Chinese Journal of Tissue Engineering Research ›› 2013, Vol. 17 ›› Issue (4): 728-735.doi: 10.3969/j.issn.2095-4344.2013.04.025
Previous Articles Next Articles
Mechanical analysis of locking compression plate fixation for the treatment of tibial fracture
Sun Xiang1, 2, Kan Shi-lian2, Yuan Tian-xiang2
- Sun Xiang1, 2, Kan Shi-lian2, Yuan Tian-xiang2
-
Received:2012-06-13Revised:2013-01-05Online:2013-01-22Published:2013-01-22 -
Contact:Sun Xiang★, Studying for master’s degree, Physician, Tianjin Medical University, Tianjin 300070, China; Tianjin Hospital, Tianjin 300211, China Edgar_x@126.com -
About author:Sun Xiang★, Studying for master’s degree, Physician, Tianjin Medical University, Tianjin 300070, China; Tianjin Hospital, Tianjin 300211, China Edgar_x@126.com
CLC Number:
Cite this article
Sun Xiang, Kan Shi-lian, Yuan Tian-xiang. Mechanical analysis of locking compression plate fixation for the treatment of tibial fracture[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(4): 728-735.
share this article
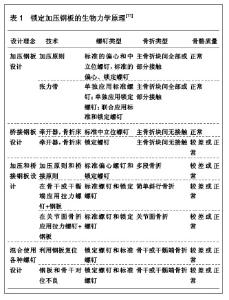
1 锁定加压钢板治疗骨折的力学原理 由于锁定加压钢板的特殊设计,可以作为标准钢板使用标准螺钉,也可以作为内固定支架使用锁定螺钉,也可以同时应用联合固定。内固定支架的力学原理基本上等同于外固定支架的力学原理。锁定加压钢板按照不同力学原理作为不同的内固定器械使用,其生物力学原理,见表1。"
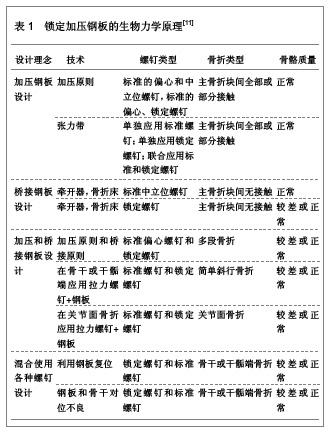
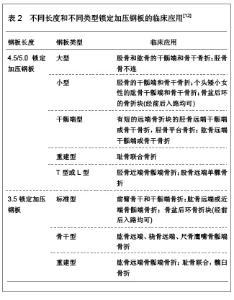
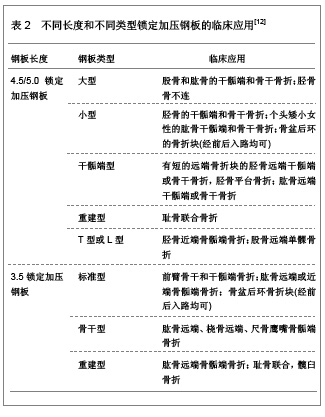
加压钢板的设计是运用了加压固定装置,通过张力带或钢板打入偏心螺钉获得动力加压均可以完成加压的作用。这种力学理念的适应证为软组织损伤小的长骨干骺端或者是骨干的简单横行骨折或斜行骨折。 桥接钢板设计技术包括内固定钢板和损伤骨折部位之间的连接。桥接钢板的稳定性取决于钢板的强度和钢板与骨之间的结合力。可以使用各种不同类型的螺钉来固定干骺端或骨干部位的粉碎性骨折。使用锁定螺钉的优势在于仅穿过单层皮质骨,可以减短螺钉的长度,以及使用自钻螺钉,不需要测量螺钉的长度。 锁定加压钢板的内固定依赖于成角稳定的钢板和螺钉界面,锁定加压钢板的内固定适用于4种原则,即加压原则、中和原则、桥接原则和结合原则,以及骨质疏松和关节周围粉碎性骨折,对于简单骨干部骨折,复位不良的骨折及关节内移位明显的骨折并不适用。 骨骼质量正常时,标准的螺钉和锁定的螺钉均可使用。在骨质疏松患者中,推荐使用双皮质骨拉力螺钉。 在钢板类型的选择方面,锁定加压钢板的横截面和力学特性与钛合金有限接触动力加压钢板一致。因此,对于特定的骨折块和骨折类型,可以使用同类型的钢板。 不同长度和不同类型锁定加压钢板的临床应用,见表2。"

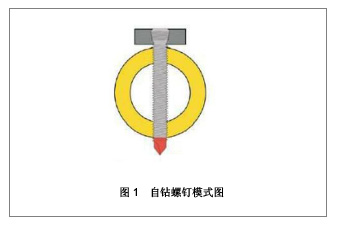
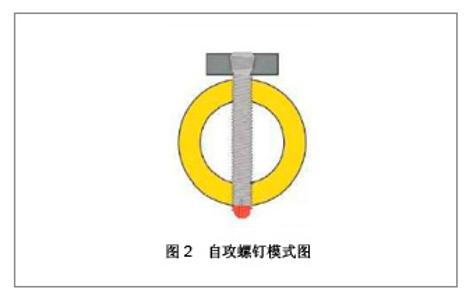
2 锁定加压钢板置入内固定治疗长骨骨折的生物力学特点 锁定加压钢板有4种不同的螺钉,分别是标准松质骨螺钉、标准皮质骨螺钉、自钻螺钉和自攻螺钉[13]。在需要调整螺钉角度,以避免进入关节腔或者使用偏心螺钉使骨折端获得加压时,应使用标准螺钉。对骨骼质量优异的长骨干骨折块应使用自钻螺钉。自钻螺钉和自攻螺钉的模式图,见图1和2。"
"
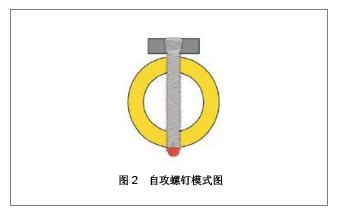
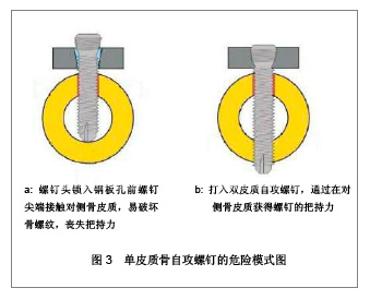
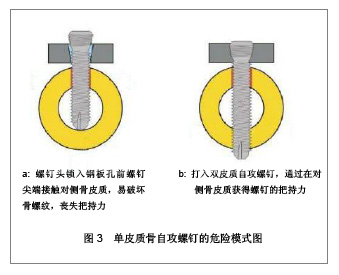
自攻螺钉可应用于骨骺端、干骺端和骨干骨折。由于没有切割头,自攻螺钉穿出对侧骨皮质的长度要短于自钻螺钉。为了在双侧骨皮质获得良好的螺钉把持力,即使是自攻螺钉也应该轻度穿过对侧骨皮质。 2.1 单皮质骨自攻螺钉的危险 对于骨骼质量优良的长骨干骨折使用自钻螺钉作为单皮质骨螺钉。当骨髓腔细小时应避免螺钉尖端损伤近端皮质的骨螺纹,因其很容易穿入对侧骨皮质。当打入单皮质自攻螺钉,螺钉帽锁定于钢板上时,如果螺钉尖端接触骨皮质,即使是最短的螺钉也会毁坏骨螺纹。如果发生类似情况,应更换为双皮质自攻螺钉至少在对侧骨皮质获得把持力[14]。单皮质骨自枚螺钉的危险模式图,见图3。"
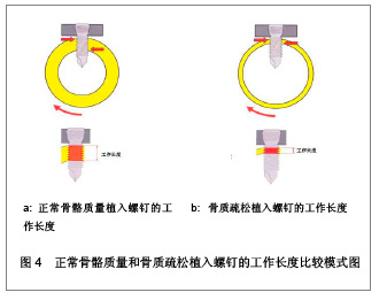
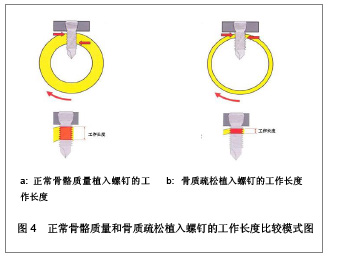
2.2 锁定加压钢板的螺钉工作长度 治疗骨质疏松时,骨皮质通常很薄,打入单皮质骨螺钉产生的工作长度减少,即使是锁定螺钉所提供的把持力也是不够的[15]。可能导致螺钉把持力的完全丧失从而引起内固定的不稳。对于所有合并骨质疏松的骨折,推荐在骨折块间使用双皮质自攻螺钉以提高螺钉工作长度,避免骨与螺钉界面的潜在问题,正常骨骼质量和骨质疏松植入螺钉的工作长度比较模式图,见图4。"
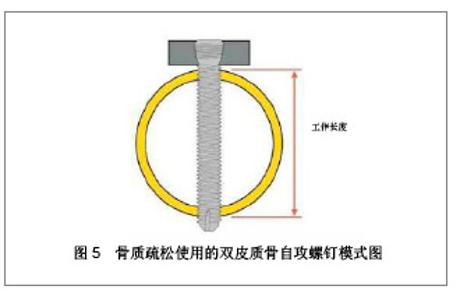
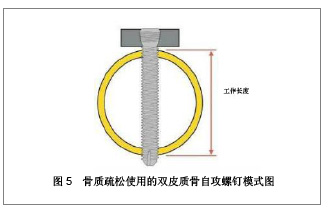
螺钉的工作长度由骨皮质的厚度决定,对于骨质疏松的骨皮质,单皮质螺钉工作长度减少,因此即使是锁定螺钉所提供的把持力也是不够的,可能导致螺钉把持力的完全丧失,从而引起内固定失效,在主要承受扭转应力的部分尤其危险。推荐在所有骨折块均使用双皮质骨自攻螺钉,以提高螺钉的工作长度。避免骨-螺纹界面潜在问题,骨质疏松使用的双皮质骨自攻螺钉模式图,见图5。"
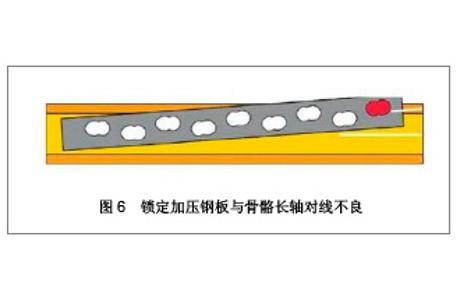
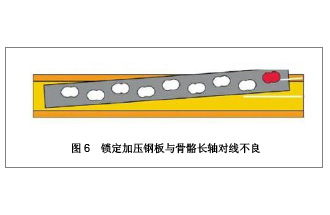
2.3 锁定加压钢板与骨骼长轴对线不良 由于螺钉头已经进入圆锥形螺纹钢板孔,在螺钉打入和拧紧时会失去对骨骼质量的感觉。当长骨轴线与钢板对线不良时,钢板远端末节经皮向骨干打入短的单皮质骨螺钉常发生危险[16],与骨骼长轴对线不良,见图6。"
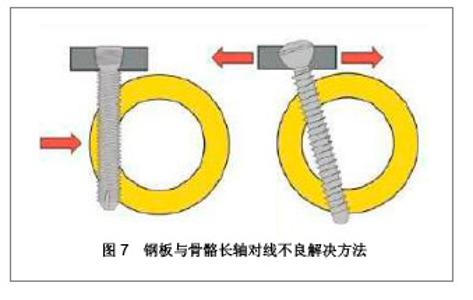
解决对线不良的方法,要么打入长自攻螺钉,要么改变角度打标准螺钉。使带钻头的中置螺钉和打入单皮质自钻螺钉前感觉到骨皮质。对线不良解决方法,见图7。"
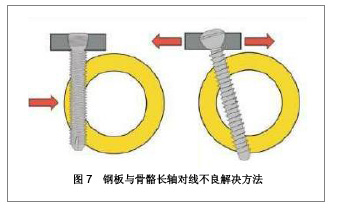
解决钢板偏心放置时单皮质自钻螺钉把持力不足的问题,可以使用长的双皮质骨自攻螺钉,也可以在钢板孔内改变角度打入标准螺钉。 2.4 锁定加压钢板长度对内固定稳定的影响 理想的内固定置入物长度取决于2个因素:钢板跨越比和钢板螺钉密度[17]。钢板跨越比是钢板长度与骨折长度的比值,粉碎性骨折中应大于2-3,对于简单骨折应大于8-9。选择短钢板以避免切割过多的皮肤和软组织。由于没有或很少的额外生物学损伤,可以只根据骨折稳定所需的力学要求来选择钢板长度。从力学方面考虑,应尽可能的降低钢板和螺钉的负荷以避免其因循环负荷导致疲劳骨折。锁定加压钢板分为3个部分,最紧靠骨折端的2颗螺钉的中间部分,获得植入物把持力的近端部分和远端部分。钢板的长度和螺钉的位置影响钢板和螺钉本身所受的应力。跨越骨折的中间部分的局部力学环境决定骨折生物学反应。 2.5 锁定加压钢板螺钉的数量和位置 如果将锁定加压钢板作为锁定内固定支架,用于桥接或微创钢板内固定技术,在骨折区两侧各使用两三枚螺钉,尤其是加压负重的胫骨。近骨折区第1个螺钉的位置及额外的螺钉取决于骨折间隙的大小,简单骨折或骨折块之间的间隙小于2 mm,一两个骨折区的螺孔不应打螺钉,以便保留骨折的微动。对于粉碎性骨折,骨折区两边各3枚螺钉,并且中间的2枚螺钉应尽可能靠近骨折区。对于强抗扭力的骨折,每个主要骨折块应打入三四枚螺钉固定。粉碎性骨折应尽可能将螺钉靠近骨折区。当骨痂形成的时候,钢板随着压力迅速降低,并且不依赖于螺钉的位置。骨折区两边各3枚螺钉,提供了足够的稳定性,并且减少置入物失败风险。为了提供足够的稳定性,最远端的2枚螺钉必须打入。在桥接钢板边上打入更多的螺钉能够提高抗扭力强度,来降低骨痂被破坏危险,螺钉数量越多,可以使钢板的锚合力增加,对于骨质疏松的患者更有效[18]。 2.6 锁定加压钢板内固定的临床适应证 锁定加压钢板既可以作为传统的加压钢板,又可作为内固定的支架使用,也可将两者结合起来。 锁定加压钢板内固定的临床适应证[19]:"
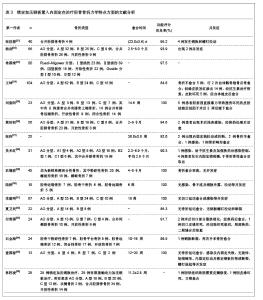
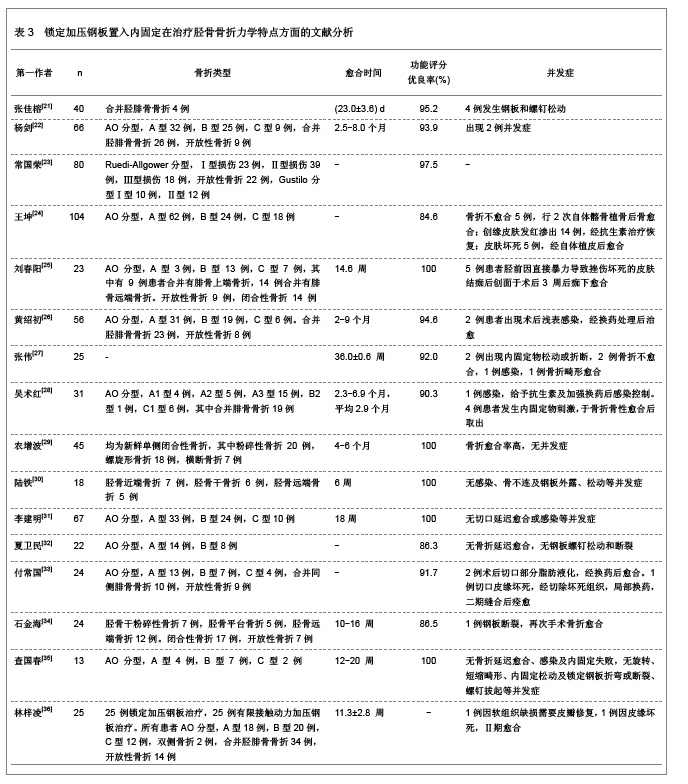
3 锁定加压钢板置入内固定治疗胫骨骨折力学特点的文献分析 3.1 资料来源 检索数据库有关锁定加压钢板置入内固定治疗胫骨骨折力学特点研究的文献[20],检索时间范围在2006至2012年,检索词为“锁定加压钢板;内固定;胫骨骨折;力学分析”,检索到相关文献152篇,结果分析相关文献16篇[21-36]。 3.2 纳入标准 ①与锁定加压钢板置入内固定治疗胫骨骨折研究相关的文献。②与经皮微创锁定加压钢板置入内固定治疗胫骨骨折研究相关的文献。 3.3 排除标准 ①重复研究、普通综述或Meta分析类文献。②将锁定加压钢板内固定作为锁定内固定处理简单骨折。③间接复位锁定固定处理移位的关节内骨折。④用传统钢板即可获得满意固定。 3.4 分析指标 ①锁定加压钢板置入内固定治疗患者的骨折类型。②锁定加压钢板置入内固定愈合时间。③锁定加压钢板置入内固定后功能评分优良率。④锁定加压钢板置入内固定后并发症。 3.5 锁定加压钢板置入内固定治疗胫骨骨折力学特点方面的文献分析 相关文献分析,见表3。"

此外,锁定加压钢板置入内固定治疗胫骨骨折的临床应用中,应注意能导致钢板内固定失败的因素。①选用钢板过短:锁定加压钢板长度对骨折内固定起到很重要的作用,如果钢板长度较短会降低钢板轴向强度和扭转强度。在简单骨折内固定时钢板长度与骨折区长度的比值要高8-10倍,在粉碎性骨折内固定时钢板长度与骨折区长度比值要高两三倍。②钢板与骨面间隙过大[37]:研究发现与骨面间隙大于5 mm时,锁定加压钢板轴向和扭转强度有所下降,小于2 mm时下降不明显,因此,锁定加压钢板与骨面间隙建议不超过2 mm。③钢板与骨骼长轴对线不良:经皮微创内固定时,锁定加压钢板的位置不容易控制,可能会发现对线不良,建议适当取小切口,术中手指触摸,将钢板引导到满意位置,克氏针辅助固定,并行X射线检查。④选用不合适的螺钉类型:对于髓腔较窄的骨干骨折,打入螺钉时很容易触及对侧的皮质骨,这样会影响螺钉和骨的把持力,应改用双皮质自攻螺钉。对于骨质疏松的患者,由于皮质较薄,螺钉的工作长度有所减少,易引起螺钉松动移位,建议改用双皮质螺钉来增加螺钉的工作长度,获得增强的骨把持力。⑤螺钉分布不均匀:锁定加压钢板的螺钉如果分布过多,会造成局部的应力集中,容易出现内固定失败。如果螺钉的分布过少,会使内固定的强度不够,也会造成内固定失败。因此,建议骨折两端的螺钉密度在40%-50%。锁定加压钢板要相对较长,并且在骨折处空出2-3个孔,使钢板具有更高的弹性,避免应力集中,增加内固定的力学平衡。⑥螺钉与钢板角度不正确:由于对锁定加压钢板的操作不熟练以及未达到功能复位要求而放置钢板很容易发生成角畸形,建议在术前制定详细的手术计划,用牵引、解剖复位以及克氏针临时固定的方法,在X射线下得到满意位置后安放钢板和螺钉。螺钉与锁定加压钢板之间的角度并不完全垂直的,存在大约5°角的目的是减少螺钉的应力,如果螺钉与钢板的角度不正确,可能破坏内固定的强度[38]。如果拧入的螺钉与锁定加压钢板的角度过大,会造成螺钉的把持力明显下降[39]。⑦患肢负重过早:锁定加压钢板在骨折内固定时是相对稳定固定,但需要有骨痂形成来实现愈合。锁定加压钢板置入后,鼓励患肢早期活动,但不易过早负重训练,应在手术6周以后逐渐进行负重练习,并且在X射线片上有明显的骨痂形成。如果患者过早和过度负重,会造成锁定加压钢板或螺钉的断裂和拔出。⑧肌腱、神经血管等损伤:经皮微创内固定技术在置入的过程中,由于不能直视皮下组织结构,需要经皮插入在肌肉组织下,使肌腱和血管神经损伤的可能性明显增加。因此,要求术者了解并熟悉骨折周围的解剖结构,保护术区肌腱和神经血管组织,要充分进行钝性分离,避免造成神经牵拉和损伤[40-41]。⑨手术切口感染:由于锁定加压钢板的宽度和厚度较大,在处理软组织较薄的骨折部位时,易造成软组织损伤,导致伤口感染[4]。因此,应把握好手术治疗时机和手术技巧,遵循骨折治疗原则,重视无菌操作,仍可能发生感染。⑩钢板外露:锁定加压钢板如复位不良,会引起钢板的放置不适宜,顶于皮下组织,如骨折区软组织条件较差或切口选择不当,可引起钢板的外露[42]。○11软组织激惹症:软组织激惹是钢板置入内固定后皮下可触及钢板以及钢板周围的疼痛,可能与钢板的体积过大或放置的位置不当有关,在胫骨远端骨折时,内踝位置的软组织较薄,易压迫皮肤软组织出现不适[43]。现在应用的新型钢板干骺远端较薄,与骨面较贴敷,边缘也较光滑,可以有效解决软组织激惹症的问题。○12锁定螺钉不易取出:锁定加压钢板由高强度的钛金属制成,在愈合过程中容易被骨痂所包裹,在螺钉取出时需要剔除骨痂,增加了螺钉取出的难度,另外,由于弃用螺钉瞄准器不但使螺钉和钢板成角不正确,还会使螺钉过度旋紧,使锁定螺钉不易取出,超过限度的扭矩或锁定螺钉与锁定孔之间的成角大于5°,则会造成螺纹破坏,以致冷焊接[44]。应使用螺钉瞄准器,使螺纹能与钢板准确锁定,也可以使用特别的扳手,控制力的大小[45]。 作者贡献:孙翔进行实验设计、实施及评估,资料收集、成文,对实验进行审校并对文章负责。 利益冲突:课题未涉及任何厂家及相关雇主或其他经济组织直接或间接的经济或利益的赞助。 伦理要求:实验获得所在单位的伦理委员会批注,符合伦理学标准。 作者声明:文章为原创作品,数据准确,内容不涉及泄密,无一稿两投,无抄袭,无内容剽窃,无作者署名争议,无与他人课题以及专利技术争执,内容真实,文责自负。"

| [1] Chakravarthy J, Bansal R, Cooper J. Locking plate osteosynthesis for Vancouver Type B1 and Type C periprosthetic fractures of femur: a report on 12 patients. Injury.2007;38(6):725-733.[2] Leung F, Chow SP. Locking compression plate in the treatment of forearm fractures: a prospective study. J Orthop Surp(Hong Kong).2006;14(3):291-294.[3] Miller DL, Goswami T. A review of locking compression plate biomechanics and their advantages as internal fixators in fracture healing. Clin Biomech(Bristol,Avon).2007;22(10):1049-1062.[4] Phisitkul P, McKinley To, Nepola JV, et al. Complications of locking plate fixation in complex proximal tibia injuries. J Orthop Trauma.2007;21(2):83-91.[5] Arora R, Lutz M, Hennerbichler A, et al. Complications following in-ternal fixation of unstable distal radius fracture with a palmar locking plate. J Orthop Trauma.2007;21(5): 316-322.[6] Chung KC, Watt AJ, Kotsis SV. Treatment of unstable distal radial fractures with the volar locking plate system. J Bone Joint Surg(Am).2006;88(12):2687-2694.[7] Rose PS, Adams CR, Torchia ME, et al. Locking plate fixation for proximal humeral fractures: initial results with a new implant. J Shoulder Elbow Surg. 2007;16(2):202-207.[8] Gautier E, Sommer C. Guidelines for the clinical application of the LCP. Injury.2003;34(2Suppl):63-76.[9] Sommer C, Babst R, Mvller M, et al. Locking compression plate loos-ening and plate breakage: a report of four cases. J Orthop Trau-ma.2004;18(8):571-577.[10] Kregor PJ, Stanard JA, Zlowodzki M, et al. Treatment of distal femur fractures using the less invasie stabilization system: surgical experience and early clinical results in 103 fractures. J Orthop Trauma.2004;18(8):509-520.[11] 丁香园. 锁定加压钢板临床应用指南(一)[DB/OL].2012-12-15. http://orthop.dxy.cn/article/10527[12] 曹清,马宝通.锁定加压钢板的临床应用[J].中国矫形外科杂志, 2008,16(12):930-931.[13] 周凤彬,潘梁.锁定加压钢板在多发性骨折中的应用[J].中外医疗,2011,30(13):44,46.[14] 刘晓辉,张国川.锁定加压钢板生物力学原理及置入后的失败分析[J].中国组织工程研究与临床康复,2011,15(4):717-720.[15] 邓仁椿,洪澜,崔华明,等.经皮微创锁定加压钢板内固定治疗胫骨远段骨折[J].中国矫形外科杂志,2010,18(8):682-684.[16] 张飞,武宇赤,李哲海,等.锁定加压钢板内固定失败原因分析[J]. 实用骨科杂志,2012,18(2):177-180.[17] 丁华文,尹生云.锁定加压钢板治疗胫骨骨折的临床观察[J].求医问药,2012,10(2):557-558.[18] 丁香园. 锁定加压钢板临床应用指南(二)[DB/OL].2012-12-15. http://orthop.dxy.cn/article/10528_2[19] 龙雨.锁定加压钢板的临床应用[J].右江民族医学院学报,2010, 25(2):243-244.[20] 中国知网.国学术期刊总库[DB/OL].2012-08-10. https://www.cnki.net[21] 张佳榕.锁定加压钢板在治疗四肢骨折中的临床价值研究[J].临床医学工程,2012,19(9):1532-1533. [22] 杨剑.锁定加压钢板治疗胫骨骨折66例临床观察[J].亚太传统医药,2012,8(9):134-135. [23] 常国荣.锁定加压钢板治疗80例胫骨骨折的疗效观察[J].经验体会,2012,10(19):118. [24] 王坤,刘德昌.微创经皮和有限切开复位锁定加压钢板治疗胫骨骨折的疗效比较[J].中国临床医学,2012,19(3):270-271. [25] 刘春阳.经皮微创锁定加压钢板治疗胫骨远端骨折[J].医药论坛杂志,2011,32(19):136-137. [26] 黄绍初,李雄,曹粉红.锁定加压钢板治疗胫骨骨折的临床分析[J].临床医学工程,2011,18(9):1396-1397. [27] 张伟,王伟,林忠勤,等.解剖型胫骨髓内钉与锁定加压钢板内固定治疗胫骨骨折不愈合的疗效比较[J].中国骨与关节损伤杂志, 2011, 26(7):633-634. [28] 吴术红,刘毅.经皮微创锁定加压钢板内固定治疗胫骨远端骨折[J].医学理论与实验,2011,24(12):1429-1431. [29] 农增波,赵利敏,赵茂盛,等.经皮微创锁定加压钢板治疗胫骨骨折45例分析[J].中国误诊学杂志,2011,11(9):2212. [30] 陆铁,周君琳,刘清和,等.锁定加压钢板微创经皮内固定治疗胫骨骨折[J].中国骨与关节损伤杂志,2011,26(2):161-162. [31] 李建明,付新民,韩丽.有限切开复位锁定加压钢板治疗胫骨骨折67例分析[J].中国误诊学杂志,2011,11(4):938. [32] 夏卫民,阮腊林,黄林.有限切开结合锁定加压钢板固定治疗胫骨远端骨折[J].内蒙古中医药,2009,28(24):72-73. [33] 付常国,刘国华,宋自昌.锁定加压钢板治疗胫骨远端骨折[J].实用骨科杂志,2009,15(4):298-300. [34] 石金海,刘家瑞,蔡新良,等.锁定加压钢板内固定治疗胫骨骨折的疗效[J].实用临床医学,2008,9(12):52-54. [35] 查国春,陈泽林,齐小波.经皮微创锁定加压钢板内固定治疗胫骨骨折[J].中国修复重建外科杂志,2008,22(12):1448-1450. [36] 林梓凌,黄枫,郑晓辉,等.锁定加压钢板在胫骨干骨折治疗中的应用研究和探讨[J].中国中医骨伤科杂志,2006,14(5):1-3.[37] Ahmad M, Nanda R, Bajwa AS, et al.Biomechanical testing of the locking compression plate: when does the distance between bone and implant significantly reduce construct stability?Injury. 2007; 38(3):358-364.[38] Sommer C, Gautier E, Müller M, et al.First clinical results of the Locking Compression Plate (LCP).Injury. 2003;34 Suppl 2: B43-54.[39] Kääb MJ, Frenk A, Schmeling A,et al.Locked internal fixator: sensitivity of screw/plate stability to the correct insertion angle of the screw.J Orthop Trauma. 2004;18(8):483-487.[40] 彭朝华,杨彬,邹秋富,等.微创锁定加压钢板固定术中失误及术后早期并发症分析[J].四川医学,2012,33(6):965-967.[41] 张富军,杨昊,李靖,等.微创经皮钢板固定技术前置锁定加压钢板治疗肱骨中下段骨折[J]. 中国临床研究,2011,24(10):879-881.[42] Namazi H, Mozaffarian K.Awful considerations with LCP instrumentation: a new pitfall.Arch Orthop Trauma Surg. 2007; 127(7):573-575.[43] Hasenboehler E, Rikli D, Babst R.Locking compression plate with minimally invasive plate osteosynthesis in diaphyseal and distal tibial fracture: a retrospective study of 32 patients. Injury. 2007;38(3):365-370.[44] Smith WR, Ziran BH, Anglen JO, et al. Locking plates: tips and tricks. J Bone Joint Surg Am. 2007;89(10):2298-2307.[45] Ehlinger M, Adam P, Simon P, et al.Technical difficulties in hardware removal in titanium compression plates with locking screws.Orthop Traumatol Surg Res. 2009;95(5):373-376. |
| [1] | Xu Feng, Kang Hui, Wei Tanjun, Xi Jintao. Biomechanical analysis of different fixation methods of pedicle screws for thoracolumbar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1313-1317. |
| [2] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [3] | Chen Xinmin, Li Wenbiao, Xiong Kaikai, Xiong Xiaoyan, Zheng Liqin, Li Musheng, Zheng Yongze, Lin Ziling. Type A3.3 femoral intertrochanteric fracture with augmented proximal femoral nail anti-rotation in the elderly: finite element analysis of the optimal amount of bone cement [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1404-1409. |
| [4] | Du Xiupeng, Yang Zhaohui. Effect of degree of initial deformity of impacted femoral neck fractures under 65 years of age on femoral neck shortening [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1410-1416. |
| [5] | Zhang Shangpu, Ju Xiaodong, Song Hengyi, Dong Zhi, Wang Chen, Sun Guodong. Arthroscopic suture bridge technique with suture anchor in the treatment of acromioclavicular dislocation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1417-1422. |
| [6] | Yuan Jiawei, Zhang Haitao, Jie Ke, Cao Houran, Zeng Yirong. Underlying targets and mechanism of Taohong Siwu Decoction in prosthetic joint infection on network pharmacology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1428-1433. |
| [7] | Zhou Jihui, Li Xinzhi, Zhou You, Huang Wei, Chen Wenyao. Multiple problems in the selection of implants for patellar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1440-1445. |
| [8] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [9] | Hu Kai, Qiao Xiaohong, Zhang Yonghong, Wang Dong, Qin Sihe. Treatment of displaced intra-articular calcaneal fractures with cannulated screws and plates: a meta-analysis of 15 randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1465-1470. |
| [10] | Jiang Hongying, Zhu Liang, Yu Xi, Huang Jing, Xiang Xiaona, Lan Zhengyan, He Hongchen. Effect of platelet-rich plasma on pressure ulcers after spinal cord injury [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1149-1153. |
| [11] | Li Cai, Zhao Ting, Tan Ge, Zheng Yulin, Zhang Ruonan, Wu Yan, Tang Junming. Platelet-derived growth factor-BB promotes proliferation, differentiation and migration of skeletal muscle myoblast [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1050-1055. |
| [12] | He Li, Tian Wei, Xu Song, Zhao Xiaoyu, Miao Jun, Jia Jian. Factors influencing the efficacy of lumbopelvic internal fixation in the treatment of traumatic spinopelvic dissociation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 884-889. |
| [13] | Yang Weiqiang, Ding Tong, Yang Weike, Jiang Zhengang. Combined variable stress plate internal fixation affects changes of bone histiocyte function and bone mineral density at the fractured end of goat femur [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 890-894. |
| [14] | Zhang Lei, Ma Li, Fu Shijie, Zhou Xin, Yu Lin, Guo Xiaoguang. Arthroscopic treatment of greater tuberosity avulsion fractures with anterior shoulder dislocation using the double-row suture anchor technique [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 895-900. |
| [15] | Yuan Xinping, Shao Yanbo, Wu Chao, Wang Jianling, Tong Liangcheng, Li Ying. Accuracy of target bone segments in personalized differential modeling and simulation of CT scanning parameters at fracture end [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 912-916. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||