Chinese Journal of Tissue Engineering Research ›› 2022, Vol. 26 ›› Issue (36): 5849-5856.doi: 10.12307/2022.791
Previous Articles Next Articles
Implant-related errors and complications in medial open-wedge high tibial osteotomy
Pan Jianke1, Zhao Di1, 2, Jin Xiao3, Yang Weiyi1, Luo Minghui1, Liu Jun1, 2, 4, 5, Han Yanhong1, Cao Houran1
- 1Department of Sports Medicine, Second Affiliated Hospital, Guangzhou University of Chinese Medicine, Guangzhou 510120; 2Bone and Joint Degeneration and Injury Research Team, Guangzhou 510120; 3Department of Chinese Medicine, First Affiliated Hospital of Jinan University, Guangzhou 510632; 4Guangdong Second Traditional Chinese Medicine Hospital, Guangzhou 510095; 5Fifth Clinical Medical College of Guangzhou University of Chinese Medicine, Guangzhou 510405
-
Received:2021-08-24Accepted:2021-12-07Online:2022-12-28Published:2022-04-27 -
Contact:Yang Weiyi, Chief physician, Professor, Master’s supervisor, Department of Sports Medicine, Second Affiliated Hospital, Guangzhou University of Chinese Medicine & Guangdong Provincial Hospital of Chinese Medicine, Guangzhou 510120, Guangdong Province, China -
About author:Pan Jianke, MD, Associate chief physician, Department of Sports Medicine, Second Affiliated Hospital, Guangzhou University of Chinese Medicine & Guangdong Provincial Hospital of Chinese Medicine, Guangzhou 510120, Guangdong Province, China -
Supported by:The Ministry of Industry and Information Technology and the National Health and Family Planning Commission “Orthopedic Surgery Robot Application Center” Construction Project, No. 2017MHDOSR1008 (to LJ); Guangdong Provincial Department of Finance Project (Management System of Traditional Chinese Medicine for Middle-Aged and Elderly Degenerative Knee Osteoarthritis, No. [2014]157; Traditional Characteristic Therapy Inheritance and Innovation Research of Traditional Chinese Medicine Orthopedics and Traumatology, No. [2018]8) (to LJ); Science and Technology Special Research of Guangdong Provincial Hospital of Traditional Chinese Medicine (Clinical Experience Inheritance Research of Lingnan Traumatology Famous Traumatology Experts, No. YK2013B2N19; Systematic Review of Clinical Studies of Traditional Chinese Medicine in the Treatment of Osteoarthritis and its GRADE Evidence Quality Evaluation Study, No. YN2015MS15 (to LJ)
CLC Number:
Cite this article
Pan Jianke, Zhao Di, Jin Xiao, Yang Weiyi, Luo Minghui, Liu Jun, Han Yanhong, Cao Houran. Implant-related errors and complications in medial open-wedge high tibial osteotomy[J]. Chinese Journal of Tissue Engineering Research, 2022, 26(36): 5849-5856.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
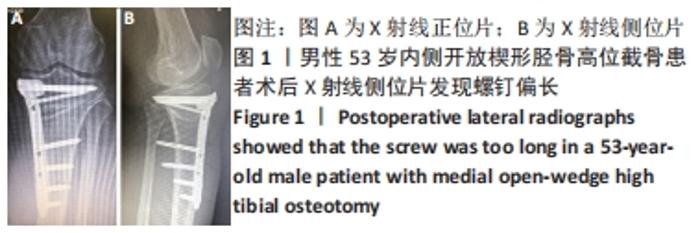
2.1 螺钉选择偏短或偏长 男性患者,53岁,影像学图片见图1。出现的原因:术者经验不足,术中未行X射线侧位片的透视,或X射线侧位片透视时下肢存在旋转影响判断。避免此项失误的措施是正确使用测深尺或术中拍摄标准的膝关节X射线正侧位片。"
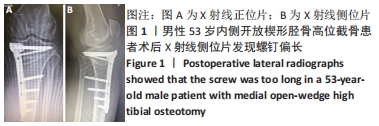
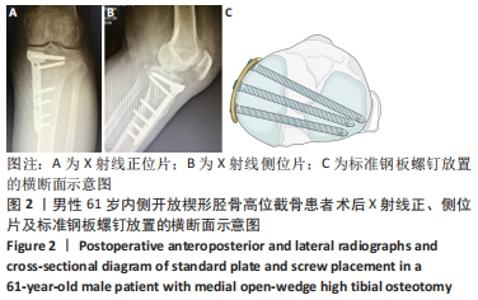
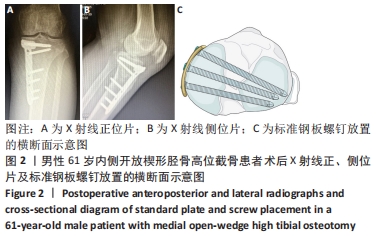
2.2 钢板放置偏前 男性患者,61岁,影像学图片见图2。出现的原因:钢板的近端放置过于偏前,容易导致近端的A、B、C孔的螺钉偏短(术中标准X射线正位片显示近端螺钉的长度未抵达外侧胫骨平台中央时,需考虑螺钉偏短的可能性),近端钢板的支撑和螺钉把持力会稍减弱,术后应避免激进的康复方案,在外侧合页完好的情况下,术后第1个月应以1/3负重为主,1个月后再从1/3负重过渡到完全负重。为防止钢板放置偏前,可使用3D打印个体化截骨导板进行钢板定位,或使用克氏针临时固定钢板时,把钢板近端尽量靠近胫骨内后方,同时让助手固定钢板的下方,避免钢板下方突出胫骨前缘激惹皮肤。"
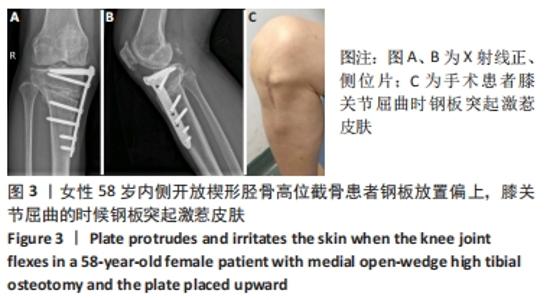
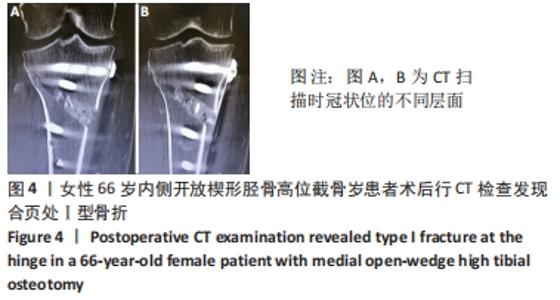
2.3 钢板放置偏上 女性患者,58岁,影像学图片见图3。正常钢板的位置其近端平行于内侧关节面,位于关节面下方5-10 mm,截骨线位于钢板的无孔区,是钢板最坚强的位置。出现钢板放置偏上的原因:截骨线偏上,或单纯失误将钢板放置偏上。在膝关节伸屈活动时,钢板容易刺激皮肤,引起内侧关节间隙的疼痛。另外,此例病例还存在钢板与胫骨贴合度差的问题,也加剧了对皮肤的刺激。建议截骨线应该放在内侧胫骨平台下方4 cm的位置,如果放在内侧胫骨平台下方3.5 cm处容易导致截骨线偏上,另外临床上身材矮小的患者容易出现将截骨线放置偏上的情况。"
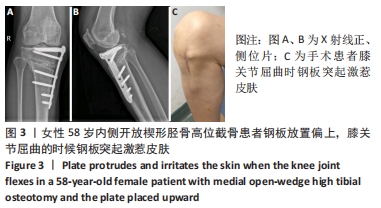
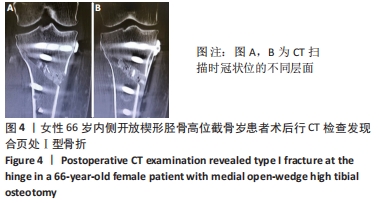
2.4 合页骨折 2.4.1 Ⅰ型合页骨折 女性患者,66岁。Ⅰ型骨折一般在X射线片上较难发现,CT可见一两个扫描层面的骨折。出现的原因:合页保留偏少、截骨过深或撑开角度较大时亦可出现,见图4。"
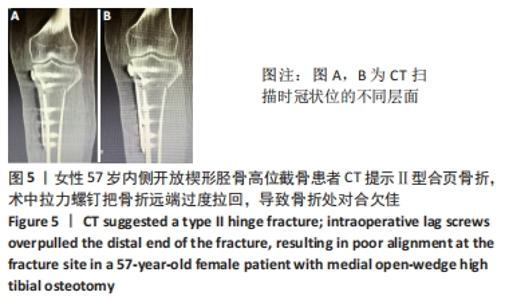
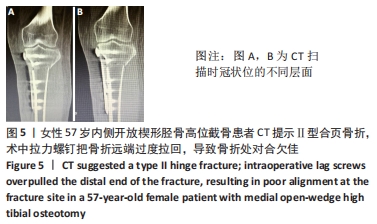
2.4.2 Ⅱ型合页骨折 女性患者,57岁。Ⅱ型骨折一般较易在术中或术后复查X射线片时发现,出现的原因:截骨线选低了,向下骨折。Ⅱ型合页骨折见图5。"
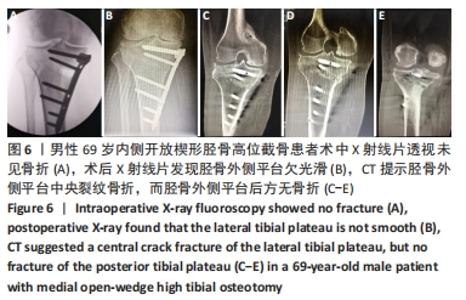
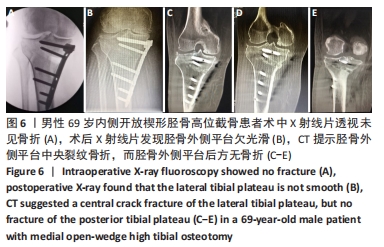
2.4.3 Ⅲ型合页骨折 男性患者,69岁。Ⅲ型骨折一般在术中即可发现,出现的原因:截骨深度不够,预留合页较多,撑开时易导致骨折。而Ⅲ型合页部分骨折在临床中较少见,也较难发现,出现的原因与Ⅲ型合页骨折一样。通常术中X射线片透视未见骨折,术后X射线片发现胫骨外侧平台欠光滑,CT提示胫骨外侧平台中央裂纹骨折,而胫骨外侧平台后方无骨折,见图6。"
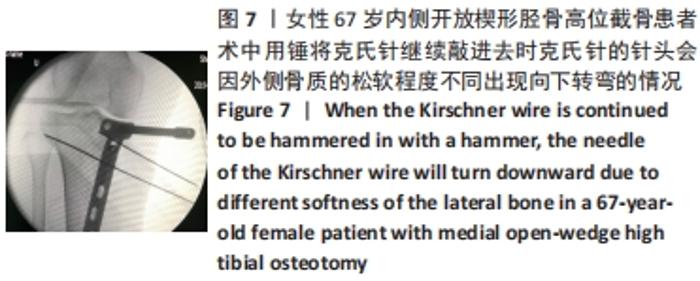
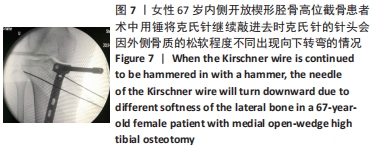
外侧合页的骨折,是内侧开放楔形胫骨高位截骨手术一种常见的并发症,文献报道的发生率为5.6%-25%[7-11]。其中外侧合页的骨折被分为3型,Ⅰ型骨折多是由于过深的截骨,截骨线向外侧延长导致外侧皮质的断裂;Ⅱ型骨折多是由于截骨线过低或截骨的方向有误造成合页在胫腓关节下方处断裂;Ⅲ型骨折则多是由于截骨深度不够,造成撑开时截骨线向距离更近的上方关节面劈裂、或由于截骨的方向过度偏向外上方造成合页位置过于靠近关节面或直接截入至关节面[12]。Ⅰ型骨折一般在X射线片上比较难发现,一旦患者出现术后下肢的肿胀,即需考虑是否存在合页骨折;Ⅰ型骨折一般需要CT的确认,但Ⅰ型骨折比较稳定,通常不需要额外的处理。Ⅱ、Ⅲ型骨折在术后的X射线片上较易发现,但这2种类型的骨折不稳定,增加了内固定的负荷,会出现应力遮挡效应[13],需额外的辅助固定,不宜早期下地负重,可在4周后部分负重,6周后视骨痂愈合情况决定是否完全负重,同时这两种类型的骨折也增加了术后延迟愈合和不愈合的风险,因此选择合适的截骨位置以及保留合适大小的合页对于预防合页处的骨折非常重要。另外有研究发现在合页区骨质内留置保护性的螺钉或克氏针,或在截骨顶点合页处进行矢状面预钻孔,都可以降低合页骨折发生的概率[14-17]。除此之外,作者在临床中还发现,Ⅲ型骨折存在部分骨折的可能,即在术中X射线片未见骨折,术后X射线片发现胫骨外侧平台欠光滑,通过CT检查提示胫骨外侧平台中央裂纹骨折,而胫骨外侧平台后方无骨折。对于这一类骨折患者容易在临床引起忽视,应该引起重视。 2.5 截骨线定位与实际截骨出现偏差 女性患者67岁。原因: (1)克氏针定位偏差,会导致截骨线出现误差:最初使用克氏针钻入胫骨进行定位时方向尚可,之后用锤将克氏针继续敲进去时,克氏针的针头会因外侧骨质松软程度的不同出现往下转弯的情况,见图7,而实际截骨的时候电锯只能沿着初始克氏针的方向进入胫骨骨质。而另外一种情况是相同的原因出现了向上转弯,也会造成实际截骨线的偏差。 "
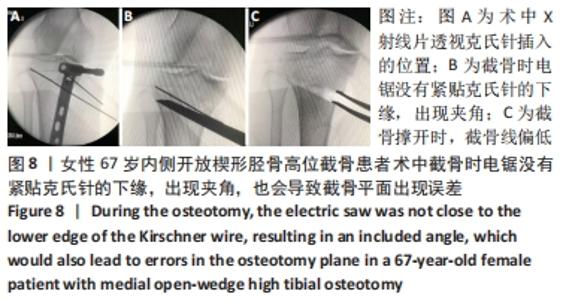
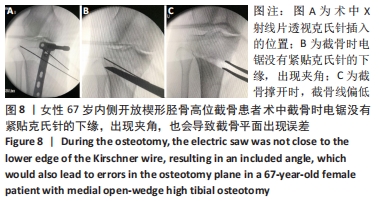
(2)调整克氏针方向以后,确保克氏针方向正确,但是截骨时电锯没有紧贴克氏针的下缘,出现了夹角,也会导致截骨平面出现误差,最终导致截骨线偏低,见图8。 "
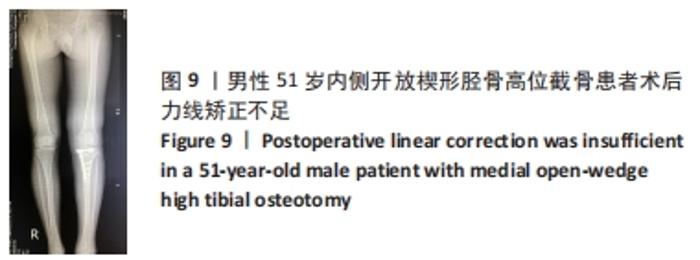
截骨的准确性对于预防合页处骨折和术后骨的延迟愈合起到了非常重要的作用,但在实际截骨过程中,因外侧骨质的松软程度不同,当用锤将克氏针继续敲进去时,针头会出现向上或向下转弯的情况。而实际截骨的时候电锯只能沿着初始克氏针的方向进行截骨,导致实际截骨线出现差异。因此在进入克氏针时,建议全程使用电钻,避免使用锤将克氏针敲入。另外一种情况是克氏针方向正确,但是截骨时电锯没有紧贴克氏针的下缘,出现夹角,也会导致截骨平面出现误差。而术中的透视就显得非常重要,能够降低误差发生的风险。 2.6 力线矫正不足 男性患者,51岁,影像学图片见图9。 "
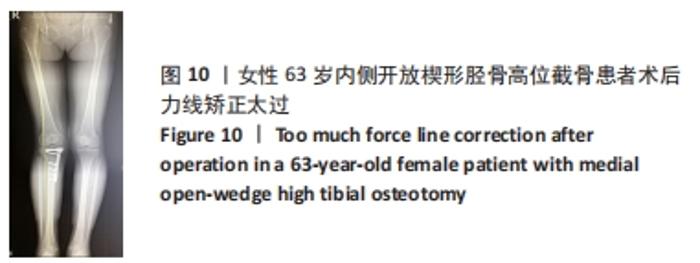
2.7 力线矫正太过 女性患者,63岁,影像学图片见图10。"
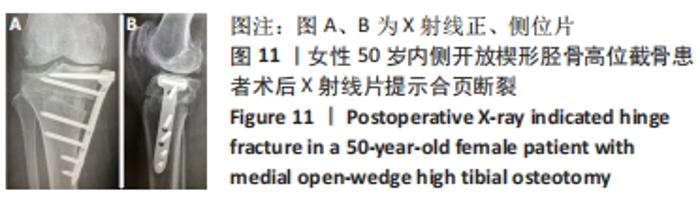
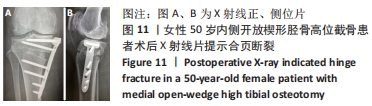
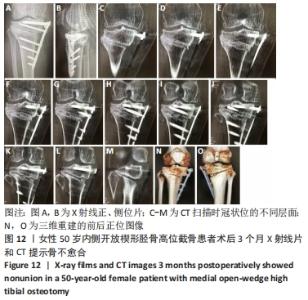
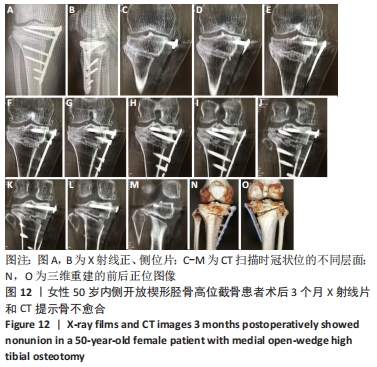
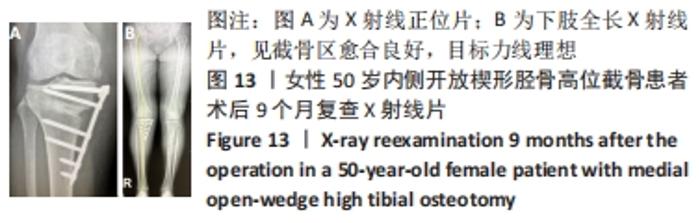
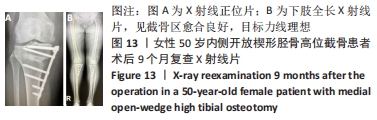
调整力线是内侧开放楔形胫骨高位截骨手术治疗膝骨关节炎的核心,但是尽管数字化技术已经被应用于临床,力线调整不良的问题却仍然存在。传统的力线认为应通过Fujisawa点,而目前更强调个体化差异。力线矫正太过可能与膝关节周围软组织松弛有关[18-19],会加速外侧间室的退变。力线矫正不足,除人为可能导致的原因外,还可能与体位差异(站立位-平卧位)和胫骨内翻畸形角度过大有关[20-22],会使得内侧间室负荷减轻不足,出现术后持续疼痛和软骨磨损,最终导致翻修。因此有学者建议应在持续外翻应力的情况下撑开截骨间隙,以减少体位差异和软组织松弛的影响[23]。此外,在临床观察中发现,术前下肢全长片拍摄位置欠标准,也会对术前规划和术中力线的调整产生影响,如术前下肢全长片存在内旋,会导致测量角度的偏小;存在外旋,会导致测量角度的偏大,而术中又未进行透视确认力线,因而导致力线矫正不足或太过。因此,术中需要反复确认力线调整的位置是否准确,或借助3D打印个体化截骨导板提高手术的精准性。 2.8 骨不愈合 女性患者,50岁,内侧开放楔形胫骨高位截骨术后患肢即刻负重行走,康复计划过度激进,3个月后右膝负重痛,复查X射线片发现骨不愈合,见图11,12。予截骨区注射富血小板血浆(瑞士瑞珍科技有限公司),患肢不负重半年,半年后复查X射线片提示截骨区愈合良好,患者恢复完全负重行走,膝关节功能良好,见图13。 "
"
"
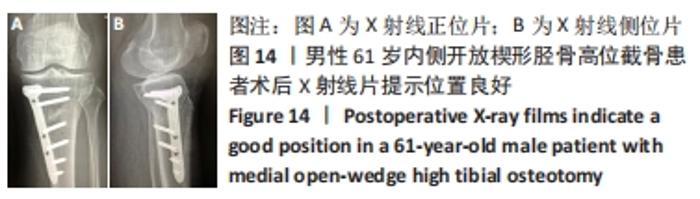
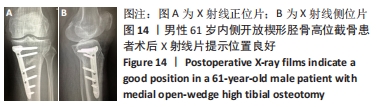
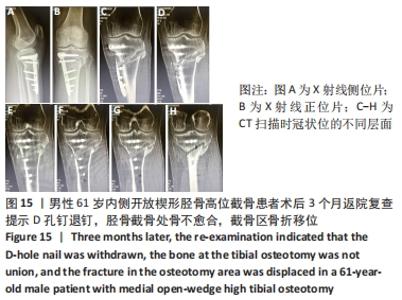
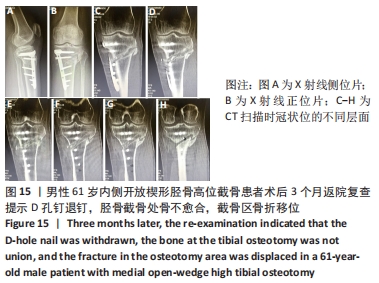
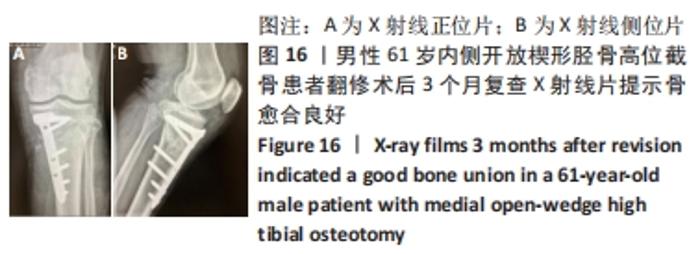
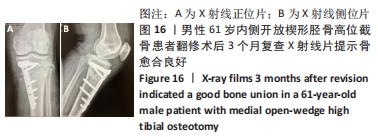
截骨处的骨不愈合也是内侧开放楔形胫骨高位截骨手术的一种并发症,目前文献报道的截骨不愈合率为0.5%-4.3%[24-27]。导致截骨间隙不愈合的主要危险因素有截骨间隙过大、长期吸烟和内固定的不稳定[28-29]。还有一些研究发现撑开角度大于13 mm、Ⅱ型或Ⅲ型合页骨折、截骨线在安全区域以下可引起术后骨愈合的延迟[30],而骨愈合的延迟很可能导致骨不愈合的发生,为了更好地明确和解决这一问题,很多学者对截骨区的植骨问题进行了研究,但仍未获得统一的结论。外国的研究者发现使用骨填充物会增加手术部位的并发症发生率,当截骨撑开距离大于15 mm时才建议使用,除此范围内不使用骨填充物不会增加不愈合的风险[31],其他学者也得出了相似的结论[32-33]。还有一些研究发现,尽管在截骨区不进行骨移植可以获得满意的效果,但撑开间隙大小与愈合时间有明显的相关性[34]。截骨间隙越大意味着填充骨小梁的面积越大,这很可能是引起截骨处延迟愈合或不愈合的重要原因。作者认为植骨在总体上可以加快患者术后的康复时间,所带来的并发症发生率较低,可以合理使用。同时因为富血小板血浆含有多种生长因子,且安全性较高,使用富血小板血浆在一定程度上有利于加快截骨区的愈合,但是由于其价格较高,需视情况使用。 2.9 骨折移位、骨不愈合、退钉 男性患者,61岁,内侧开放楔形胫骨高位截骨术后患肢即刻负重行走,康复计划过度激进,患者因路途较远随访较难。术后3个月左膝负重疼痛,返院复查提示D孔钉退钉、胫骨截骨处骨不愈合、截骨区骨折移位。予刮除坏死区死骨+自体髂骨取骨植骨+调整D孔钉的方向,翻修术后3个月复查X射线片提示骨愈合良好,见图14-16。 "
"
"
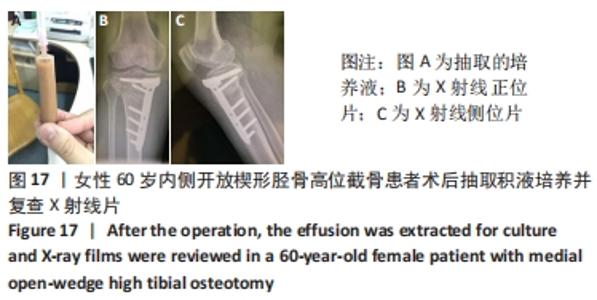
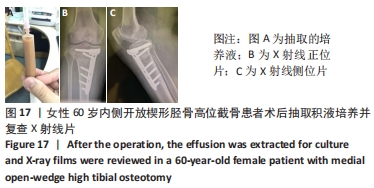
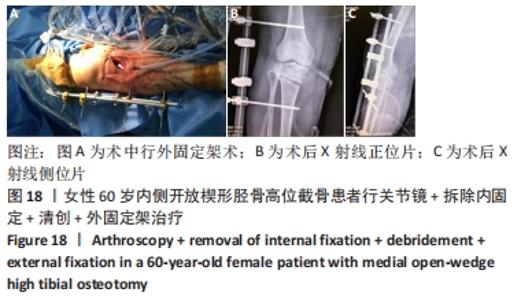
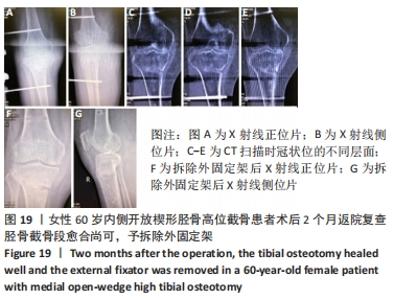
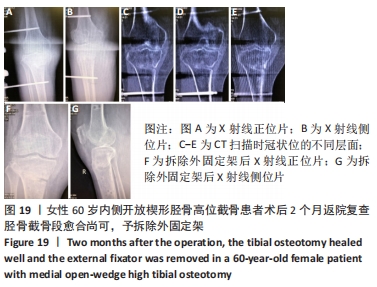
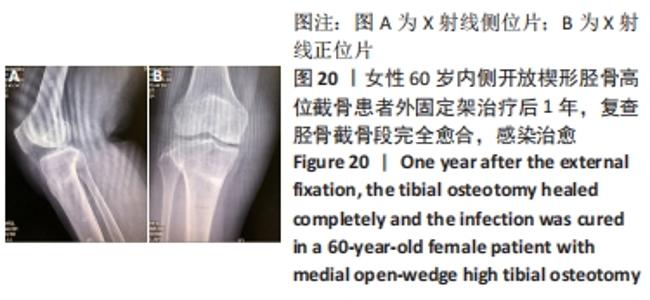
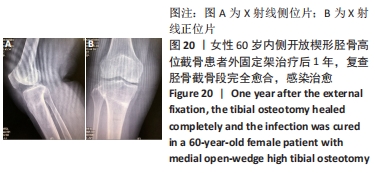
2.10 术后感染 女性患者,60岁,右膝术后2个月,右膝突然红肿热痛,胫骨处伤口局部有波动感,关节腔抽液培养发现金黄色葡萄球菌。之后行右膝关节镜+拆除内固定+清创+外固定架治疗,术中膝关节腔抽液再次培养发现金黄色葡萄球菌。予膝关节腔内留置进出水管并用生理盐水持续冲洗,术中在胫骨截骨面放入万古霉素[VIANEX S.A.(PLANT C)]4 g+利福平(广东华南药业集团有限公司)10粒。术后口服利福平 0.45 g,1次/d;静滴盐酸克林霉素 0.45 g(广州白云山天心制药股份有限公司,8 h 1次),+左氧氟沙星氯化钠注射液0.5 g(第一三共制药(北京)有限公司,1次/d)。右膝关节腔冲洗1周后取引流液送检未见细菌,术后C-反应蛋白和血沉水平逐渐降低,拔除冲洗管。术后2周术口愈合良好后出院,带药盐酸克林霉素棕榈酸酯分散片(广州一品红制药有限公司)0.4 g口服3次/d,乳酸左氧氟沙星分散片 (海南全星制药有限公司)0.4 g 口服 1次/d,共2个月。口服药物抗感染治疗2个月后,患者右膝轻度肿胀疼痛,右膝和小腿术口肤温偏高,肤色偏红,复查白细胞计数10.45×109 L-1,中性粒细胞63.1%,血沉42 mm/h、C-反应蛋白0.61 mg/L,拆除外固定架,见图17-20。"
"

"
"
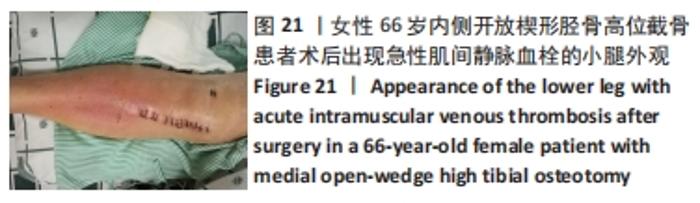
内侧开放楔形胫骨高位截骨术后的感染是一种较难处理的并发症,文献报道浅表感染的发生率为1%-9%,深部感染的发生率为0.5%-4.7%[35-38],其中吸烟、糖尿病、老年患者、人工植骨替代物的使用、男性和长时间麻醉持续时间(≥210 min)是导致术后手术部位感染的危险因素[38-39]。对于确定出现感染的患者,首要的治疗是彻底清创和静脉或口服应用抗生素,早期移除内固定也有益于控制感染,同时予外固定架以固定,防止矫形的丢失。此次研究中的1例深部感染患者采用关节镜+拆除内固定+清创+外固定架术治疗,术后患者感染控制良好。 2.11 术后急性肌间静脉血栓形成 女性患者,66岁,右膝术后3 d出现小腿下方的肿胀,见图21,完善彩超提示右小腿肌间静脉曲张并急性完全性血栓形成声像,予口服利伐沙班抗凝治疗。 "
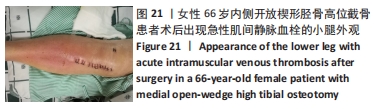
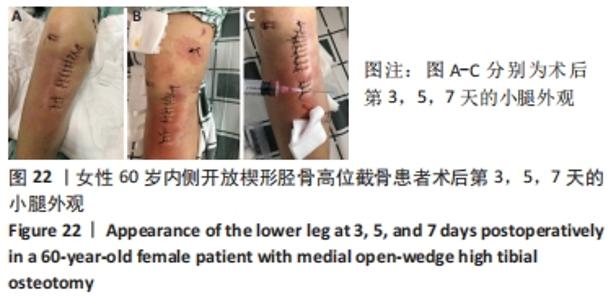
术后急性静脉血栓形成是膝关节周围手术后一种比较危险的并发症,其导致的肺栓塞可致命,目前文献报道胫骨高位截骨术后静脉血栓的发生风险为2.4%-41.0%[40-42]。ONISHI等[43]做了更进一步的研究,他们发现相比于内侧开放楔形胫骨高位截骨手术,仅外侧闭合楔形胫骨截骨手术被认为与术后急性静脉血栓的形成密切相关。KIM等[44]发现亚洲患者内侧开放楔形胫骨高位截骨术后静脉血栓栓塞的总发生率很低,但是体质量指数> 30 kg/m2被认为是静脉血栓栓塞发生的易感因素,因此这类患者应该考虑选择性的提前预防。尽管目前发现内侧开放楔形胫骨高位截骨术后发生静脉血栓的风险不高,但是仍然需要提前做好干预和预防。抗凝药的使用被认为是内侧开放楔形胫骨高位截骨术后的常规治疗方案[43],但是对于该类药物的使用应综合评估、个性化使用,当出血风险明显增加时应及时停用。同时,还可以根据Autar量表和Caprini量表对血栓形成风险的等级进行评估[45-46],针对不同的风险等级,个体化采取主被动锻炼、抗凝药物和(或)间歇性充气加压装置联合预防和治疗,减少术后下肢静脉血栓的形成。 2.12 术后伤口肿痛 女性患者,60岁,无基础疾病,未服用抗凝抗聚药物,凝血功能正常,术后第1天复查X射线片提示外侧合页完好,术后第3天开始出现右小腿术口周围的轻度肿胀和瘀斑,术后第5天小腿术口周围中度肿胀,术后第7天小腿术口周围重度肿胀,见图22。完善下肢静脉彩超未发现血栓形成,患者小腿肿痛感明显,在术口下方用注射器可抽出少量血性液体,每天用针头对周围皮肤进行散在穿刺和减压,方便血性液体的渗出(1次/d,一般3-5 d可缓解),穿刺后用无菌纱块挤压促进积血的排出。抗生素确保长时间覆盖预防感染,小腿术区冰敷每天两三次,加强踝泵锻炼,口服消炎止痛药物和迈之灵(德国礼达大药厂)消肿,一般对症治疗3-5 d后肿胀可消退。治疗期间可在小腿后侧或踝关节上方外敷清热解毒、活性化瘀的中药膏或吲哚美辛巴布膏(尼普洛外用药品株式会社)等促进消除肿痛的药物,但需注意避免皮肤过敏。术后半年随访时复查X射线片,发现外侧合页断裂,见图23,但患者术后膝关节功能恢复良好。 "


"


术后肿痛也是内侧开放楔形胫骨高位截骨术后的一种并发症,但导致术后肿痛的原因比较多,作者前期做了一部分回顾性调查,发现隐性出血量≥150 mL、外侧合页断裂、吸烟史、下肢静脉血栓的形成和撑开角度≥12°可能是导致内侧开放楔形胫骨高位截骨术后发生下肢肿痛的危险因素。此例患者术后即出现肿痛,早期X射线片未能发现外侧合页断裂,术后半年复查发现是由于外侧合页断裂引起的。作者认为术中的精细操作非常重要,在截骨过程中要做到轻柔缓慢,注意软组织的保护,并且手术全程应尽可能减少止血带的使用,降低术后的隐性出血量。合页断裂与否也是决定术后发生肿痛非常重要的因素之一,一旦患者出现术后肿痛,建议要完善CT检查明确合页是否断裂以及完善彩超明确血栓是否存在,方便指导下一步治疗和康复方案的调整。此外,患者如果服用了抗凝或抗聚药物,也会引发术后的下肢肿胀。术前应注意这些影响因素,做好术后应对的准备。同时,术后需进行加压包扎,并放置引流管,术后第2天或第3天予拔除引流,尽可能减少术后肿痛的发生。如果患者没有出现明显的皮下波动感和深部感染,可采取保守治疗,绝大部分肿胀可自行吸收;如果出现术后感染,则应及时使用或升级抗生素进一步处理。 "

| [1] GLYN-JONES S, PALMER AJ, AGRICOLA R, et al. Osteoarthritis. Lancet. 2015;386(9991):376-387. [2] COVENTRY MB. Osteotomy of the upper portion of the tibia for degenerative arthritis of the knee. A preliminary report. 1965. Clin Orthop Relat Res. 1989;(248):4-8. [3] HERNIGOU P, MEDEVIELLE D, DEBEYRE J, et al. Proximal tibial osteotomy for osteoarthritis with varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg Am. 1987;69(3):332-354. [4] COVENTRY MB. Osteotomy about the knee for degenerative and rheumatoid arthritis. J Bone Joint Surg Am. 1973;55(1):23-48. [5] SONG EK, SEON JK, PARK SJ, et al. The complications of high tibial osteotomy: closing- versus opening-wedge methods. J Bone Joint Surg Br. 2010;92(9):1245-1252. [6] HAN SB, IN Y, OH KJ, et al. Complications Associated With Medial Opening-Wedge High Tibial Osteotomy Using a Locking Plate: A Multicenter Study. J Arthroplasty. 2019;34(3):439-445. [7] DAY M, WOLF BR. Medial Opening-Wedge High Tibial Osteotomy for Medial Compartment Arthrosis/Overload. Clin Sports Med. 2019;38(3): 331-349. [8] SEO SS, KIM OG, SEO JH, et al. Complications and Short-Term Outcomes of Medial Opening Wedge High Tibial Osteotomy Using a Locking Plate for Medial Osteoarthritis of the Knee. Knee Surg Relat Res. 2016; 28(4):289-296. [9] OGAWA H, MATSUMOTO K, AKIYAMA H. The prevention of a lateral hinge fracture as a complication of a medial opening wedge high tibial osteotomy: a case control study. Bone Joint J. 2017;99-B(7):887-893. [10] NAKAMURA R, KOMATSU N, MURAO T, et al. The validity of the classification for lateral hinge fractures in open wedge high tibial osteotomy. Bone Joint J. 2015;97-B(9):1226-1231. [11] HAN SB, CHOI JH, MAHAJAN A, et al. Incidence and Predictors of Lateral Hinge Fractures Following Medial Opening-Wedge High Tibial Osteotomy Using Locking Plate System: Better Performance of Computed Tomography Scans. J Arthroplasty. 2019;34(5):846-851. [12] 林炯同,杨伟毅,潘建科,等.内侧开放楔形高位胫骨截骨术外侧合页骨折的处理[J]. 中国矫形外科杂志,2019,27(10):907-911. [13] KANG KT, KOH YG, LEE JA, et al. Biomechanical effect of a lateral hinge fracture for a medial opening wedge high tibial osteotomy: finite element study. J Orthop Surg Res. 2020;15(1):63. [14] DIFFO KA, MAAS S, HOFFMANN A, et al. Mechanical strength assessment of a drilled hole in the contralateral cortex at the end of the open wedge for high tibial osteotomy. J Exp Orthop. 2017;4(1):23. [15] BOSTROM A, AMIN AK, MACPHERSON GJ, et al. Hinge location and apical drill holes in opening wedge high tibial osteotomy: A finite element analysis. J Orthop Res. 2021;39(3):628-636. [16] GULAGACI F, JACQUET C, EHLINGER M, et al. A protective hinge wire, intersecting the osteotomy plane, can reduce the occurrence of perioperative hinge fractures in medial opening wedge osteotomy. Knee Surg Sports Traumatol Arthrosc. 2020;28(10):3173-3182. [17] JACQUET C, MARRET A, MYON R, et al. Adding a protective screw improves hinge’s axial and torsional stability in High Tibial Osteotomy. Clin Biomech (Bristol, Avon). 2020;74:96-102. [18] PARK JG, KIM JM, LEE BS, et al. Increased preoperative medial and lateral laxity is a predictor of overcorrection in open wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2020;28(10):3164-3172. [19] KIM YT, CHOI JY, LEE JK, et al. Coronal tibiofemoral subluxation is a risk factor for postoperative overcorrection in high tibial osteotomy. Knee. 2019;26(4):832-837. [20] JIN C, SONG EK, SANTOSO A, et al. Survival and Risk Factor Analysis of Medial Open Wedge High Tibial Osteotomy for Unicompartment Knee Osteoarthritis. Arthroscopy. 2020;36(2):535-543. [21] KAMADA S, SHIOTA E, SAEKI K, et al. Severe varus knees result in a high rate of undercorrection of lower limb alignment after opening wedge high tibial osteotomy. J Orthop Surg (Hong Kong). 2019;27(2): 615506948. [22] LEE OS, LEE ES, LEE YS. Disparity between Preoperative Target Correction Amount and Postoperative Correction Amount in Open Wedge High Tibial Osteotomy. Knee Surg Relat Res. 2019;31(2):126-131. [23] KIM MS, SON JM, KOH IJ, et al. Intraoperative adjustment of alignment under valgus stress reduces outliers in patients undergoing medial opening-wedge high tibial osteotomy. Arch Orthop Trauma Surg. 2017; 137(8):1035-1045. [24] FLOERKEMEIER S, STAUBLI AE, SCHROETER S, et al. Outcome after high tibial open-wedge osteotomy: a retrospective evaluation of 533 patients. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):170-180. [25] WOODACRE T, RICKETTS M, EVANS JT, et al. Complications associated with opening wedge high tibial osteotomy--A review of the literature and of 15 years of experience. Knee. 2016;23(2):276-282. [26] HAN SB, IN Y, OH KJ, et al. Complications Associated With Medial Opening-Wedge High Tibial Osteotomy Using a Locking Plate: A Multicenter Study. J Arthroplasty. 2019;34(3):439-445. [27] SEO SS, KIM OG, SEO JH, et al. Complications and Short-Term Outcomes of Medial Opening Wedge High Tibial Osteotomy Using a Locking Plate for Medial Osteoarthritis of the Knee. Knee Surg Relat Res. 2016; 28(4):289-296. [28] DAY M, WOLF BR. Medial Opening-Wedge High Tibial Osteotomy for Medial Compartment Arthrosis/Overload. Clin Sports Med. 2019;38(3): 331-349. [29] HOOPER NM, SCHOUTEN R, HOOPER GJ. The outcome of bone substitute wedges in medial opening high tibial osteotomy. Open Orthop J. 2013;7:373-377. [30] GOSHIMA K, SAWAGUCHI T, SHIGEMOTO K, et al. Large opening gaps, unstable hinge fractures, and osteotomy line below the safe zone cause delayed bone healing after open-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2019;27(4):1291-1298. [31] KFURI M, LOBENHOFFER P. High Tibial Osteotomy for the Correction of Varus Knee Deformity. J Knee Surg. 2017;30(5):409-420. [32] JUNG WH, TAKEUCHI R, KIM DH, et al. Faster union rate and better clinical outcomes using autologous bone graft after medial opening wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2020;28(5):1380-1387. [33] SLEVIN O, AYENI OR, HINTERWIMMER S, et al. The role of bone void fillers in medial opening wedge high tibial osteotomy: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2016;24(11):3584-3598. [34] EL-ASSAL MA, KHALIFA YE, ABDEL-HAMID MM, et al. Opening-wedge high tibial osteotomy without bone graft. Knee Surg Sports Traumatol Arthrosc. 2010;18(7):961-966. [35] ANAGNOSTAKOS K, MOSSER P, KOHN D. Infections after high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):161-169. [36] HAN SB, IN Y, OH KJ, et al. Complications Associated With Medial Opening-Wedge High Tibial Osteotomy Using a Locking Plate: A Multicenter Study. J Arthroplasty. 2019;34(3):439-445. [37] SCHENKE M, DICKSCHAS J, SIMON M, et al. Corrective osteotomies of the lower limb show a low intra- and perioperative complication rate-an analysis of 1003 patients. Knee Surg Sports Traumatol Arthrosc. 2018;26(6):1867-1872. [38] KAWATA M, JO T, TAKETOMI S, et al. Type of bone graft and primary diagnosis were associated with nosocomial surgical site infection after high tibial osteotomy: analysis of a national database. Knee Surg Sports Traumatol Arthrosc. 2021;29(2):429-436. [39] LIU TW, CHIU CH, CHEN AC, et al. Risk Factor Analysis for Infection after Medial Open Wedge High Tibial Osteotomy. J Clin Med. 2021;10(8): 1727. [40] MARTIN R, BIRMINGHAM TB, WILLITS K, et al. Adverse event rates and classifications in medial opening wedge high tibial osteotomy. Am J Sports Med. 2014;42(5):1118-1126. [41] MILLER BS, DOWNIE B, MCDONOUGH EB, et al. Complications after medial opening wedge high tibial osteotomy. Arthroscopy. 2009;25(6): 639-646. [42] KUBOTA M, KIM Y, INUI T, et al. Risk factor for venous thromboembolism after high tibial osteotomy -analysis of patient demographics, medical comorbidities, operative valuables, and clinical results. J Orthop. 2021; 25:124-128. [43] ONISHI S, ISEKI T, KANTO R, et al. Incidence of and risk factors for deep vein thrombosis in patients undergoing osteotomies around the knee: comparative analysis of different osteotomy types. Knee Surg Sports Traumatol Arthrosc. 2021;29(10):3488-3494. [44] KIM KI, KIM GB, LEE MG, et al. Do We Need Chemoprophylaxis to Prevent Venous Thromboembolism following Medial Open-Wedge High Tibial Osteotomy? J Knee Surg. 2021;34(9):1007-1013. [45] AUTAR R. Nursing assessment of clients at risk of deep vein thrombosis (DVT): the Autar DVT scale. J Adv Nurs. 1996;23(4):763-770. [46] CASSIDY MR, ROSENKRANZ P, MCANENY D. Reducing postoperative venous thromboembolism complications: in reply to Lau and colleagues. J Am Coll Surg. 2014;219(5):1103-1104. [47] MAO Y, XIONG Y, LI Q, et al. 3D-Printed Patient-Specific Instrumentation Technique Vs. Conventional Technique in Medial Open Wedge High Tibial Osteotomy: A Prospective Comparative Study. Biomed Res Int. 2020;2020:1923172. [48] AKAMATSU Y, KOBAYASHI H, KUSAYAMA Y, et al. Comparative Study of Opening-Wedge High Tibial Osteotomy With and Without a Combined Computed Tomography-Based and Image-Free Navigation System. Arthroscopy. 2016;32(10):2072-2081. |
| [1] | Zhai Hongjie, Han Guanda, Li Lei, Dong Xiaohui, Jiang Zhiquan, Lou Feiyun. 3D printed polyetheretherketone material for skull defect repair [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(3): 380-384. |
| [2] | Yao Xiaoling, Peng Jiancheng, Xu Yuerong, Yang Zhidong, Zhang Shuncong. Variable-angle zero-notch anterior interbody fusion system in the treatment of cervical spondylotic myelopathy: 30-month follow-up [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1377-1382. |
| [3] | He Junjun, Huang Zeling, Hong Zhenqiang. Interventional effect of Yanghe Decoction on synovial inflammation in a rabbit model of early knee osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(5): 694-699. |
| [4] | Lin Xuchen, Zhu Hainian, Wang Zengshun, Qi Tengmin, Liu Limin, Suonan Angxiu. Effect of xanthohumol on inflammatory factors and articular cartilage in a mouse mode of osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(5): 676-681. |
| [5] | Jiang Xu, Cao Fuyang, Xiong Ao, Yang Meng, Tan Jun, Yu Yang, Zhang Shaokun, Xu Jianzhong. Distribution, drug resistance, and clinical characteristics of pathogenic bacteria in 102 cases of periprosthetic joint infection [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(36): 5837-5843. |
| [6] | Sun Yiyuan, Li Qi, Xiong Yan, Li Jian. Different doses of tranexamic acid affect blood loss after high tibial osteotomy [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(36): 5857-5861. |
| [7] | Lin Zhiyu, Han Jie, Ren Guowu, Chai Yuan, Wen Shuaibo, Wu Yukun, Xie Xiaozhong, Jin Wanqing. Active components of flemingia in regulating the signaling pathways related to knee osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(36): 5889-5896. |
| [8] | Wu Yongli, Liu Di, Wang Duo, Liu Junwei, Ma Yuyuan. Effect of warm acupuncture on PI3K/Akt signaling pathway in articular cartilage of a rabbit knee osteoarthritis model [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(35): 5596-5601. |
| [9] | Cao Fei, Hui Min, Dong Xiling, Wang Le, Wang Zuxu, Zhang Min, Zhang Xiaoming, Liu Tongbin. Preparation of silver-loaded nanohydroxyapatite/polycaprolactone composite nanofiber scaffold and its osteogenic and antibacterial properties [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(34): 5461-5467. |
| [10] | Wang Yiming, Yang Fengdong, Mao Wenbin, Jia Xin, Wei Shuxin, Wei Xinting. Comparison of clinical application of skull repair materials of three-dimensional digital shaping polyether ether ketone and titanium mesh [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(34): 5492-5497. |
| [11] | Song Wei, Zhang Yaxin, Jia Dazhou, Sun Yu. Adjective application of dexamethasone combined with furosemide for early pain and swelling after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(33): 5317-5322. |
| [12] | Lu Qigui, Xie Pingjin, Luo Zhen, Li Feilong, Chen Qunqun, Chai Shengting. MicroRNA-20b-5p effects on cartilage and subchondral bone angiogenesis in early-stage osteoarthritis rats [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(29): 4658-4665. |
| [13] | Ci Wentao, Zhang Xinlong, Yan Shi, Wang Zhao. Reducing the recurrence of infection after the application of Masquelet technique for osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(28): 4546-4552. |
| [14] | Wang Wenli, Zhang Zihan, Li Yourui. Application of the socket-shield technique in the implant restoration [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(27): 4406-4410. |
| [15] | Xu Ran, Chen Xingyu, Li Zhiqiang. Antibacterial agents loaded on hydroxyapatite scaffolds: action mechanism between the drug and the scaffold [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(27): 4411-4416. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||