Chinese Journal of Tissue Engineering Research ›› 2024, Vol. 28 ›› Issue (33): 5357-5363.doi: 10.12307/2024.666
Previous Articles Next Articles
Subcutaneous endplate bone graft reduction combined with percutaneous pedicle screw fixation for A3+B2 thoracolumbar burst fractures
Sun Houjie1, Han Jianhua1, Cai Xiaojun1, Li Daijun1, Fan Rui2
- 1Department of Spinal Surgery, Zunyi First People’s Hospital and Third Affiliated Hospital of Zunyi Medical University, Zunyi 563000, Guizhou Province, China; 2Zunyi Medical University, Zunyi 563000, Guizhou Province, China
-
Received:2023-08-02Accepted:2023-10-12Online:2024-11-28Published:2024-01-30 -
Contact:Sun Houjie, Master, Chief physician, Department of Spinal Surgery, Zunyi First People’s Hospital and Third Affiliated Hospital of Zunyi Medical University, Zunyi 563000, Guizhou Province, China -
About author:Sun Houjie, Master, Chief physician, Department of Spinal Surgery, Zunyi First People’s Hospital and Third Affiliated Hospital of Zunyi Medical University, Zunyi 563000, Guizhou Province, China -
Supported by:Zunyi Science and Technology Plan Project, No. HZ(2019)162 (to SHJ)
CLC Number:
Cite this article
Sun Houjie, Han Jianhua, Cai Xiaojun, Li Daijun, Fan Rui. Subcutaneous endplate bone graft reduction combined with percutaneous pedicle screw fixation for A3+B2 thoracolumbar burst fractures[J]. Chinese Journal of Tissue Engineering Research, 2024, 28(33): 5357-5363.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
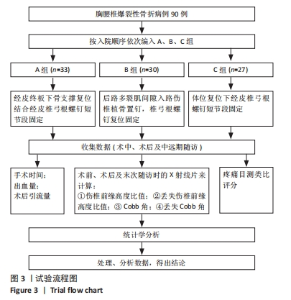
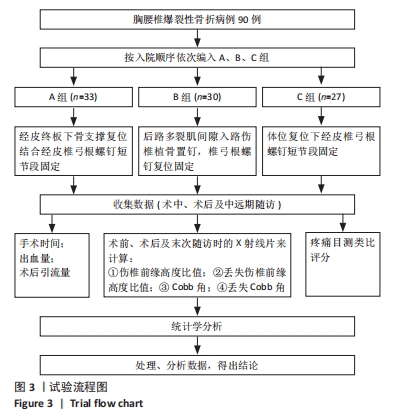
2.1 参与者数量分析 纳入胸腰椎爆裂骨折患者90例,A组33例,B组30例,C组27例;均完成18个月以上随访,全部进入结果分析,无丢失病例。 2.2 试验流程图 见图3。"

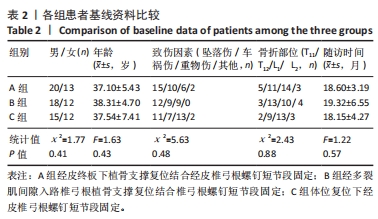
2.3 基线资料比较 3组患者基线资料比较,差异无显著性意义,具有可比性,见表2。"
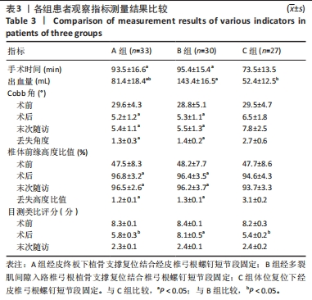
2.4 临床疗效分析 3组病例术前Cobb角、椎体前缘高度比值及目测类比疼痛评分方面无显著性差异(P > 0.05);C组手术时间比A、B组少,术中出血量A、C组较B组少,且差异均有显著性意义(P < 0.05)。见表3。"
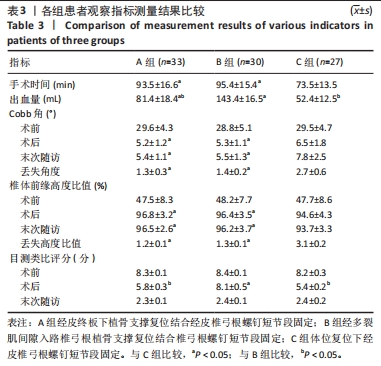

所有患者伤口均Ⅰ期愈合。末次随访时所有患者无神经功能损害,无明显腰背后凸畸形及顽固性腰背部疼痛。术后A、B组Cobb角、椎体前缘高度优于C组(P < 0.05);末次随访时A、B组优于C组(P < 0.05),A、B组间比较差异无显著性意义(P > 0.05);末次随访时丢失Cobb角、椎体前缘高度A、B组小于C组(P < 0.05),A、B组间比较差异无显著性意义(P > 0.05)。术后患者目测类比评分A、C组优于B组(P < 0.05),末次随访时3组间比较差异无显著性意义(P > 0.05)。见表3。 2.5 不良事件 C组1例患者术后1个月复查内固定松动移位,椎体高度再次丢失伴背痛,经严格卧床6周,椎体高度丢失无加重,疼痛缓解,1年后取出内固定,末次随访高度丢失无加重,发生率为4%;A组患者影像学检查伤椎终板骨折全部愈合,未见内固定松动失败;B组患者无伤椎高度丢失,无内固定松动、断裂等并发症。 2.6 植入物与宿主的生物相容性 山东威高公司生产的SINO带可折断尾部的万向长尾椎弓根螺钉、GB12-2椎弓根螺钉脊柱内固定系统和四川国纳科技有限公司生产的n-HA/PA66人工合成骨材料生物相容性好,患者未出现植入物周围感染、过敏反应、免疫反应及排斥反应等。"

| [1] TRUNGU S, RICCIARDI L, FORCATO S. Percutaneous pedicle screw fixation without arthrodesis of 368 thoracolumbar fractures: long-term clinical and radiological outcomes in a single institution. Eur Spine J. 2023;32(1):75-83. [2] BUTLER AJ, COLMAN MW, LYNCH J, et al. Augmented reality in minimally invasive spine surgery: early efficiency and complications of percutaneous pedicle screw instrumentation. Spine J. 2023;23(1):27-33. [3] NORIEGA DC, CRESPO-SANJUAN J, OLAN WJ, et al. Treatment of Thoracolumbar Type A3 Fractures Using a Percutaneous Intravertebral Expandable Titanium Implant: Long-term Follow-up Results of a Pilot Single Center Study. Pain Physician. 2021;24(5):E631-E638. [4] TRUNGU S, RICCIARDI L, FORCATO S, et al. Percutaneous pedicle screw fixation without arthrodesis of 368 thoracolumbar fractures: long-term clinical and radiological outcomes in a single institution. Eur Spine J. 2023;32(1):75-83. [5] XU J,LIU C,LIN Y, et al. Microscopic minimally invasive keyhole technique for surgical resection of spinal dumbbell tumors. World Neurosurg. 2018;109:e110-e117. [6] MOON MS, YU CG, JEON JM, et al. Usefulness of Percutaneous Pedicle Screw Fixation for Treatment of Lower Lumbar Burst (A3-A4) Fractures: Comparative Study with Thoracolumbar Junction Fractures. Indian J Orthop. 2023;57(9):1415-1422. [7] KUMAR N, CHIN BZ, CHUA CXK, et al. Unipedicular-Screw Index Vertebra Manipulation Technique for Minimally Invasive Short-Segment Thoracolumbar Fracture Fixation. Int J Spine Surg. 2023:8524. [8] MARTIN-SOMOZA FJ, CANTERO ESCRIBANO JM, RAMIREZ-VILLAESCUSA JV. Long-Term Reliability of the Two-Segment Fusion Technique in the Treatment of Thoracolumbar Fractures Using Screws in the Fractured Vertebra. Int J Spine Surg. 2021;15(1):169-178. [9] 付建仲,冯慧峰.后路椎弓根内固定术联合椎体成形术治疗老年胸腰段脊柱骨折疗效分析[J].中国烧伤创疡杂志,2022,34(6):418-421. [10] WANG H, ZHANG L, DU H, et al. Efficacy and Safety Evaluation of Bilateral Pedicle Approach Combined with Positional Reduction for the Treatment of Osteoporotic Thoracolumbar Burst Fractures. Altern Ther Health Med. 2023;29(6):176-181. [11] KOCIS J, KELBL M, KOCIS T, et al. Percutaneous versus open pedicle screw fixation for treatment of type A thoracolumbar fractures. Eur J Trauma Emerg Surg. 2020;46(1):147-152. [12] 尹稳,焦伟,于海洋.经皮椎弓根螺钉置钉辅助技术及应用进展[J].中国脊柱脊髓杂志,2022,32(8):743-747. [13] KANNO H, AIZAWA T, HASHIMOTO K, et al. Enhancing percutaneous pedicle screw fixation with hydroxyapatite granules: A biomechanical study using an osteoporotic bone model. PLoS One. 2019;14(9):e0223106. [14] ANANIA CD, BONO BC, TROPEANO M, et al. Single-Stage Posterior Transpedicular Corpectomy and 360-Degree Reconstruction for Thoracic and Lumbar Burst Fractures: Technical Nuances and Outcomes. J Neurol Surg A Cent Eur Neurosurg. 2023;84(5):489-497. [15] SUBRAMANIAN P, RAMACHANDRAN K, ARUMUGAM T, et al. Evaluation of Disc and Endplate Degeneration in AO Type A Fractures Using Magnetic Resonance Imaging Analysis. World Neurosurg. 2023:S1878-8750(23)01107-5. [16] XU C, BAI X, RUAN D, et al. Comparative finite element analysis of posterior short segment fixation constructs with or without intermediate screws in the fractured vertebrae for the treatment of type a thoracolumbar fracture. Comput Methods Biomech Biomed Engin. 2023:1-12. [17] WANG P, HU X. Biomechanical finite element analysis of superior endplate collapse after thoracolumbar fracture surgery. Ann Transl Med. 2020;8(12):753. [18] 孙家安,李亚男,王肖虎,等.经皮椎体成形术治疗老年胸腰椎骨折对患者手术创伤程度及脊柱功能的影响[J].中国老年学杂志, 2023,43(2):318-321. [19] 高志祥,肖聪,杨红涛,等.胸腰椎爆裂骨折伴神经损伤围术期隐性失血的统计学决策树模型分析[J].中国组织工程研究,2021, 25(15):2364-2369. [20] 刘凌,孙佳佳,季一鸣,等.伤椎置钉短节段固定韧带复合体损伤胸腰椎骨折[J].中国矫形外科杂志,2020,28(22):2060-2064. [21] 王子奡,宋文慧,刘昌文.胸腰椎爆裂骨折短节段固定:方法改良及减少失败的策略[J].中国组织工程研究,2021,25(24):3902-3907. [22] 韩雪昆,任永信,张慰.经皮伤椎置钉植骨治疗胸腰椎骨折疗效观察[J].南京医科大学学报(自然科学版),2020,40(1):115-118. [23] 赵继荣,王兴盛,邓强,等.微创经皮椎弓根螺钉联合经伤椎植骨固定治疗胸腰椎骨折42例[J].中国微创外科杂志,2017,17(12): 1112-1116. [24] CHEN L, LIU H, HONG Y, et al. Minimally Invasive Decompression and Intracorporeal Bone Grafting Combined with Temporary Percutaneous Short-Segment Pedicle Screw Fixation for Treatment of Thoracolumbar Burst Fracture with Neurological Deficits. World Neurosurg. 2020;135: e209-e220. [25] TOYONE T, TANAKA T, KATO D, et al. The treatment of acute thoracolumbar burst fractures with transpedicular intracorporeal hydroxyapatite grafting following indirect reduction and pedicle screw fixation: a prospective study. Spine (Phila Pa 1976). 2006;31(7): E208-E214. [26] 邵建树,刘伟峰,叶维,等.经椎弓根椎体内植骨联合短节段固定治疗老年脊柱骨折临床效果及对预后的影响[J].中国老年学杂志, 2022,42(20):5001-5004. [27] CIRILLO JI, FARIAS I, DEL PINO C, et al. Surgical timing prevails as the main factor over morphologic characteristics in the reduction by ligamentotaxis of thoracolumbar burst fractures. BMC Surg. 2023; 23(1):166. [28] LIMTHONGKUL W, WANNARATSIRI N, SUKJAMSRI C, et al. Biomechanical Comparison Between Posterior Long-Segment Fixation, Short-Segment Fixation, and Short-Segment Fixation With Intermediate Screws for the Treatment of Thoracolumbar Burst Fracture: A Finite Element Analysis. Int J Spine Surg. 2023;17(3):442-448. [29] ALANDER DH, CUI S. Percutaneous Pedicle Screw Stabilization: Surgical Technique, Fracture Reduction, and Review of Current Spine Trauma Applications. J Am Acad Orthop Surg. 2018;26(7):231-240. [30] ZOU P, YANG J, WANG X, et al. Comparison of Clinical and Radiologic Outcome Between Mini-Open Wiltse Approach and Fluoroscopic-Guided Percutaneous Pedicle Screw Placement: A Randomized Controlled Trial. World Neurosurg . 2020:144:e368-e375. [31] CHEN ZD, WU J, YAO XT, et al. Comparison of Wiltse’s paraspinal approach and open book laminectomy for thoracolumbar burst fractures with greenstick lamina fractures: a randomized controlled trial. J Orthop Surg Res. 2018;13(1):43. [32] WANG F, NAN L, FENG X, et al. The efficacy and safety of multiple-dose intravenous tranexamic acid in reducing perioperative blood loss in patients with thoracolumbar burst fracture. Clin Neurol Neurosurg. 2020:193:105766. [33] 丁其瑞,凡进,任永信,等.经皮椎弓根螺钉短节段固定结合不同经伤椎椎体内植骨方法治疗胸腰椎骨折的早期疗效比较[J].中国修复重建外科杂志,2021,35(10):1311-1317. [34] GONZALES-PORTILLO GS, MAMARIL-DAVIS JC, RIORDAN K, et al. Evaluation of the Thoracolumbar Injury Classification and Severity (TLICS) Score Over a Two-Year Period at a Level One Trauma Center. Cureus. 2023;15(8):e43762. [35] NISHIDA N, SUZUKI H, JIANG F, et al. Posterior Fixation for Different Thoracic-Sacrum Alignments Containing a Thoracolumbar Vertebral Fracture: A Finite Element Analysis. World Neurosurg. 2023:S1878-8750(23)00922-1. [36] SCHNAKE KJ, SCHROEDER GD, VACCARO AR. AO Spine Classification Systems (Subaxial, Thoracolumbar). J Orthop Trauma. 2017;31 Suppl 4:S14-S23. [37] TIAN D, ZHONG H, ZHU B, et al. Unilateral biportal endoscopic technique combined with percutaneous transpedicular screw fixation for thoracolumbar burst fractures with neurological symptoms: technical note and preliminary report. J Orthop Surg Res. 2023; 18(1):584. [38] WEI H, HSU D, KATTA H, et al. Safety and Effectiveness of Expandable Intravertebral Implant Use for Thoracolumbar Burst Fractures. J Vasc Interv Radiol. 2023;34(8):1409-1415. [39] ZENG Z, ZHANG D, ZENG FL, et al. Posterior unilateral small fenestration of lamina combined with a custom-made Y-shaped fracture reduction device for the treatment of severe thoracolumbar burst fracture: a prospective comparative study. J Orthop Surg Res. 2023;18(1):529. [40] KUMAR N, CHIN BZ, CHUA CXK, et al. Unipedicular-Screw Index Vertebra Manipulation Technique for Minimally Invasive Short-Segment Thoracolumbar Fracture Fixation. Int J Spine Surg. 2023: 17(5):652-660. [41] 朱福良,郑道明,时宇博,等.后路钉棒反弓折顶技术结合椎弓根植骨治疗胸腰段椎体爆裂骨折[J].中国组织工程研究,2020,24(12): 1817-1822. [42] PARAJÓN A, ALIMI M, NAVARRO-RAMIREZ R, et al. Minimally Invasive Transforaminal Lumbar Interbody Fusion: Meta-analysis of the Fusion Rates. What is the Optimal Graft Material? Neurosurgery. 2017;81(6): 958-971. [43] 徐世财,马飞,唐超,等.纳米羟基磷灰石/聚酰胺66椎间融合器形状对颈椎前路融合效果的影响[J].中国组织工程研究,2023, 27(30):4830-4835. [44] ZHAO J, ZHAO X, YANG L, et al. Percutaneous vertebroplasty with granulated allogeneic bone grafting using screw-view model of navigation for thoracolumbar compressive fracture: A case report. Medicine (Baltimore). 2019;98(20):e15715. [45] KONG D, SHI Y, GAO Y, et al. Preparation of BMP-2 loaded MPEG-PCL microspheres and evaluation of their bone repair properties. Biomed Pharmacother. 2020;130:110516. [46] OUCHIDA J, KANEMURA T, SATAKE K, et al. True accuracy of percutaneous pedicle screw placement in thoracic and lumbar spinal fixation with a CT-based navigation system:Intraoperative and postoperative assessment of 763 percutaneous pedicle screws. J Clin Neurosci. 2020;79:1-6. [47] HU B, WANG L, SONG Y, et al. Long-term outcomes of the nano-hydroxyapatite/polyamide-66 cage versus the titanium mesh cage for anterior reconstruction of thoracic and lumbar corpectomy: a retrospective study with at least 7 years of follow-up. J Orthop Surg Res. 2023;18(1):482. |
| [1] | Yu Zhaoyu, Tan Lixin, Sun Kai, Lu Yao, Li Yong. Meta-analysis of cement-augmented pedicle screw for thoracolumbar degenerative diseases with osteoporosis [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(5): 813-820. |
| [2] | Kong Dewei, Song Chao, Wu Liang, Wu Ming, Gong Lulu, Wang Jiaqi, Pan Hongyuan, Fan Xinbin, Zhang Yan. Finite element analysis of three-dimensional frame screws and minimally invasive plate for fixation of Sanders III calcaneal fractures [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(33): 5289-5294. |
| [3] | Tang Long, Zheng Jiazhuang, Wang Fandong, Liu Yuanbin, Song Zhaojun, Zhang Zhi, Wang Miao, Zhou Yong, Liu Huiyi, Chen Yu. Uniaxial endoscopic intervertebral fusion combined with pedicle screw fixation in treatment of lumbar degenerative diseases [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(24): 3873-3878. |
| [4] | Liu Wendong, Xia Hongle, Liu Lin, Shen Runbin, Guo Wei, Wang Xuyang, Li Guoliang. Three-dimensional digital model-assisted minimally invasive needle penetration and steel plate internal fixation in treatment of Sanders types II and III calcaneal fractures [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(18): 2819-2824. |
| [5] | Hao Shuai, Ma Xun, Zhang Yannan, Zhao Haoliang, Liu Qingqing. Morphological classification of CT reconstruction of the narrowest part of pediculoisthmic component [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(18): 2876-2880. |
| [6] | Li Tusheng, Ding Yu, Jiang Qiang, Zhang Hanshuo, Liu Jiang. Percutaneous transforaminal endoscopic discectomy combined with platelet-rich plasma in treatment of lumbar disc herniation [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(15): 2385-2390. |
| [7] | Chen Liuxu, Yang Han, Yang Jian, Yang Linyu, Kang Jianping. Finite element analysis of lumbar vertebra biomechanics after transforaminal lumbar interbody fusion combined with bilateral transpedicular transdiscal lumbar screw fixation [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(12): 1815-1822. |
| [8] | Wan Jian, Wang Ning, Bei Chaoyong, Chen Yuanming, Wang Honggang. Two lumbar fusion regimens in treatment of single-level lumbar degenerative diseases based on propensity score matching [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(12): 1914-1919. |
| [9] | Liu Jinyu, Zhang Hanshuo, Cui Hongpeng, Pan Lingzhi, Zhao Boran, Li Fei, Ding Yu. Finite element biomechanical analysis of minimally invasive treatment of cervical spondylotic myelopathy and accurate exercise rehabilitation [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(9): 1359-1364. |
| [10] | Zhou Changjun, Long Shengli, Zou Wei, Xiao Jie, Long Hao, Feng Mingxing, Zhang Yang, Liu Jie, Zeng Zhongwei. Design and clinical application of coplanar screw guide for percutaneous pedicle screw in the treatment of thoracolumbar fracture [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 534-538. |
| [11] | Bao Kai, Song Wenhui, Liu Changwen, Liang Kaiheng, Wang Jiajia. Posterior single-segment pedicle screw fixation for unstable atlas fractures [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 594-599. |
| [12] | Xin Xiaoming, Gao Mingxuan, Zhang Fan, Chi Fei, Feng Junchao, Luo Wenyuan. Application of orthopedic robot-assisted screw placement in the correction of adolescent idiopathic scoliosis [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(36): 5790-5794. |
| [13] | Wang Ziyang, Zuo Enjun. Application of biological materials in vital pulp therapy [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(3): 427-433. |
| [14] | Chen Xiao, He Binbin, Zhou Youliang, Zhao Liang, Zhang Xinguo, Jiang Ziyun, Shen Zhe. Comparison of reduction strength between long-arm single-axis pedicle screw fixation and single-plane pedicle screw fixation in the treatment of traumatic thoracolumbar fractures [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(29): 4641-4646. |
| [15] | Jin Xinjie, Lu Xiangdong, Zhao Yibo, Zhao Xiaofeng, Qi Detai, Zhao Bin. Endoscopic transforaminal lumbar interbody fusion for degenerative diseases of the lumbar spine: decompression fusion and preservation of posterior spine anatomy [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(27): 4401-4407. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||