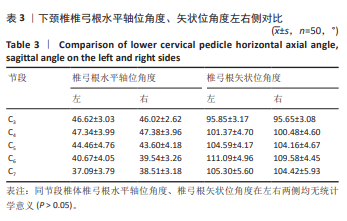
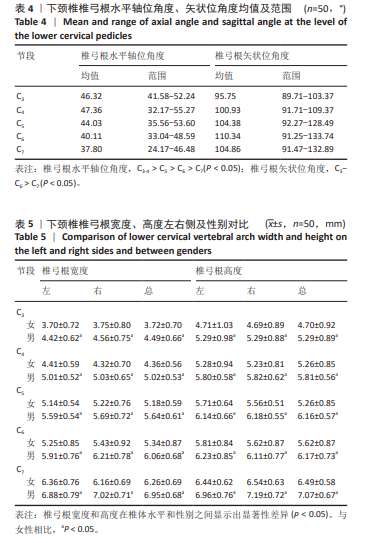
2.4 进钉方向 如表3,4所示,所有的椎弓根水平轴位角度和椎弓根矢状位角度在男女之间和左右侧之间差异无显著性意义(P > 0.05)。从整体上看,除C3外,C4-C7横切面椎弓根的角度由47.36°显著减低至37.80°,C3的横切面椎弓根角的大小与C4接近,为46.32°。而针对矢状面的椎弓根角度,除C7外,从C3-C6,矢状面的椎弓根角度由95.75°显著增加至110.34°,C6角度最大。"
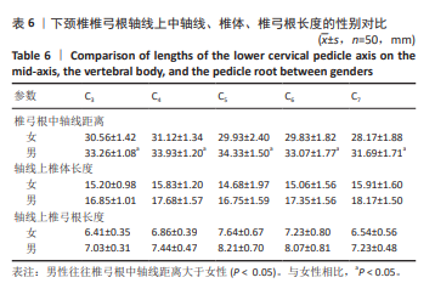
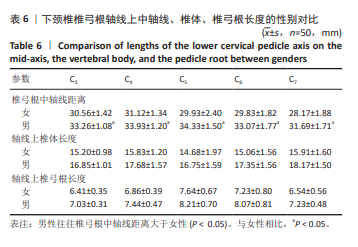
2.5 螺钉参数 如表5,6所示,所有患者的平均椎弓根宽度、椎弓根高度在左右侧之间无显著性差异,但对于性别及椎体水平差异有显著性意义(P < 0.05)。在所有水平上,男性的椎弓根宽度及椎弓根高度往往大于女性,并且从C3-C7是递增的。对于椎弓根中轴线距离,在左右侧之间无显著性差异,但男性往往椎弓根中轴线距离大于女性,整体上看,在C3、C4水平时,平均椎弓根中轴线距离值相对较大,轴线上椎体长度也相对较大,分别为15.99 mm,16.72 mm;C5-C7平均椎弓根中轴线距离呈下降趋势,C7水平椎弓根中轴线距离最小,分别为(31.69±1.71) mm和(28.17±1.88) mm。但轴线上椎体长度逐渐增大,平均值分别为15.87,15.96,17.00 mm,相反椎弓根长度逐渐减小,左右侧之间差异无显著性意义(P > 0.05)。"
"
| [1] ARTS MP, BRAND R, VAN DEN AKKER E, et al. The NEtherlands Cervical Kinematics (NECK) trial. Cost-effectiveness of anterior cervical discectomy with or without interbody fusion and arthroplasty in the treatment of cervical disc herniation; a double-blind randomised multicenter study. BMC Musculoskelet Disord. 2010;11:122. [2] MONTANO N, RICCIARDI L, OLIVI A. Comparison of Anterior Cervical Decompression and Fusion versus Laminoplasty in the Treatment of Multilevel Cervical Spondylotic Myelopathy: A Meta-Analysis of Clinical and Radiological Outcomes. World Neurosurg. 2019;130:530-536.e2. [3] DAI L, QIN C, GUO P, et al. Comparison of anterior cervical diskectomy with fusion (ACDF) and laminoplasty treating multilevel cervical spondylotic myelopathy with developmental canal stenosis: a retrospective study. J Orthop Surg Res. 2024;19(1):29. [4] HUANG W, TIAN Y, WANG H, et al. Comparative analysis of the biomechanics of anterior cervical discectomy and fusion with multiple segmental plates fixation versus single multilevel plate fixation: a finite element study. BMC Musculoskelet Disord. 2022;23(1):848. [5] CHIN KR, CUMMING VB, HENSON M, et al. Effects of misalignment on static torsional strength of anterior cervical plate systems. Spine J. 2013;13(11):1544-1548. [6] KOLLER H, ACOSTA F, TAUBER M, et al. Cervical anterior transpedicular screw fixation (ATPS)--Part II. Accuracy of manual insertion and pull-out strength of ATPS. Eur Spine J. 2008;17(4):539-555. [7] KOLLER H, HITZL W, ACOSTA F, et al. In vitro study of accuracy of cervical pedicle screw insertion using an electronic conductivity device (ATPS part III). Eur Spine J. 2009;18(9):1300-1313. [8] TOMASINO A, PARIKH K, KOLLER H, et al. The vertebral artery and the cervical pedicle: morphometric analysis of a critical neighborhood. J Neurosurg Spine. 2010;13(1):52-60. [9] KOTIL K, AKÇETIN MA, SAVAS Y. Neurovascular complications of cervical pedicle screw fixation. J Clin Neurosci. 2012;19(4):546-551. [10] ATALAR K, COŞKUN ZK, KAYMAZ AM. Optimal screw positioning in cervical pedicles to avoid complications. Turk J Med Sci. 2022;52(4): 1118-1129. [11] KOKTEKIR E, TOKTAS ZO, SEKER A, et al. Anterior transpedicular screw fixation of cervical spine: Is it safe? Morphological feasibility, technical properties, and accuracy of manual insertion. Journal of Neurosurgery: Spine. 2015;22(6):596-604. [12] FU MQ, LIN LJ, KONG XX, et al. Construction and Accuracy Assessment of Patient-Specific Biocompatible Drill Template for Cervical Anterior Transpedicular Screw (ATPS) Insertion: An In Vitro Study. PLoS One. 2013;8(1):8. [13] WANG L, ZHAO L, GU Y, et al. Effectiveness of 2 Types of Drill Templates for Cervical Anterior Transpedicular Screw Placements: A Comparative Study. World Neurosurg. 2021;147:e343-e350. [14] LV Y, TIAN W, CHEN D, et al. The prevalence and associated factors of symptomatic cervical Spondylosis in Chinese adults: a community-based cross-sectional study. BMC Musculoskelet Disord. 2018;19(1): 325. [15] BOOCKVAR JA, PHILIPS MF, TELFEIAN AE, et al. Results and risk factors for anterior cervicothoracic junction surgery. J Neurosurg. 2001; 94(1 Suppl):12-17. [16] YE SQ, YE JC, HOU ZP, et al. Biomechanical study of anterior transpedicular root screw intervertebral fusion system of lower cervical spine: a finite element analysis. Front Bioeng Biotechnol. 2024;12:13. [17] DAUBS MD. Early failures following cervical corpectomy reconstruction with titanium mesh cages and anterior plating. Spine (Phila Pa 1976). 2005;30(12):1402-1406. [18] HUANG SB, LING QJ, LIN XX, et al. Biomechanical evaluation of a novel anterior transpedicular screw-plate system for anterior cervical corpectomy and fusion (ACCF): a finite element analysis. Front Bioeng Biotechnol. 2023;11:11. [19] DUNLAP BJ, KARAIKOVIC EE, PARK HS, et al. Load sharing properties of cervical pedicle screw-rod constructs versus lateral mass screw-rod constructs. Eur Spine J. 2010;19(5):803-808. [20] KOLLER H, SCHMIDT R, MAYER M, et al. The stabilizing potential of anterior, posterior and combined techniques for the reconstruction of a 2-level cervical corpectomy model: biomechanical study and first results of ATPS prototyping. Eur Spine J. 2010;19(12):2137-2148. [21] KAST E, MOHR K, RICHTER HP, et al. Complications of transpedicular screw fixation in the cervical spine. Eur Spine J. 2006;15(3):327-334. [22] ONIBOKUN A, KHOO LT, BISTAZZONI S, et al. Anatomical considerations for cervical pedicle screw insertion: the use of multiplanar computerized tomography measurements in 122 consecutive clinical cases. Spine J. 2009;9(9):729-734. [23] SOLIMAN MAR, AGUIRRE AO, KHAN S, et al. Complications associated with subaxial placement of pedicle screws versus lateral mass screws in the cervical spine (C2-T1): systematic review and meta-analysis comprising 4,165 patients and 16,669 screws. Neurosurg Rev. 2023; 46(1):61. [24] 李杰, 赵刘军, 干开丰, 等. 下颈椎两节段椎体次全切后前路椎弓根螺钉固定系统重建稳定性有限元模型的建立[J]. 中国骨伤,2022, 35(2):178-185. [25] 吴晓宇, 董谢平, 吴彦超, 等. 3D打印颈椎前路椎弓根螺钉导板的准确性评估[J]. 中国矫形外科杂志,2018,26(6):538-542. [26] 盛晓磊, 袁峰, 李智多, 等. 3D打印组合式导板辅助下颈椎前路椎弓根螺钉置入与徒手置钉的准确性对比[J]. 中国组织工程研究, 2017,21(3):406-411. [27] 肖进, 尹庆水, 张美超, 等. Mimics软件重建脊柱三维骨骼数据基础上快速成型的脊柱畸形模型[J]. 中国组织工程研究与临床康复, 2008,12(35):6835-6838. [28] EBRAHEIM NA, XU R, KNIGHT T, et al. Morphometric evaluation of lower cervical pedicle and its projection. Spine (Phila Pa 1976). 1997; 22(1):1-6. [29] HERRERO CF, LUIS DO NASCIMENTO A, MARANHO DAC, et al. Cervical pedicle morphometry in a Latin American population: A Brazilian study. Medicine (Baltimore). 2016;95(25):e3947. [30] 王远政, 刘洋, 邓忠良. 下颈椎前路椎弓根螺钉置入的实验研究[J]. 第三军医大学学报,2012,34(18):1839-1843. [31] KARAIKOVIC EE, DAUBS MD, MADSEN RW, et al. Morphologic characteristics of human cervical pedicles. Spine (Phila Pa 1976). 1997; 22(5):493-500. [32] BREDOW J, MEYER C, SCHEYERER MJ, et al. Accuracy of 3D fluoroscopy-navigated anterior transpedicular screw insertion in the cervical spine: an experimental study. Eur Spine J. 2016;25(6):1683-1689. [33] GUPTA R, KAPOOR K, SHARMA A, et al. Morphometry of typical cervical vertebrae on dry bones and CT scan and its implications in transpedicular screw placement surgery. Surg Radiol Anat. 2013;35(3): 181-189. [34] RUOFU Z, HUILIN Y, XIAOYUN H, et al. CT evaluation of cervical pedicle in a Chinese population for surgical application of transpedicular screw placement. Surg Radiol Anat. 2008;30(5):389-396. [35] CHEN C, RUAN D, WU C, et al. CT morphometric analysis to determine the anatomical basis for the use of transpedicular screws during reconstruction and fixations of anterior cervical vertebrae. PLoS One. 2013;8(12):e81159. [36] ZHENG R, CHEN Y, YAO G, et al. Computed Tomography-Based Morphometric Analysis of Lower Cervical Anterior Transpedicular Screw Fixation and Related Factors in the Chinese Population. World Neurosurg. 2024;182:e721-e733. [37] GELALIS ID, PASCHOS NK, PAKOS EE, et al. Accuracy of pedicle screw placement: a systematic review of prospective in vivo studies comparing free hand, fluoroscopy guidance and navigation techniques. Eur Spine J. 2012;21(2):247-255. [38] KWON JW, ARREZA EO, SUGUITAN AA, et al. Medial Pedicle Pivot Point Using Preoperative Computed Tomography Morphometric Measurements for Cervical Pedicle Screw Insertion: A Novel Technique and Case Series. J Clin Med. 2022;11(2). doi:10.3390/jcm11020396. [39] 董亮, 谭明生, 移平, 等. 颈椎前路椎弓根螺钉置入的解剖学研究[J]. 中国矫形外科杂志,2014,22(2):138-143. [40] CHACHAN S, BIN ABD RAZAK HR, LOO WL, et al. Cervical pedicle screw instrumentation is more reliable with O-arm-based 3D navigation: analysis of cervical pedicle screw placement accuracy with O-arm-based 3D navigation. Eur Spine J. 2018;27(11):2729-2736. [41] GUHA D, JAKUBOVIC R, GUPTA S, et al. Intraoperative Error Propagation in 3-Dimensional Spinal Navigation From Nonsegmental Registration: A Prospective Cadaveric and Clinical Study. Global Spine J. 2019;9(5): 512-520. [42] WESTERMANN L, SPEMES C, EYSEL P, et al. Computer tomography-based morphometric analysis of the cervical spine pedicles C3-C7. Acta Neurochir (Wien). 2018;160(4):863-871. [43] NAKASHIMA H, YUKAWA Y, IMAGAMA S, et al. Complications of cervical pedicle screw fixation for nontraumatic lesions: a multicenter study of 84 patients. J Neurosurg Spine. 2012;16(3):238-247. [44] 王力冉, 赵刘军, 顾勇杰, 等. 3D打印导航模板引导双侧下颈椎前路椎弓根螺钉置钉的可行性[J]. 中国脊柱脊髓杂志,2016,26(11): 1012-1017. [45] WANG Y, XIE J, YANG Z, et al. Computed tomography assessment of lateral pedicle wall perforation by free-hand subaxial cervical pedicle screw placement. Arch Orthop Trauma Surg. 2013;133(7):901-909. |
| [1] | Cheng Qisheng, Julaiti·Maitirouzi, Xiao Yang, Zhang Chenwei, Paerhati·Rexiti. Finite element analysis of novel variable-diameter screws in modified cortical bone trajectory of lumbar vertebrae [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2162-2171. |
| [2] | Zhu Xiaolong, Zhang Wei, Yang Yang. Visualization analysis of research hotspots and cutting-edge information in the field of intervertebral disc regeneration and repair [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2391-2402. |
| [3] | Wen Fayan, Li Yan, Qiang Tianming, Yang Chen, Shen Linming, Li Yadong, Liu Yongming. Unilateral biportal endoscopic technology for treatment of lumbar degenerative diseases: global research status and changing trends [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2380-2390. |
| [4] | Xinjiang Branch of China Trauma Rescue & Treatment Association. Expert consensus on diagnosis and treatment of brucellar osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2403-2412. |
| [5] | Zhao Feifan, Cao Yujing. Risk factors and coping strategies of internal fixation failure in treatment of intertrochanteric fracture with proximal femoral nail antirotation [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2323-2333. |
| [6] | Li Zhifei, Han Bin, Liu Qiuli, Zhang Zhanming, Wei Haokai, Zuo Kuangshi, Zhang Yisheng. Cervical motion characteristics in patients with cervical spondylotic radiculopathy based on motion capture technology [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2286-2293. |
| [7] | Li Sa, Sun Ning, Sun Zhaozhong, Feng Zhimeng, Li Xuedong. Evaluation parameters and specific region of C6 nerve oppression by uncinate process degeneration [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2294-2302. |
| [8] | Wang Nan, Chen Shuang, Xi Zhipeng, Qian Yuzhang, Zhang Xiaoyu, Gu Jun, Kang Ran, Xie Lin. MRI evaluation of nerve root subsidence sign affecting efficacy of percutaneous endoscopic decompression in lumbar spinal stenosis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2262-2268. |
| [9] | Chen Haojie, Wang Dai, Shen Shan. Immune inflammatory microenvironment mechanisms in peri-implantitis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 2054-2062. |
| [10] | Yang Qiongqiong, Liu Wei. Comparison of performance and clinical effects of zirconia and titanium implants [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 2063-2071. |
| [11] | Liu Yang, Liu Donghui , Xu Lei, Zhan Xu, Sun Haobo, Kang Kai. Role and trend of stimuli-responsive injectable hydrogels in precise myocardial infarction therapy [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 2072-2080. |
| [12] | Wang Zheng, Cheng Ji, Yu Jinlong, Liu Wenhong, Wang Zhaohong, Zhou Luxing. Progress and future perspectives on the application of hydrogel materials in stroke therapy [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 2081-2090. |
| [13] | Guo Yuchao, Ni Qianwei, Yin Chen, Jigeer·Saiyilihan, Gao Zhan . Quaternized chitosan hemostatic materials: synthesis, mechanism, and application [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 2091-2100. |
| [14] | Liu Dawei, Cui Yingying, Wang Fanghui, Wang Zixuan, Chen Yuhan, Li Yourui, Zhang Ronghe. Epigallocatechin gallate-mediated bidirectional regulation of reactive oxygen species and its application in nanomaterials [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 2101-2112. |
| [15] | Lai Yu, Chen Yueping, Zhang Xiaoyun. Research hotspots and frontier trends of bioactive materials in treating bone infections [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 2132-2144. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||