Chinese Journal of Tissue Engineering Research ›› 2022, Vol. 26 ›› Issue (15): 2323-2329.doi: 10.12307/2022.584
Previous Articles Next Articles
Effect of knee ligamentous laxity on patient satisfaction after total knee arthroplasty: a medium to long-term follow-up
Xia Peige, Yin Li, Wang Haitao, Zhang Yi, Qiao Renqiu, Kong Zhiheng, Zhao Hongbo, Shi Xiangyu
- Department of Orthopedics, the First Affiliated Hospital of Zhengzhou University, Zhengzhou 450000, Henan Province, China
-
Received:2021-08-02Revised:2021-08-04Accepted:2021-09-01Online:2022-05-28Published:2022-01-05 -
Contact:Yin Li, MD, Chief physician, Master’s supervisor, Department of Orthopedics, the First Affiliated Hospital of Zhengzhou University, Zhengzhou 450000, Henan Province, China -
About author:Xia Peige, Master candidate, Department of Orthopedics, the First Affiliated Hospital of Zhengzhou University, Zhengzhou 450000, Henan Province, China -
Supported by:Key Scientific Research Project of Colleges in Henan Province, No. 20A310022 (to YL)
CLC Number:
Cite this article
Xia Peige, Yin Li, Wang Haitao, Zhang Yi, Qiao Renqiu, Kong Zhiheng, Zhao Hongbo, Shi Xiangyu. Effect of knee ligamentous laxity on patient satisfaction after total knee arthroplasty: a medium to long-term follow-up[J]. Chinese Journal of Tissue Engineering Research, 2022, 26(15): 2323-2329.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
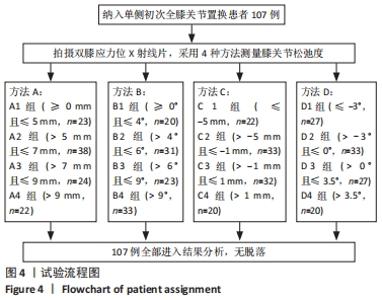
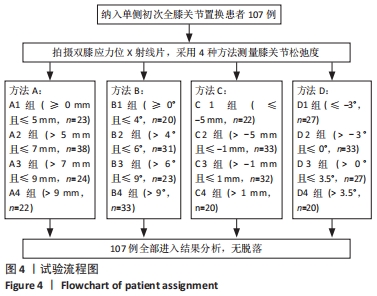
2.1 参与者数量分析 107例患者均进入结果分析。 2.2 试验分组流程 见图4。"
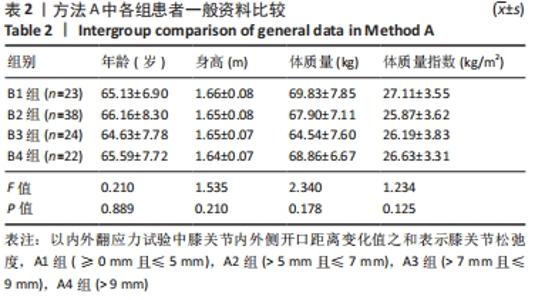
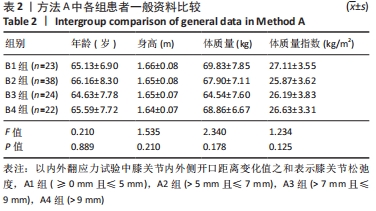
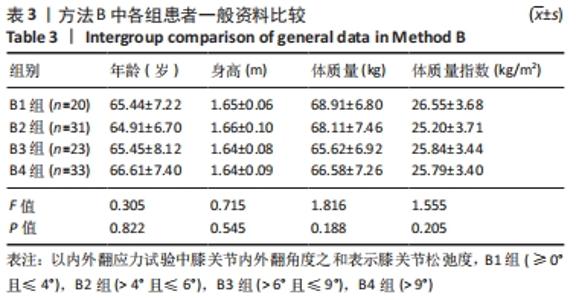
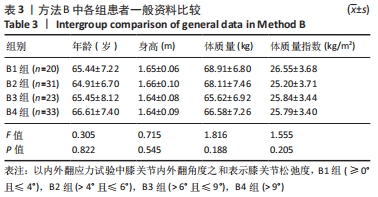
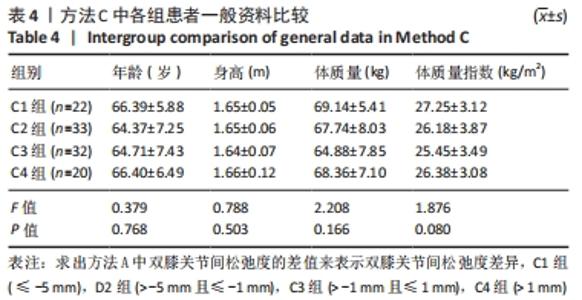
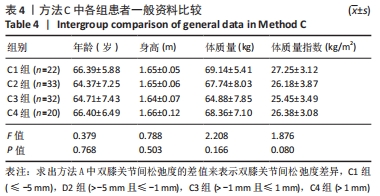
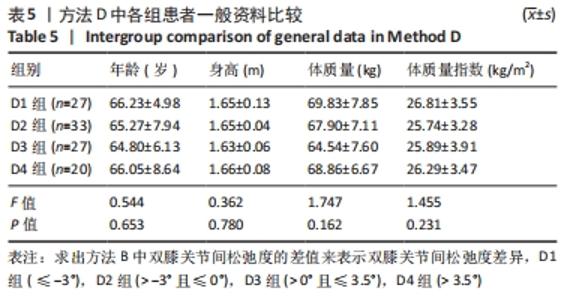
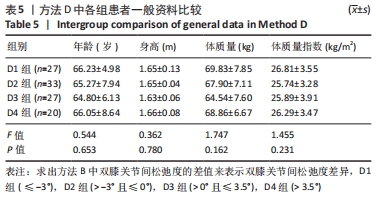
2.3 各组基线资料比较 4测量方法中,各组患者年龄、身高、体质量指数等一般资料比较差异均无显著性意义(P > 0.05),见表2-5。"
"
"
"

2.4 各组OKS与改良Lysholm评分评估结果 见图5,6。"


"


2.4.1 OKS评估结果 见表6。"
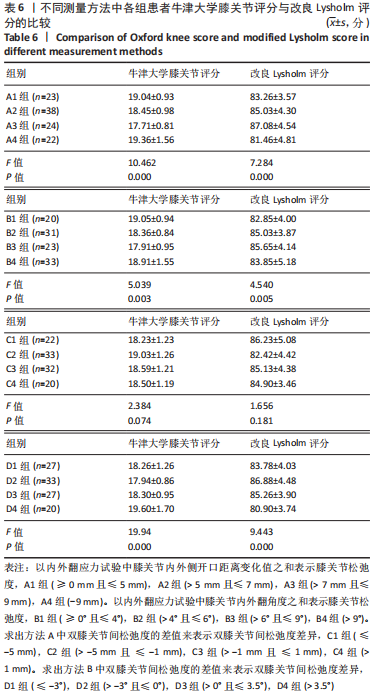

单因素方差分析显示,方法A中4组患者OKS评估结果比较差异有显著性意义(F=10.462,P=0.000);组间两两比较LSD检验显示,除A1、A4组OKS比较差异无显著性意义(P > 0.05)外,其余组间两两比较差异均有显著性意义(P < 0.05或P < 0.01)。单因素方差分析显示,方法B中4组患者OKS评估结果比较差异有显著性意义(F=5.039,P=0.003);组间两两比较LSD检验显示,B1组与B4组患者OKS评估结果比较差异无显著性意义(P=0.664),B2与B3组、B2组与B4组患者OKS评估结果比较差异无显著性意义(P > 0.05),其余组间两两比较差异均有显著性意义(P < 0.05或P < 0.01)。单因素方差分析显示,方法C中4组患者OKS评估结果比较差异无显著性意义(F=2.384,P=0.074);组间两两比较LSD检验显示,C1组与C3组、C3组与C4组患者OKS评估结果比较差异有显著性意义(P < 0.05),其余组间两两比较差异无显著性意义(P > 0.05)。单因素方差分析显示,方法D中4组患者OKS评估结果比较差异有显著性意义(F=19.94,P=0.000);组间两两比较LSD检验显示,D1组与D3组、D2组与D3组患者OKS评估结果比较差异无显著性意义 (P > 0.05),其余组间两两比较差异均有显著性意义(P < 0.01)。 2.4.2 各组改良Lysholm评分 见表6。 单因素方差分析显示,方法A中4组患者改良Lysholm评分比较差异有显著性意义(F=7.284,P=0.000);组间两两比较LSD检验显示,A1组与A2组、A1组与A4组、A2组与A3组患者改良Lysholm评分比较差异无显著性意义(P > 0.05),其余组间两两比较差异有显著性意义(P < 0.01)。单因素方差分析显示,方法B中4组患者改良Lysholm评分比较差异有显著性意义(F=4.540,P=0.005);组间两两比较LSD检验显示,B1组与B2组、B1组与B3组、B3组与B4组患者改良Lysholm评分比较差异有显著性意义(P < 0.05或P < 0.01),其余组间两两比较差异无显著性意义(P > 0.05)。单因素方差分析显示,方法C中4组患者改良Lysholm评分比较差异无显著性意义(F=1.656,P=0.181);组间两两比较LSD检验显示,C1组与C3组患者改良Lysholm评分比较差异有显著性意义(P < 0.05),其余组间两两比较差异无显著性意义(P > 0.05)。单因素方差分析显示,方法D中4组患者改良Lysholm评分比较差异有显著性意义(F=9.443,P=0.000);组间两两比较LSD检验显示,D1组与D3组、D2组与D3组患者改良Lysholm评分比较差异无显著性意义(P > 0.05),其余组间两两比较差异有显著性意义(P < 0.05或P < 0.01)。 2.5 测量方法A与B的比较 因为方法C和D均不是直接反映软组织松弛度的指标,所以在此只比较方法A和B的检验效能。 分析出初步结果后将A、B两组数据进行转化:①规定OKS≤18,改良Lysholm评分≥85时的患者纳入满意组,其他患者纳入不满意组,规定初次分析中功能最好的两组患者为符合组,其余为不符合组,以此将资料调整为两组二分类资料,以交叉表法分别计算测量方法A和B的灵敏度和特异度。方法A的分析结果显示,Pearson卡方=10.514,P=0.001,灵敏度为66.27%,特异度为70.83%;方法B的分析结果,Pearson卡方=12.201,P=0.000,灵敏度为66.67%,特异度为73.91%。测量方法B的灵敏度和特异度均高于方法A。②规定OKS≤18分,改良Lysholm评分≥80分时的患者纳入满意组,其他患者纳入不满意组,其余处理不变。方法A的分析结果显示,Pearson卡方=13.240,P=0.000,灵敏度为64.52%,特异度为71.11%;方法B的分析结果显示,Pearson卡方=10.185,P=0.001,灵敏度为64.81%,特异度为66.04%。方法A的灵敏度略低于方法B但差异较小,特异度高于方法B。"

| [1] JASPER LL, JONES CA, MOLLINS J, et al. Risk factors for revision of total knee arthroplasty: a scoping review. BMC Musculoskelet Disord. 2016;17:182. [2] LÜRING C, BECKMANN J. Custom made total knee arthroplasty : Review of current literature. Orthopade. 2020;49(5):382-389. [3] SEO SS, NHA KW, KIM TY, et al. Survival of total knee arthroplasty after high tibial osteotomy versus primary total knee arthroplasty: A meta-analysis. Medicine (Baltimore). 2019;98(30):e16609. [4] WANG Z, CHENG X, ZHANG Y, et al. Restoration of Constitutional Alignment in TKA with a Novel Osteotomy Technique. J Knee Surg. 2020;33(2):190-199. [5] BLAKENEY W, BEAULIEU Y, PULIERO B, et al. Bone resection for mechanically aligned total knee arthroplasty creates frequent gap modifications and imbalances. Knee Surg Sports Traumatol Arthrosc. 2020;28(5):1532-1541. [6] SASAKI S, SASAKI E, KIMURA Y, et al. Effect of medial collateral ligament release and osteophyte resection on medial laxity in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2020. doi: 10.1007/s00167-020-06257-1. [7] ASANO H, MUNETA T, SEKIYA I. Soft tissue tension in extension in total knee arthroplasty affects postoperative knee extension and stability. Knee Surg Sports Traumatol Arthrosc. 2008;16(11):999-1003. [8] PAXTON EW, FURNES O, NAMBA RS, et al. Comparison of the Norwegian knee arthroplasty register and a United States arthroplasty registry. J Bone Joint Surg Am. 2011;93 Suppl 3:20-30. [9] KAPPEL A, LAURSEN M, NIELSEN PT, et al. Relationship between outcome scores and knee laxity following total knee arthroplasty: a systematic review. Acta Orthop. 2019;90(1):46-52. [10] OH CS, SONG EK, SEON JK, et al. The effect of flexion balance on functional outcomes in cruciate-retaining total knee arthroplasty. Arch Orthop Trauma Surg0 2015;135(3):401-406. [11] LEE BS, CHO HI, BIN SI, et al. Femoral Component Varus Malposition is Associated with Tibial Aseptic Loosening After TKA. Clin Orthop Relat Res0 2018;476(2):400-407. [12] SEON JK, SONG EK, YOON TR, et al. In vivo stability of total knee arthroplasty using a navigation system. Int Orthop. 2007;31(1):45-48. [13] Aunan E, Kibsgård TJ, Diep LM, et al. Intraoperative ligament laxity influences functional outcome 1 year after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 2015;23(6):1684-1692 [14] ALTMAN R, ASCH E, BLOCH D, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986;29(8):1039-1049. [15] SIONG FT, KIM TW, KIM SC, et al. Efficacy and Safety of Functional Medial Ligament Balancing With Stepwise Multiple Needle Puncturing in Varus Total Knee Arthroplasty. J Arthroplasty. 2020;35(2):380-387. [16] LAPRADE RF, HEIKES C, BAKKER AJ, et al. The reproducibility and repeatability of varus stress radiographs in the assessment of isolated fibular collateral ligament and grade-III posterolateral knee injuries. An in vitro biomechanical study. J Bone Joint Surg Am. 2008;90(10):2069-2076. [17] KANE PW, DEPHILLIPO NN, CINQUE ME, et al. Increased Accuracy of Varus Stress Radiographs Versus Magnetic Resonance Imaging in Diagnosing Fibular Collateral Ligament Grade III Tears. Arthroscopy. 2018;34(7):2230-2235. [18] MURER M, FALKOWSKI AL, HIRSCHMANN A, et al. Threshold values for stress radiographs in unstable knees after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2021;29(2):422-428. [19] DEPHILLIPO NN, KANE PW, ENGEBRETSEN L. Stress Radiographs for Ligamentous Knee Injuries. Arthroscopy. 2021;37(1):15-16. [20] GOH GS, BIN ABD RAZAK HR, TAY DK, et al. Early post-operative oxford knee score and knee society score predict patient satisfaction 2 years after total knee arthroplasty. Arch Orthop Trauma Surg. 2021;141(1):129-137. [21] JEONG HS, LEE SC, JEE H, et al. Proprioceptive Training and Outcomes of Patients With Knee Osteoarthritis: A Meta-Analysis of Randomized Controlled Trials. J Athl Train. 2019;54(4):418-428. [22] LIN K, BAO L, WANG J, et al. Validation of the Chinese (Mandarin) Version of the Oxford Knee Score in Patients with Knee Osteoarthritis. Clin Orthop Relat Res. 2017;475(12):2992-3004. [23] SUEYOSHI T, EMOTO G, YATO T. Correlation between Single Assessment Numerical Evaluation score and Lysholm score in primary total knee arthroplasty patients. Arthroplast Today. 2018;4(1):99-102. [24] BRIGGS KK, STEADMAN JR, HAY CJ, et al. Lysholm score and Tegner activity level in individuals with normal knees. Am J Sports Med. 2009;37(5):898-901. [25] BELLEMANS J, VANDENNEUCKER H, VAN LAUWE J, et al. A new surgical technique for medial collateral ligament balancing: multiple needle puncturing. J Arthroplasty. 2010;25(7):1151-1156. [26] SINICROPE BJ, FEHER AW, BHIMANI SJ, et al. Increased Survivorship of Cementless versus Cemented TKA in the Morbidly Obese. A Minimum 5-Year Follow-Up. J Arthroplasty. 2019;34(2):309-314. [27] MONTONEN E, LAAKSONEN I, MATILAINEN M, et al. What Is the Long-term Survivorship of Cruciate-retaining TKA in the Finnish Registry. Clin Orthop Relat Res. 2018;476(6):1205-1211. [28] Courtney PM, Lee GC. Early Outcomes of Kinematic Alignment in Primary Total Knee Arthroplasty: A Meta-Analysis of the Literature. J Arthroplasty 2017;32(6):2028-2032.e1 [29] YONG TM, YOUNG EC, MOLLOY IB, et al. Long-Term Implant Survivorship and Modes of Failure in Simultaneous Concurrent Bilateral Total Knee Arthroplasty. J Arthroplasty. 2020;35(1):139-144. [30] KUSTER MS, BITSCHNAU B, VOTRUBA T. Influence of collateral ligament laxity on patient satisfaction after total knee arthroplasty: a comparative bilateral study. Arch Orthop Trauma Surg. 2004;124(6):415-417. [31] YAMAKADO K, KITAOKA K, YAMADA H, et al. Influence of stability on range of motion after cruciate-retaining TKA. Arch Orthop Trauma Surg. 2003; 123(1):1-4. [32] NAKAHARA H, OKAZAKI K, HAMAI S, et al. Does knee stability in the coronal plane in extension affect function and outcome after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2015;23(6):1693-1698. [33] ARIRACHAKARAN A, CHOOWIT P, PUTANANON C, et al. Is unicompartmental knee arthroplasty (UKA) superior to total knee arthroplasty (TKA)? A systematic review and meta-analysis of randomized controlled trial. Eur J Orthop Surg Traumatol. 2015;25(5):799-806. [34] RUTHERFORD RW, JENNINGS JM, LEVY DL, et al. Revision Total Knee Arthroplasty for Arthrofibrosis. J Arthroplasty. 2018;33(7S):S177-S181. [35] BADE MJ, STRUESSEL T, DAYTON M, et al. Early High-Intensity Versus Low-Intensity Rehabilitation After Total Knee Arthroplasty: A Randomized Controlled Trial. Arthritis Care Res (Hoboken). 2017;69(9):1360-1368. [36] WALKER LC, CLEMENT ND, DEEHAN DJ. Predicting the Outcome of Total Knee Arthroplasty Using the WOMAC Score: A Review of the Literature. J Knee Surg. 2019;32(8):736-741. |
| [1] | Zhang Jichao, Dong Yuefu, Mou Zhifang, Zhang Zhen, Li Bingyan, Xu Xiangjun, Li Jiayi, Ren Meng, Dong Wanpeng. Finite element analysis of biomechanical changes in the osteoarthritis knee joint in different gait flexion angles [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1357-1361. |
| [2] | Jin Tao, Liu Lin, Zhu Xiaoyan, Shi Yucong, Niu Jianxiong, Zhang Tongtong, Wu Shujin, Yang Qingshan. Osteoarthritis and mitochondrial abnormalities [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1452-1458. |
| [3] | Wang Baojuan, Zheng Shuguang, Zhang Qi, Li Tianyang. Miao medicine fumigation can delay extracellular matrix destruction in a rabbit model of knee osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(8): 1180-1186. |
| [4] | Liu Dongcheng, Zhao Jijun, Zhou Zihong, Wu Zhaofeng, Yu Yinghao, Chen Yuhao, Feng Dehong. Comparison of different reference methods for force line correction in open wedge high tibial osteotomy [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(6): 827-831. |
| [5] | Huang Hao, Hong Song, Wa Qingde. Finite element analysis of the effect of femoral component rotation on patellofemoral joint contact pressure in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(6): 848-852. |
| [6] | Yuan Jing, Sun Xiaohu, Chen Hui, Qiao Yongjie, Wang Lixin. Digital measurement and analysis of the distal femur in adults with secondary knee valgus deformity [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(6): 881-885. |
| [7] | Zhou Jianguo, Liu Shiwei, Yuan Changhong, Bi Shengrong, Yang Guoping, Hu Weiquan, Liu Hui, Qian Rui. Total knee arthroplasty with posterior cruciate ligament retaining prosthesis in the treatment of knee osteoarthritis with knee valgus deformity [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(6): 892-897. |
| [8] | He Junjun, Huang Zeling, Hong Zhenqiang. Interventional effect of Yanghe Decoction on synovial inflammation in a rabbit model of early knee osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(5): 694-699. |
| [9] | Lin Xuchen, Zhu Hainian, Wang Zengshun, Qi Tengmin, Liu Limin, Suonan Angxiu. Effect of xanthohumol on inflammatory factors and articular cartilage in a mouse mode of osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(5): 676-681. |
| [10] | Xu Lei, Han Xiaoqiang, Zhang Jintao, Sun Haibiao. Hyaluronic acid around articular chondrocytes: production, transformation and function characteristics [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(5): 768-773. |
| [11] | Zhang Tong, Cai Jinchi, Yuan Zhifa, Zhao Haiyan, Han Xingwen, Wang Wenji. Hyaluronic acid-based composite hydrogel in cartilage injury caused by osteoarthritis: application and mechanism [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(4): 617-625. |
| [12] | Zhang Jian, Lin Jianping, Zhou Gang, Fang Yehan, Wang Benchao, Wu Yongchang. Semi-quantitative MRI evaluation of cartilage degeneration in early knee osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(3): 425-429. |
| [13] | Li Kai, Liu Zhendong, Li Xiaolei, Wang Jingcheng. Risk factors for recurrent prosthesis dislocation after total hip arthroplasty through posterolateral approach [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(3): 354-358. |
| [14] | Wang Chong, Zhang Meiying, Zhou Jian, Lao Kecheng. Early gait changes after total hip arthroplasty through direct anterior approach and posterolateral approach [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(3): 359-364. |
| [15] | Pan Hao, Zhao Huihui, Wang Jiangjing, Wang Feng, Wang Peng, Shi Qiuling, Guo Jin, Li Lin, Liu Guoqiang. Comparison of kinematic alignment and mechanical alignment to guide gait after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(3): 365-370. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||