Chinese Journal of Tissue Engineering Research ›› 2020, Vol. 24 ›› Issue (12): 1935-1940.doi: 10.3969/j.issn.2095-4344.2525
Previous Articles Next Articles
Types and advantages of spinal implants in percutaneous kyphoplasty
Gao Jian’an, Chen Xi, Zhang Longsheng, Liao Wenbo
- Department of Spine Surgery, Affiliated Hospital of Zunyi Medical University, Zunyi 563000, Guizhou Province, China
-
Received:2019-09-26Revised:2019-09-28Accepted:2019-10-25Online:2020-04-28Published:2020-03-03 -
Contact:Liao Wenbo, MD, Chief physician, Department of Spine Surgery, Affiliated Hospital of Zunyi Medical University, Zunyi 563000, Guizhou Province, China -
About author:Gao Jian’an, Master candidate, Department of Spine Surgery, Affiliated Hospital of Zunyi Medical University, Zunyi 563000, Guizhou Province, China -
Supported by:the Science and Technology Project of Guizhou Province, No. [2019]2812
CLC Number:
Cite this article
Gao Jian’an, Chen Xi, Zhang Longsheng, Liao Wenbo. Types and advantages of spinal implants in percutaneous kyphoplasty[J]. Chinese Journal of Tissue Engineering Research, 2020, 24(12): 1935-1940.
share this article
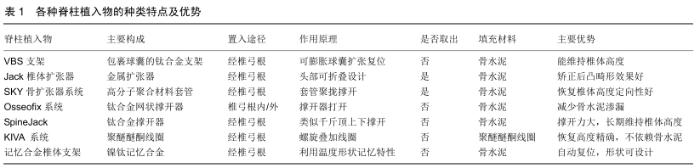
各种脊柱植入物的种类特点及主要优势见表1。 "
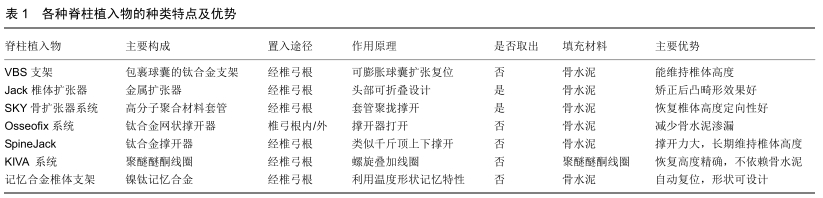

2.1 VBS支架 椎体支架(Vertebral Body Stending, VBS,瑞士)是一种经皮微创治疗椎体压缩性骨折的装置,主要结构是头端包裹着球囊的钛合金支架,球囊与可膨胀式气囊类似,可用于充气膨胀与支架撑开重新复位塌陷的椎体,将支架留在椎体内部并撤出球囊,在低压状态下向支架空腔内注入骨水泥[14-15]。适应证主要是没有后壁受累的骨质疏松性椎体压缩骨折,以及椎体骨皮质完整的椎体内溶骨性病变[16-17]。椎体支架置入需在透视下通过双侧椎弓根入路,在椎体内向中线对称的放置2个支架,充气系统需要同时扩张两侧的支架,膨胀的支架可在椎体内创造一个明确的空腔,允许在低压下注射骨水泥。生物力学实验显示,VBS椎体成形术与球囊后凸成形术相比,对伤椎的高度恢复明显占优势[18-21];同样在减轻疼痛方面,临床试验更倾向于VBS椎体支架成形术而不是后凸成形术。另外,VBS椎体支架在有效维持椎体高度的同时为骨水泥注入提供空腔,有利于减少骨水泥渗漏[21]。但WERNER等[22]进行一项VBS椎体支架与球囊相比较的试验,结果显示VBS相比于球囊后凸成形术在骨水泥渗漏、辐射暴露时间和神经系统后遗症方面没有益处。理论上来说,在撤出球囊后有支架的支撑作用,可避免恢复的椎体高度再降低,对脊柱后凸畸形纠正更具优势[23-25]。 2.2 Jack椎体扩张器 Jack椎体扩张器(中国,江苏)是依据解剖上胸腰段椎弓根高宽比例特点来设计的,其扩张器的头部采用可折叠设计,操作时需保证扩张器头部竖立,使面积较宽的部分对向上下终板,顺时针旋转手柄张开扩张器,撑开上下终板复位塌陷椎体,并形成椎体内空腔在注射骨水泥加固[23,26]。Jack椎体扩张器设计上分为4.8 mm×7 mm及5.3 mm×8 mm两种型号,其最大撑开高度和骨水泥容量分别是16 mm,2.0 mL和19 mm,2.5 mL。卞元健等[27]应用Jack椎体扩张器和经皮球囊椎体后凸成形分别对24例椎体压缩骨折标本进行生物力学实验对比,结果表明两者术后在椎体的最大载荷、抗压强度及刚度方面并无明显差异,Jack椎体扩张器还可以有效提高骨质疏松性椎体压缩性骨折术后抗塌陷能力,达到加强骨折椎体的目的。LI等[28]报道了16例接受Jack椎体扩张器手术的椎体压缩性骨折患者并进行平均19个月随访,表明Jack椎体扩张器能有效缓解疼痛的同时,能更好地恢复椎体高度及矫正后凸畸形,并在一定程度上减少骨水泥渗漏。JIN等[29]对218例骨质疏松性椎体压缩性骨折应用Jack椎体扩张器治疗,末次随访时椎前缘高度、Cobb角度由术前的(19.3±3.2) mm、(16.2±6.6)°改善至(24.9±2.6) mm及(8.5±5.6)°,目测类比评分、Oswestry功能障碍指数由术前的(8.2±1.3)分、(78.2± 13.3)%改善至(1.8±0.8)分、(20.9±6.8)%。但由于Jack扩张器扩张依靠的是刚性的机械张力,存在过度加压使得骨皮质发生继发性破裂的风险[30]。另外其手术过程中所需工作通道比球囊扩张器粗,因此对椎弓根宽度较窄的病例有所限制。 2.3 SKY骨扩张系统 SKY骨扩张系统(Sky Bone Expender System,以色列)主要用于骨质疏松性椎体压缩性骨折和陈旧性椎体骨折[31-34]。SKY骨扩张器是采用高分子聚合材料制成的可塑形套管,其操作是在建立椎弓根工作通道后,将头端套管置入塌陷椎体的中心部位,再通过尾端螺旋使套管向头端聚拢,套管聚拢呈放射状扩张,起到撑开塌陷椎体的作用,取出时反向旋转尾端使套管恢复,取出后可在椎体内留下空腔,再灌注骨水泥加固强 化[32-33]。SKY骨扩张器分14 mm、16 mm两种规格,该装置在扩张过程中有良好的定向性。XIONG等[34]对25例27节压缩骨折的伤椎行SKY骨扩张器治疗,随访1年伤椎Cobb角(9.8±9.76)°、目测类比评分(0.80±0.94)分、Oswestry功能障碍指数(9.13±2.45)%,与术前(17.18± 9.35)°、(6.82±2.12)分及(42.88 ±3.95)%比较差异有显著性意义。ZHENG等[35]应用SKY骨扩张器对15例18节骨质疏松性椎体压缩性骨折手术,指出SKY具有明显的止痛作用,以及操作方便、缩短卧床时间的优势。然而SKY骨扩张器也有不足之处,如SKY骨扩张器在扩张后碎骨屑易嵌入套管间隙内从而导致不容易取出;另外头端套管聚拢时局部张力可造成骨皮质损伤,空腔的裂隙不均质,增加了骨水泥渗漏的风险。 2.4 Osseofix系统 Osseofix系统(美国,加利福尼亚州)主要应用于椎体压缩性骨折的治疗,同样是采用钛合金制作的网状椎体内固定装置,并联合骨水泥的应用对伤椎起到固定及稳定的作用,临床上主要用于T6-L5的椎体压缩性骨折,可经椎弓根内或外通道置入[23,36]。UPASANI等[37]在尸体标本上分别测试置入Osseofix系统和球囊组进行生物力学对比,通过分析表明Osseofix系统能以较少的骨水泥注入量实现较大的椎体高度复位和维持,更加符合人体脊柱的生物力学。ENDER等[38]对32例骨质疏松性椎体压缩性骨折应用Osseofix系统治疗,随访12个月表明患者疼痛症状和椎体高度改善显著,平均目测类比评分和Cobb角分别由7.7分及11.7°改善至1.4分及10.4°。有学者也同样报道了Osseofix系统的良好临床疗效,并且强调其在减少骨水泥使用量及降低术后并发症发生率的优势[39-41];GHOFRANI等[42]通过体外测试发现注入和不注入骨水泥2种状态下Osseofix系统对骨折椎体的影响差异不明显,这表明Osseofix系统并不过于依赖骨水泥的加固。 2.5 SpineJack SpineJack(法国,巴尔马)目前在欧洲已在临床上使用,但临床报道较少。SpineJack犹如千斤顶通过撑开上下推板产生支撑力,主要应用于椎体压缩性骨折的治疗,操作时通过上下推板的机械撑开作用于上下终板来复位骨折椎体,然后在椎体空腔内注入骨水泥加固[43-48]。NORIEGA等[48]在2014年进行一项前瞻性多中心观察性研究,即确定SpineJack联合使用高黏度聚甲基丙烯酸甲酯骨水泥用于治疗椎体压缩性骨折的安全性和临床疗效。在32例患者术后随访1年内,在疼痛、功能活动和生活质量方面有显著改善,除骨水泥泄漏高达30.8%之外,未发现与SpineJack相关的并发症。SpineJack被称为第3代经皮椎体扩大成形术的钛制机械装置,与经皮球囊后凸成形相比在手术时间、骨水泥使用量和术后椎体高度恢复均有较大优势[48-51]。RENAUD[52]于2015年同样报道了经皮椎弓根通道使用SpineJack结合骨水泥技术完成77例椎体压缩性骨折的微创手术,通过5年的随访表明SpineJack能提供即刻稳定性,同时可以缓解疼痛,恢复椎体功能,维持伤椎的高度及形态;虽然并发症如骨水泥渗漏的发生率与椎体后凸成形相似,但伤椎邻近椎体骨折发生率显著较低[47,53]。 2.6 KIVA系统 KIVA系统(美国,加利福尼亚州)的重要部件是通过连续螺旋环路中可拆卸的的高分子材料聚醚醚酮线圈,操作时经过椎弓根入路,在椎体垂直方向上通过叠加数个螺旋线圈来逐步抬高压缩的椎体,精准恢复椎体的高度同时提供持久的椎体高度恢复[54-55]。另外,植入物的管状和穿孔设计允许注入的骨水泥仅包含在螺旋管内部,从而防止骨水泥渗漏。OTTEN等[56-57]在临床研究中发现,KIVA系统快速缓解患者疼痛症状的效果可以与经皮椎体后凸成形相媲美。RENNER等[54]通过生物力学实验发现,KIVA不仅可在伤椎高度未完全恢复时有效提高脊柱的抗弯曲能力,且能有效矫正椎体的后凸畸形。BEALL等[55]比较了KIVA系统与经皮椎体后凸成形在治疗304例椎体压缩骨折患者时发现,与经皮椎体后凸成形相比,使用KIVA系统术后发生邻近椎体再骨折的风险降低,同时患者平均治疗费用也降低。KIVA系统操作较简便,每增加1个螺旋环路时椎体抬高约1 mm,可精确掌握椎体恢复的高度且不依赖骨水泥加固。 2.7 记忆合金椎体支架 记忆合金椎体支架(中国,苏州)的主要材料是镍钛合金,其具有复温后的形状记忆功能和超弹性的特性。刘小勇等[58]运用镍钛记忆合金的特性设计了一种记忆合金可扩张椎体支架,使支架置入椎体内利用温度而发生形变产生一定强度的支撑力,扩张塌陷椎体使其复位并产生椎体内空腔,再结合骨水泥加固椎体。但该合金支架复形的力量较有限,主要适用于新鲜的椎体压缩骨折。杨益民等[59]在压缩骨折椎体标本中对植入记忆合金椎体支架进行对比性研究,结果显示其能有效地复位支撑椎体终板,是对无神经损伤椎体骨折微创治疗的新探索。多种体外实验可以表明,镍钛记忆合金的形状记忆性良好,其力学性能和抗疲劳性较为优越,其临床有效性可与常规椎体后凸成形术相媲美[59-61]。但缺乏有效的临床数据来说明其体内长期置入的生物力学性能、骨组织长入情况以及体温反复变化对支架的影响等,有待于更深入的临床应用研究。 "

| [1] CHENG J, MUHEREMU A, ZENG X, et al. Percutaneous vertebroplasty vs balloon kyphoplasty in the treatment of newly onset osteoporotic vertebral compression fractures: A retrospective cohort study. Medicine (Baltimore). 2019;98(10): e14793. [2] LEE JK, JEONG HW, JOO IH, et al. Percutaneous balloon kyphoplasty for the treatment of very severe osteoporotic vertebral compression fractures: a case-control study. Spine J. 2018;18(6): 962-969. [3] WANG B, ZHAO CP, SONG LX, et al. Balloon kyphoplasty versus percutaneous vertebroplasty for osteoporotic vertebral compression fracture: a meta-analysis and systematic review. J Orthop Surg Res. 2018; 13(1):264. [4] QI Y, ZENG Y, JIANG C, et al. Comparison of percutaneous kyphoplasty versus modified percutaneous kyphoplasty for treatment of osteoporotic vertebral compression fractures. World Neurosurg. 2019; 122: e1020-e1027. [5] HEALTH QUALITY ONTARIO. Vertebral augmentation involving vertebroplasty or kyphoplasty for cancer-related vertebral compression fractures: a systematic review. Ont Health Technol Assess Ser. 2016; 16(11): 1-202. [6] LI Z, LIU T, YIN P, et al. The therapeutic effects of percutaneous kyphoplasty on osteoporotic vertebral compression fractures with or without intravertebral cleft. Int Orthop. 2019; 43(2): 359-365. [7] FILIPPIADIS DK, MARCIA S, MASALA S, et al. Percutaneous vertebroplasty and kyphoplasty: current status, new developments and old controversies. Cardiovasc Intervent Radiol. 2017; 40(12): 1815-1823. [8] SONG D, MENG B, CHEN G, et al. Secondary balloon kyphoplasty for new vertebral compression fracture after initial single-level balloon kyphoplasty for osteoporotic vertebral compression fracture. Eur Spine J. 2017; 26(7): 1842-1851. [9] ZHU SY, ZHONG ZM, WU Q, et al. Risk factors for bone cement leakage in percutaneous vertebroplasty: a retrospective study of four hundred and eighty five patients. Int Orthop. 2016; 40(6): 1205-1210. [10] YANG W, YANG J, LIANG M. Percutaneous vertebroplasty does not increase the incidence of new fractures in adjacent and nonadjacent vertebral bodies. Clin Spine Surg. 2019;32(2): E99-E106. [11] WANG P, LI J, SONG Z, et al. Utilization of the directional balloon technique to improve the effectiveness of percutaneous kyphoplasty in the treatment of osteoporotic vertebral compression fractures and reduction of bone cement leakage.Medicine (Baltimore). 2019; 98(19): e15272. [12] BUCHBINDER R, JOHNSTON RV, RISCHIN KJ, et al. Percutaneous vertebroplasty for osteoporotic vertebral compression fracture. Cochrane Database Syst Rev. 2018. 11: CD006349. [13] WANG E, YI H, WANG M, et al. Treatment of osteoporotic vertebral compression fractures with percutaneous kyphoplasty: a report of 196 cases. Eur J Orthop Surg Traumatol. 2013; 23(1):71-75. [14] HEINI PF, TEUSCHER R. Vertebral body stenting/stentoplasty. Swiss Med Wkly. 2012. 142: w13658. [15] LI C, ZHANG HB, ZHANG H, et al. Severe pathological fractures caused by vertebral hemangiomas with posterior decompression, bone cement augmentation and internal fixation. Orthop Traumatol Surg Res. 2016; 102(4): 489-494. [16] 袁凯,张顺聪,梁德,等.新型椎体成形带球囊支架系统在骨质疏松性椎体压缩骨折中的应用[J]. 临床外科杂志, 2019,27(8): 707-710. [17] 贾璞,陈浩,包利,等. 改良支架成形术与经皮椎体后凸成形术治疗骨质疏松性椎体压缩骨折近期疗效分析[J].临床和实验医学杂志, 2018,17(16): 1760-1763. [18] FÜRDERER S, ANDERS M, SCHWINDLING B, et al. Vertebral body stenting. A method for repositioning and augmenting vertebral compression fractures. Der Orthopde. 2002;31(4): 356-361. [19] KLEZL Z, MAJEED H, BOMMIREDDY R, et al. Early results after vertebral body stenting for fractures of the anterior column of the thoracolumbar spine. Injury. 2011;42(10): 1038-1042. [20] DIEL P, RÖDER C, PERLER G, et al. Radiographic and safety details of vertebral body stenting: results from a multicenter chart review. BMC Musculoskelet Disord. 2013;14(1): 233. [21] HARTMANN F, GRIESE M, DIETZ SO, et al. Two-year results of vertebral body stenting for the treatment of traumatic incomplete burst fractures. Minim Invasive Ther Allied Technol. 2015; 24(3): 161-166. [22] WERNER CM, OSTERHOFF G, SCHLICKEISER J, et al. Vertebral body stenting versus kyphoplasty for the treatment of osteoporotic vertebral compression fractures: a randomized trial. J Bone Joint Surg Am Vol. 2013; 95(7): 577-584. [23] FILIPPIADIS DK, MARCIA S, RYAN A, et al. New Implant-Based Technologies in the Spine. Cardiovasc Intervent Radiol. 2018; 41(10): 1463-1473. [24] KELBL M, KOČIŠ J, KOČIŠ T, et al. Assessment of reduction abilities of an expandable stent in treating osteoporosis-related fractures of Th/L (thoracolumbar) spine. Acta Chir Orthop Traumatol Cech. 2019; 86(1): 39-45. [25] RICHMOND BJ. Vertebral augmentation for osteoporotic compression fractures. J Clin Densitom. 2016; 19(1): 89-96. [26] SHEN GW, WU NQ, ZHANG N, et al. A prospective comparative study of kyphoplasty using the Jack vertebral dilator and balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. J Bone Joint Surg Br. 2010;92(9): 1282-1288. [27] 卞元健,黄永辉,谭玉辉,等. 两种不同扩张方式椎体后凸成形术的生物力学比较[J]. 江苏大学学报(医学版), 2014, 24(5):423-426. [28] LI D, HUANG Y, YANG H, et al. Jack vertebral dilator kyphoplasty for treatment of osteoporotic vertebral compression fractures. Eur J Orthop Surg Traumatol. 2014; 24(1): 15-21. [29] JIN F, SHEN Y, NING Z, et al. Evaluation of surgical outcome of Jack vertebral dilator kyphoplasty for osteoporotic vertebral compression fracture-clinical experience of 218 cases. J Orthop Surg Res. 2016; 11(1): 56. [30] SIETSMA MS, HOSMAN AJ, VERDONSCHOT NJ, et al. Biomechanical evaluation of the vertebral jack tool and the inflatable bone tamp for reduction of osteoporotic spine fractures. Spine (Phila Pa 1976). 2009;34(18): E640-E644. [31] FOO LS, YEO W, FOOK S, et al. Results, experience and technical points learnt with use of the SKy Bone Expander kyphoplasty system for osteoporotic vertebral compression fractures: a prospective study of 40 patients with a minimum of 12 months of follow-up. Eur Spine J. 2007; 16(11): 1944-1950. [32] TONG SC, ESKEY CJ, POMERANTZ SR, et al. "SKyphoplasty": a single institution's initial experience. J Vasc Interv Radiol. 2006;17(6): 1025-1030. [33] FOLMAN Y, SHABAT S. A comparison of two new technologies for percutaneous vertebral augmentation: confidence vertebroplasty vs. sky kyphoplasty. Isr Med Assoc J. 2011;13(7): 394-397. [34] XIONG J, DANG Y, JIANG BG, et al. Treatment of osteoporotic compression fracture of thoracic/lumbar vertebrae by kyphoplasty with SKY bone expander system. Chin J Traumatol. 2010;13(5): 270-274. [35] ZHENG WD, LI L, ZHAO YH. Clinical study on the vertebral plasty for the treatment of osteoporotic vertebral compressed fractures in elderly. Zhongguo Gu Shang. 2008;21(6): 405-406. [36] VANNI D, GALZIO R, KAZAKOVA A, et al. Third-generation percutaneous vertebral augmentation systems. J Spine Surg. 2016; 2(1): 13-20. [37] UPASANI VV, ROBERTSON C, LEE D, et al. Biomechanical comparison of kyphoplasty versus a titanium mesh implant with cement for stabilization of vertebral compression fractures. Spine (Phila Pa 1976). 2010;35(19): 1783-1788. [38] ENDER SA, WETTERAU E, ENDER M, et al. Percutaneous Stabilization System Osseofix® for Treatment of Osteoporotic Vertebral Compression Fractures - Clinical and Radiological Results after 12 Months. PLoS One. 2013; 8(6): e65119. [39] ESCHLER A, ROEPENACK P, ROESNER J, et al. Cementless titanium mesh fixation of osteoporotic burst fractures of the lumbar spine leads to bony healing: results of an experimental sheep model. Biomed Res Int. 2016; 2016: 4094161. [40] ENDER SA, GRADL G, ENDER M, et al. Osseofix® system for percutaneous stabilization of osteoporotic and tumorous vertebral compression fractures - clinical and radiological results after 12 months. Rofo. 2014;186(4): 380-387. [41] ESCHLER A, ENDER SA, SCHIML K, et al. Bony healing of unstable thoracolumbar burst fractures in the elderly using percutaneously applied titanium mesh cages and a transpedicular fixation system with expandable screws. PLoS One. 2015;10(2): e0117122. [42] GHOFRANI H, NUNN T, ROBERTSON C, et al. An evaluation of fracture stabilization comparing kyphoplasty and titanium mesh repair techniques for vertebral compression fractures: is bone cement necessary. Spine (Phila Pa 1976). 2010;35(16): E768-E773. [43] NORIEGA DC, RAMAJO RH, LITE IS, et al. Safety and clinical performance of kyphoplasty and SpineJack(®) procedures in the treatment of osteoporotic vertebral compression fractures: a pilot, monocentric, investigator-initiated study. Osteoporos Int. 2016; 27(6): 2047-2055. [44] NORIEGA DC, RODRΊGUEZ-MONSALVE F, RAMAJO R, et al. Correction to: Long-term safety and clinical performance of kyphoplasty and SpineJack® procedures in the treatment of osteoporotic vertebral compression fractures: a pilot, monocentric, investigator-initiated study. Osteoporos Int. 2019; 30(3): 647. [45] NORIEGA DC, RODRΊGUEZ-MONSALVE F, RAMAJO R, et al. Long-term safety and clinical performance of kyphoplasty and SpineJack® procedures in the treatment of osteoporotic vertebral compression fractures: a pilot, monocentric, investigator-initiated study. Osteoporos Int. 2019;30(3): 637-645. [46] PREMAT K, VANDE PERRE S, CORMIER É, et al. Vertebral augmentation with the SpineJack® in chronic vertebral compression fractures with major kyphosis. Eur Radiol. 2018;28(12): 4985-4991. [47] CRESPO-SANJUÁN J, ARDURA F, HERNÁNDEZ-RAMAJO R, et al. Requirements for a stable long-term result in surgical reduction of vertebral fragility fractures. World Neurosurg. 2017;105: 137-144. [48] NORIEGA D, KRÜGER A, ARDURA F, et al. Clinical outcome after the use of a new craniocaudal expandable implant for vertebral compression fracture treatment: one year results from a prospective multicentric study. Biomed Res Int. 2015: 1-7. [49] VANNI D, PANTALONE A, BIGOSSI F, et al. New perspective for third generation percutaneous vertebral augmentation procedures: Preliminary results at 12 months. J Craniovertebr Junction Spine. 2012; 3(2): 47-51. [50] ROTTER R, SCHMITT L, GIERER P, et al. Minimum cement volume required in vertebral body augmentation--A biomechanical study comparing the permanent SpineJack device and balloon kyphoplasty in traumatic fracture. Clin Biomech. 2015; 30(7):720-725. [51] JACOBSON RE, NENOV A, DUONG HD. Re-expansion of osteoporotic compression fractures using bilateral spinejack implants: early clinical experience and biomechanical considerations. Cureus. 2019;11(4): e4572. [52] RENAUD C. Treatment of vertebral compression fractures with the cranio-caudal expandable implant SpineJack(®): Technical note and outcomes in 77 consecutive patients. Orthop Traumatol Surg Res Otsr. 2015; 101(7): 857-859. [53] CASTILLO-CALCÁNEO JD, RODRIGUEZ-VALENCIA F, GARCÍA-GONZÁLEZ U. Use of spinejack device shows promising results in reducing refractures for osteoporotic vertebral compression fractures: results from a retrospective case control study. World Neurosurg. 2016;91: 623-625. [54] RENNER SM, TSITSOPOULOS PP, DIMITRIADIS AT, et al. Restoration of spinal alignment and disk mechanics following polyetheretherketone wafer kyphoplasty with StaXx FX. Am J Neuroradiol. 2011; 32(7): 1295-1300. [55] BEALL DP, OLAN WJ, KAKAD P, et al. Economic analysis of kiva VCF treatment system compared to balloon kyphoplasty using randomized kiva safety and effectiveness trial (KAST) data. Pain Physician. 2015; 18(3): E299-306. [56] OTTEN LA, BORNEMNN R, JANSEN TR, et al. Comparison of balloon kyphoplasty with the new Kiva® VCF system for the treatment of vertebral compression fractures. Pain Physician. 2013; 16(5): E505-512. [57] OLIVAREZ LM, DIPP JM, ESCAMILLA RF, et al. Vertebral augmentation treatment of painful osteoporotic compression fractures with the Kiva VCF Treatment System. SAS J. 2011; 5(4): 114-119. [58] 刘小勇,唐天驷,杨惠林. 记忆合金可扩张椎体支架椎体标本内初步影像结果分析——一种用于脊柱压缩骨折的微创动力内固定的设计[J]. 生物骨科材料与临床研究,2010,7(3): 7-10. [59] 杨益民,张智,李萌,等. 记忆合金支架在椎体骨折中的实验研究[J]. 中国微创外科杂志, 2014, 14(8): 751-754. [60] 刘小勇,杨惠林,罗宗平,等. 椎体解剖与EVS的曲变差分析[J]. 生物骨科材料与临床研究, 2015, 12(2): 12-16. [61] YU KX, CHU L, YANG JS, et al. Anterior transcorporeal approach to percutaneous endoscopic cervical diskectomy for single-level cervical intervertebral disk herniation: case series with 2-year follow-up. World Neurosurg. 2019; 122: e1345-e1353. [62] 杨升全,金正帅,张宁,等.椎体扩张器、Kyphon球囊和Sky骨膨胀器三种后凸成形术的临床应用比较研究[J].南京医科大学学报(自然科学版), 2011, 31(2):250-255. |
| [1] | Zhang Le, Pan Bin, Ruan Ruxin, Guo Kaijin. Effect of lumbopelvic sagittal parameters on secondary adjacent vertebral fracture after percutaneous kyphoplasty for osteoporotic vertebral compression fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(15): 2370-2374. |
| [2] | Jing Wanli, Zhang Tao, Teng Donghui, Shi Tao, Zhou Qiang. Poor outcomes of bone filling mesh container vertebroplasty for the treatment of osteoporotic vertebral compression fractures with vertebral body wall incompetence [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(10): 1522-1527. |
| [3] | Liu Qun, Sun Dongdong, Gao Lilan, He Zhijiang, Sun Minglin. Risk factors for fractures secondary to percutaneous kyphoplasty: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(6): 976-984. |
| [4] | Xie Xiufeng, Zhang Yue, Qu Ze. Clinical outcomes of drug-eluting balloons and drug-eluting stents for the treatment of in-stent restenosis [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(4): 555-560. |
| [5] | Li Kaiming, Wang Shangquan, Li Linghui, Zhu Liguo, Zhang Qing, Xie Rui. Bone filling bag vertebroplasty and percutaneous kyphoplasty for the treatment of thoracolumbar osteoporotic compression fractures: a meta-analysis of improving Cobb angle and reducing bone cement leakage [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(4): 650-656. |
| [6] |
Zheng Haijun, Jin Hui, Cui Hongling, Zhu Yakun, Zeng Hui, Han Fengjie, Qiu Cuiting, Liu Jing.
Safety of drug-coated balloon versus drug-eluting stents in the treatment of type 2 diabetes mellitus complicated by coronary artery small vessel disease in older adult patients [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(28): 4573-4579. |
| [7] | Li Kaiming, Zhu Liguo, Zhang Qing, Li Linghui, Xie Rui, Chen Ming, Liang Long, Lin Chengyu, Hou Xiaozhou. Zolidronic acid combined with percutaneous kyphoplasty in the treatment of osteoporotic compression fractures: a meta-analysis of bone density improvement, recurrent vertebral fractures prevention, and long-term efficacy evaluation [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(24): 3911-3917. |
| [8] | Jin Hui, Qiu Cuiting, Sun Yachao, Zeng Hui, Zheng Haijun, Liu Jing, Han Fengjie. Efficacy of cutting balloon versus semi-compliant balloon for predilation of coronary bifurcation lesions [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(22): 3540-3546. |
| [9] | Luo Wei, Chen Jianping, Sun Qianqian, Chen Chen, Li Hang, Ma Chenglong, Su Rui, Feng Xiaoyue, Sun Yurui. Facet joint injection versus percutaneous kyphoplasty for mild vertebral fragility fractures: rapid analgesia and restoration of spinal stability [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(20): 3168-3173. |
| [10] | Ren Yide, Zhang Yafeng, Li Feng, Gao Hongwen. Relationship between unilateral percutaneous kyphoplasty for treating Kummell’s disease and the amount of injected bone cement [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(16): 2467-2472. |
| [11] | Huang Tianji, Yang Shengdong, Lin Hao, Zhang Chunyang, Deng Zhongqi, Zhong Weiyang, Luo Xiaoji. Mapping knowledge domains of bibliometrics regarding percutaneous vertebroplasty and percutaneous kyphoplasty based on VOSviewer [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(15): 2410-2417. |
| [12] | Wu Bin, Bai Fenghua, Lin Mingxia, Lin Jianping. Risk factors of adjacent vertebral collapse after kyphoplasty with cement injection in older adult women [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(12): 1829-1834. |
| [13] | Luo Tedan, Jiang Xin, Zhou Chongchong, Huang Baofeng, Li Peng. Expression Foxp3 and bone morphogenetic protein 7 in rat models of carotid artery balloon injury after treated by total glucosides of paeony [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(35): 5633-5637. |
| [14] | Guo Dahua, Wang Yuhui, Ye Qianqu, Liu Wenhao, Yang Bo, Ye Linqiang. Mechanical changes of percutaneous kyphoplasty and percutaneous vertebroplasty in the treatment of thoracolumbar compressive fractures in three-dimensional vertebral models [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(32): 5146-5150. |
| [15] | Jiang Jie, Zhang Yong. Unipedicular percutaneous vertebroplasty versus percutaneous kyphoplasty bone cement for treating Kummell disease [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(22): 3481-3487. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||