Chinese Journal of Tissue Engineering Research ›› 2022, Vol. 26 ›› Issue (3): 468-473.doi: 10.12307/2022.077
Previous Articles Next Articles
Development and application of hexapod external fixator in the treatment of lower limb deformity
Zhang Xingdong1, Zhang Yonghong2, Wang Dong2
- 1Shanxi Medical University, Taiyuan 030001, Shanxi Province, China; 2Department of Orthopedics, Second Hospital, Shanxi Medical University, Taiyuan 030001,Shanxi Province, China
-
Received:2021-04-02Revised:2021-04-08Accepted:2021-05-26Online:2022-01-28Published:2021-10-29 -
Contact:Zhang Yonghong, MD, Chief physician, Department of Orthopedics, Second Hospital, Shanxi Medical University, Taiyuan 030001, Shanxi Province, China -
About author:Zhang Xingdong, Master candidate, Shanxi Medical University, Taiyuan 030001, Shanxi Province, China -
Supported by:Shanxi Provincial Social Development Fund, No. 201803D31126 (to ZYH)
CLC Number:
Cite this article
Zhang Xingdong, Zhang Yonghong, Wang Dong. Development and application of hexapod external fixator in the treatment of lower limb deformity[J]. Chinese Journal of Tissue Engineering Research, 2022, 26(3): 468-473.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
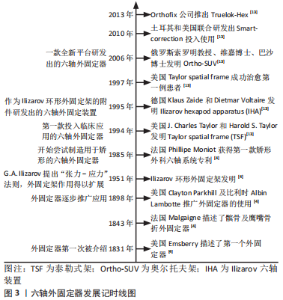
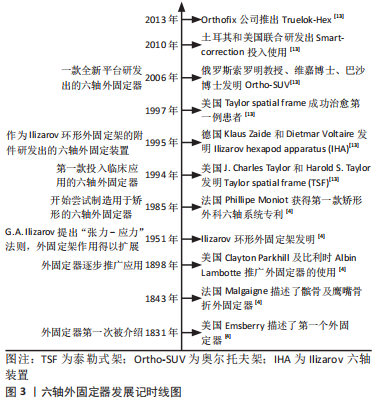
2.1 环形外固定器的起源及应用 2.1.1 环形外固定器的起源 骨外固定技术最早出现于19世纪中叶,是治疗骨折的3大固定技术之一。1831年美国人Emsberry向人们描述了第一个外固定器。1843年法国医生Malgaigne介绍了一种治疗髌骨及鹰嘴骨折的外固定器,该器械形似钳夹,被称为Malgaigne外固定器。随后美国外科医生Clayton Parkhill和比利时外科医生Albin Lambotte在当时推广应用了外固定器。20世纪50年代,随着苏联G.A. Ilizarov教授提出张力-应力法则及Ilizarov环形外固定架的发明,外固定架的应用与发展进入了一个新的阶段[4],见图3。"
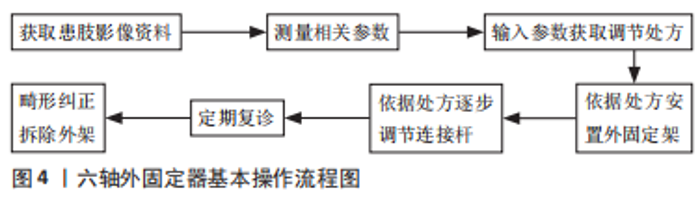
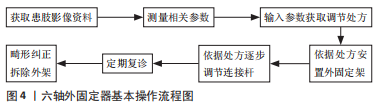
2.1.2 环形外固定器的适应证 目前环形外固定器主要适应证:①各种类型的骨折,特别是伴有较为严重软组织损伤或治疗较晚的开放性骨折、需维持肢体长度的骨折、局部严重烧伤的骨折以及不稳定的骨盆骨折等[4];②各种骨折不愈合、畸形愈合和骨不连;③矫形外科疾病,如骨缺损、感染性骨科疾病和先天性胫骨假关节、胫骨和腓骨缺损等;④关节疾病,如严重膝关节屈曲挛缩畸形和僵硬型马蹄足畸形等。 2.1.3 环形外固定器的特点 早期外固定架的功能及结构较为单一,一般用于临时的骨折固定,在此之后还需行内固 定[4]。伴随张力-应力法则的发现,外固定架的功能与应用得到了极大的发展。而今外固定架已不只是单纯地固定骨折,还可以让骨、血管、神经和皮肤等组织再生,使以前无法治疗的肢体畸形、骨缺损、慢性骨髓炎等疾病得到很好的救治,使人类的诊疗技术得到了拓展。因环形外固定架通过动态调整实现了牵拉骨再生/牵拉组织再生,有文章说环形外固定架是“活”的外固定架。这类外固定架主要的优点如下:①微创治疗,闭合穿针,对软组织及血供影响较小[5];②牵拉治疗过程中实现血管、神经和肌肉等软组织及骨组织再生,软化瘢痕皮肤[6-7];③应用环形外固定架治疗开放性骨折极少发生感染[8],这与内固定治疗形成鲜明对比;同时环形外固定架也可以用于治疗因内固定导致的感染;④环形外固定架稳定性好,术后患肢即可负(持)重,同时可给予患肢轴向应力,利于骨痂的形成,促进骨折愈合[4,9];⑤基于患者的疾病变化进程,可个体化调整外固定架,从而实现了各种疑难骨科疾病的治疗[10-11]。虽然环形外固定架有以上优点,但在使用过程中存在带架治疗周期长、患者复查频次较高等缺点,尤其是在矫正多平面畸形时,需要多次更换外固定器铰链[12],使得带架时间进一步延长。在矫正过程中需多次拍摄X射线平片容易造成额外的X射线暴露,给患者增加经济负担。同时环形外固定架的构型、治疗方案的设计与调整均需要拥有丰富临床经验并熟练掌握环形外固定架的主治医 师[1],因此使用门槛较高,无法快速、广泛的普及。 2.2 六轴外固定器的发展与应用 由于环形外固定架在多平面畸形矫正中存在的缺陷,以及计算机技术的进步,在20世纪90年代中期后,研究人员开发出多种基于计算机导航技术及Stewart和Ceppel平台的六轴外固定器。目前投入临床使用中的六轴外固定系统包括:Taylor spatial frame(美国)、Ilizarov六轴装置(IHA,德国)、Ortho-SUV(俄罗斯)、Smart-Correction(土耳其、美国)和TrueLok-Hex(美国)等[13]。这类外固定器在延续环形外固定架的优点基础上,针对其存在的缺陷进行了改进,并增加了处方软件的应用。这类外固定器的基本操作流程,见图4。"
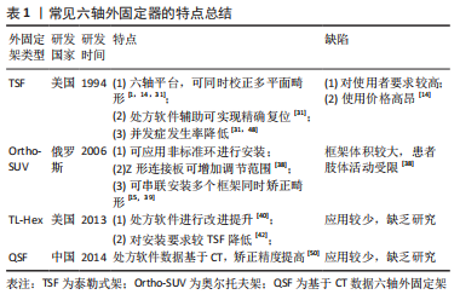
目前应用的六轴外固定器多由两个全环与六根长度可调节伸缩杆组成,这种结构使得这类外固定器具有同时矫正多平面复杂畸形的能力,在配套处方软件的辅助下可实现骨折的精确复位,减少外固定架的带架时间[4,11,13-14]。特别是在足踝部畸形矫正过程中,由于足踝部解剖结构复杂,Ilizarov环形外固定架在矫正过程中需根据矫正情况逐步换关节铰链,造成治疗时间的延长,而六轴外固定器则不需更换铰链,可在安装后直接进行矫正[15-16]。目前六轴外固定器已被证实在四肢畸形矫正、四肢长骨骨折、骨不连及骨缺损等疾病治疗中具有良好的效果[14-27],特别是在下肢畸形的治疗中,与Ilizarov环形外固定架相比,六轴外固定器治疗成功率显著提高,相关并发症的发生率及畸形残留率均显著降低[3]。目前常见六轴外固定器特点,见表1。"
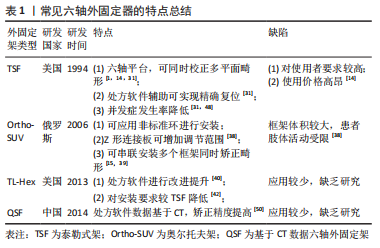
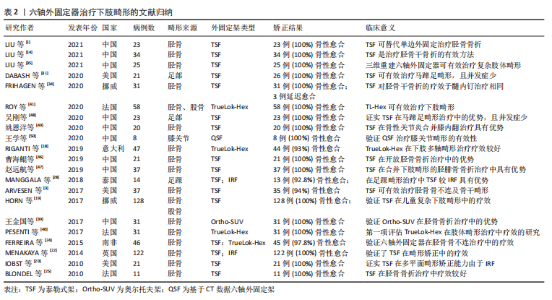
2.2.1 常见六轴外固定器的种类及特点 Taylor空间支架的特点:Taylor空间支架(Taylor spatial frame,TSF;以下简称泰勒式架)是首个在临床中投入使用的六轴外固定器。它是由J.Charles Taylor和Harold S.Taylor于1994年在改良Ilizarov 外固定系统基础上,基于Stewart平台及Chasles理论,研发出Taylor空间支架[28]。在骨折患者的应用中,泰勒式架可以做到闭合复位,从而减少了对骨折周围软组织血运的破坏,降低了骨折不愈合率[5,23]。由于泰勒式架对患处软组织的影响较小,使得患肢骨筋膜室综合征的发生率得到降低[21]。泰勒式架构型简单、易于操作和掌握,在拍摄标准正侧位X射线片后输入相应参数即可由软件生成电子处方。医师只需根据电子处方调节外架即可完成相关疾病的治疗。泰勒式架的畸形矫正是通过调节六根连接杆,使骨段围绕虚拟铰链进行移动而实现的[29]。因此在矫正过程中,泰勒式架仅需更换各种型号的延长杆,不必过多使用铰链[30]。在处方软件的辅助下,其使骨折复位及多平面畸形矫正的准确性大幅提高[31],可以达到解剖复位[21]。理论上讲,其调节精度可达到1/1 000 000英寸和1/10 000°[29],但由于实际应用中无法达到如此的精确,其实际矫正精度为1°和1 mm[32-33]。同环形外固定架相比,泰勒式架的应用大幅减少了患者的带架时间及治疗时间,从而降低了相应并发症的发生率以及治疗过程中患者X射线的暴露风险[5]。 由该综述纳入相关研究及文献文章可以看出,泰勒式架是目前中国外应用最广的六轴外固定器,并在临床治疗中成功治愈了大量骨折、组织缺损、骨折不愈合、下肢畸形等疾病患者,取得了较好的治疗效果,详见表2。"
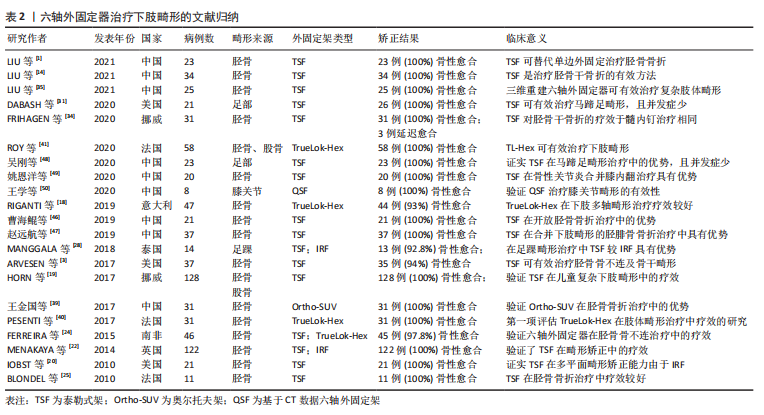
LIU等[14]应用泰勒式架治疗34例高能量胫骨骨折患者均取得了获得了骨折愈合,且对位满意。FRIHAGEN等[34]在治疗胫骨闭合骨折患者时发现泰勒式架的应用可显著避免胫骨畸形愈合,术后膝关节疼痛等并发症发生率也较髓内钉治疗患者低;DABASH等[31]报道24例马蹄内翻足畸形患者通过应用泰勒式架,在不需广泛剥离软组织情况下精确矫正畸形,同时降低了潜在并发症的发生率。可见泰勒式架在下肢畸形治疗中疗效显著,同传统治疗方案相比,可以有效降低术中及术后并发症的发生率。但是在临床工作中,它的广泛使用仍受到诸多的限制:首先泰勒式架的手术操作精度要求较高,其操作手册要求在使用时,参考环必须与参考骨段保持垂直,而在实际操作中,由医师手动安装的外固定很难保证二者完全垂直。其次,泰勒式架在应用标准外固定环时,需精确测量所需的13项参数(包括6项畸形参数、4项安装参数和3项框架参数)并严格按照操作要求进行安装才能达到较好的矫正效果[35]。错误的测量结果、X射线片拍摄不标准以及安装过程中未按照其操作标准进行安装都有可能影响矫正效果[13,33]。 且因调节杆的安装结构特点,泰勒式架在安装后稳定性较差,容易造成患者术后患肢疼痛[13]。另外,泰勒式架价格高昂[14],其配套处方软件的使用需要联网计算机的支持,在手术中使用亦有不便。 Ortho-SUV的特点:奥尔托夫架(Ortho-SUV)是索罗明教授、维嘉博士和巴沙博士于2006年在俄罗斯圣彼得堡伍列登医院,以Ilizarov技术为基础研发出的管状骨环形数字化矫形外固定架[36]。虽然其外型与泰勒式架相似,但操作系统是独特的Solomin-Utehin-Vilenskij(SUV)系统[13]。奥尔托夫架由2个固定环与6根连接杆组成,其中每个固定环只与3个连接杆相连,而另外3根连接杆则与相邻连接杆的侧面相连。这种结构为变铰点结构,而不像泰勒式架或TrueLok-Hex六轴外固定系统将所有铰点均连接在固定环上[37] 。该型外固定器与其他六轴外固定器相比,其连接杆可以与任何可用的环或拱相连,包括Ilizarov环形外固定架、泰勒式架或其他类型外固定架所用到的环。而这种灵活的安装方式则是该型外固定器与其他外固定器相比所具有的最大的优势[15]。另外调节杆和外架相连的连接片长度不受限制,可以定制为直板或Z形板,所以可在较窄的框架内提供更大的调节间隙,增加了畸形的矫正范围,避免经常更换延长杆[38]。然而使用Z型板会占据较大的空间,导致患者行走时外固定架易与对侧肢体发生碰撞,造成行动不便[38]。 与环形外固定架相比,奥尔托夫架最大的优点在于不必针对每个旋转中心分别设计矫正轴,或进行多次不同调节以纠正每个畸形,仅需单一设计框架的串联,即可完成多处畸形矫形的目的,或可以使用2个或多个框架同时进行矫形而互不影响[15,39]。另外临床上观察到该型外固定架稳定性较泰勒式架好,其在使用过程中X射线片的拍摄要求较低,可以不是标准的正侧位片。配套软件内置错误检查机制,以防止由于使用者输入错误的数据而生成错误的电子处方造成治疗失败。在软件应用方面,其配套软件可直接离线使用[15]。目前奥尔托夫架已经在长骨矫形、膝关节挛缩、足踝畸形矫形中取得了较好的治疗效果[15]。但在现阶段可检索到有关文献资料相对较少,在中国应用范围也较小。 其他六轴外固定器的特点:除上述常见的2类六轴外固定器外,目前投入使用的六轴外固定系统还有:德国Ilizarov六轴装置(即IHA),它是由德国骨科医师在1995年以环形外固定架为基础研发而成。该型外固定架矫正环间通过六根调节杆相连,它同泰勒式架相比其优势在于使用球形接头连接调节杆与外固定环,使得其初始稳定性大幅提高;在安装过程中可根据情况选择任一安装位置,无需像泰勒式架必须安装于连接环的固定位置[13]。但由于该型外固定架未得到广泛使用,仅在德国、以色列及巴西有应用。由于相关文献资料较少,故不对其优缺点进行过多评价。 在2012年,由Orthofix公司推出了TrueLok-Hex六轴外固定系统,它由2个圆环或半环组成,六根独立的支撑杆连接,可实现三维度畸形同时矫正。该系统由在线软件即时生成矫正计划,并可根据患者情况在术后及时进行调整。与泰勒式架相比,两者的主要区别就在于用以通过X射线确定肢体延长和分析畸形矫正参数的软件[40]。当患者病情出现变化时,该软件可在不需要外科医师改变外固定器组件的情况下,对患者的矫正计划进行调整[41]。TrueLok-Hex六轴外固定系统在使用过程中允许外科医师采用非垂直于参考骨段的方式进行安装,并据此生成矫正计划[42]。文章检索到的文献资料显示,TrueLok-Hex六轴外固定系统已在下肢骨折、复杂下肢畸形、骨不连及夏科氏足等治疗过程中取得了较好的治疗效果[18,41-42]。有研究报道在阶段性治疗复杂夏科氏足部畸形过程中,通过TrueLok-Hex六轴外固定器可以安全、准确进行矫正,降低对血管及周围软组织的损伤,并为下一阶段治疗奠定基础[17]。还有研究报道在47例复杂下肢畸形合并双下肢长度不均等的患者治疗中,该型六轴外固定器可以很好地矫正下肢畸形,完全矫正率达到90%以上[18]。但目前该型外固定器未引入中国,缺乏相关数据。由于Smart-Correction目前未推广使用,缺乏相关临床研究资料,故文章不作赘述。 2.2.2 六轴外固定器的缺陷 尽管目前所使用的六轴外固定系统在继承Ilizarov环形外固定架的优点基础之上,针对环形外固定架的不足之处做出了许多的改进与提升,但除外固定架应用中常见的并发症外,仍旧存在着一些不足与缺陷: 尽管六轴骨外固定器的应用较Ilizarov环形外固定架简便,但其学习曲线仍较复杂[14],对主治医师的临床经验仍然有着较高的要求。目前,中国应用较多的六轴骨外固定器主要为进口泰勒式架和中国授权仿制品,这2款外固定器与环形外固定架相比,其使用价格高昂,其配套处方软件的在线使用也使得其在术中的应用受到一定限制。"
| [1] LIU Y, LIU J, ZHANG X, et al. Correction outcomes of the postoperative malalignment salvaged by the temporary application of the hexapod external fixator in tibial diaphyseal fractures treated by monolateral external fixation. Injury. 2021. doi: 10.1016/j.injury.2021.01.018. [2] DHAR S, BUTT M, MIR M, et al. Use of the Ilizarov apparatus to improve alignment in proximal humeral fractures treated initially by a unilateral external fixator. Strategies Trauma Limb Reconstr. 2008;3(3):119-122. [3] ARVESEN J, TRACY WATSON J, ISRAEL H. Effectiveness of treatment for distal tibial nonunions with associated complex deformities using a hexapod external fixator. J Orthop Trauma. 2017;31(2):e43-e48. [4] KANI KK, PORRINO JA, CHEW FS. External fixators: looking beyond the hardware maze. Skeletal Radiol. 2020;49(3):359-374. [5] TANG P, HU L, DU H, et al. Novel 3D hexapod computer-assisted orthopaedic surgery system for closed diaphyseal fracture reduction. Int J Med Robot. 2012;8(1):17-24. [6] 扈克治,甘干达,任磊,等.Ilizarov技术治疗长管状骨骨缺损的研究进展[J].创伤外科杂志,2021,23(1):74-77. [7] BORZUNOV D, CHEVARDIN A. Ilizarov non-free bone plasty for extensive tibial defects. Int Orthop. 2013;37(4):709-714. [8] DICKSON D, MOULDER E, HADLAND Y, et al. Grade 3 open tibial shaft fractures treated with a circular frame, functional outcome and systematic review of literature. Injury. 2015;46(4):751-758. [9] HENDERSON D, RUSHBROOK J, et al. What Are the Biomechanical Properties of the Taylor Spatial Frame™? Clin Orthop Relat Res. 2017; 475(5):1472-1482. [10] 贺国宇,张永红,王栋.Ilizarov技术治疗胫骨骨缺损的优势及改进策略[J].中国组织工程研究,2020,24(24):3870-3876. [11] GANADHIEPAN G, MIRAMINI S, harwood pj, et al. Bone fracture healing under Ilizarov fixator: influence of fixator configuration, fracture geometry, and loading. Int J Numer Method Biomed Eng. 2019;35(6): e3199. [12] SIBBEL J, ABDULKARIM A, FISHER R, et al. Eccentric Taylor spatial frame placement for the correction of femoral fracture deformity: a novel technique. Eur J Orthop Surg Traumatol. 2020;30(5):869-875. [13] VILENSKY A, POZDEEV P, BUKHAREV V, et al. Orthopedic hexapods: History, present and prospects (Article). Pediatric Traumatology, Orthopaedics and Reconstructive Surgery. 2015(1):61-69. [14] LIU Y, LIU J, YUSHAN M, et al. Management of high-energy tibial shaft fractures using the hexapod circular external fixator. BMC Surg. 2021;21(1):95. [15] TAKATA M, VILENSKY VA, TSUCHIYA H, et al. Foot deformity correction with hexapod external fixator, the Ortho-SUV Frame™. J Foot Ankle Surg. 2013;52(3):324-330. [16] LIU Y, YUSHAN M, LIU Z, et al. Application of elliptic registration and three-dimensional reconstruction in the postoperative measurement of Taylor spatial frame parameters. Injury. 2020;51(12):2975-2980. [17] WROTSLAVSKY P, KRIGER S, HAMMER-NAHMAN S, et al. Computer-assisted gradual correction of charcot foot deformities: an in-depth evaluation of stage one of a planned two-stage approach to charcot reconstruction. J Foot Ankle Surg. 2020;59(4):841-848. [18] RIGANTI S, NASTO L, MANNINO S, et al. Correction of complex lower limb angular deformities with or without length discrepancy in children using the TL-HEX hexapod system: comparison of clinical and radiographical results. J Pediatr Orthop B. 2019;28(3):214-220. [19] HORN J, STEEN H, HUHNSTOCK S, et al. Limb lengthening and deformity correction of congenital and acquired deformities in children using the Taylor Spatial Frame. Acta Orthop. 2017;88(3):334-340. [20] IOBST C. Limb lengthening combined with deformity correction in children with the Taylor Spatial Frame. J Pediatr Orthop B. 2010;19(6): 529-534. [21] IOBST C. Hexapod external fixation of tibia fractures in children. J Pediatr Orthop. 2016:S24-S28. [22] MENAKAYA C, RIGBY A, HADLAND Y, et al. Fracture healing following high energy tibial trauma: Ilizarov versus Taylor Spatial Frame. Ann R Coll Surg Engl. 2014;96(2):106-110. [23] KESHET D, EIDELMAN M. Clinical utility of the Taylor spatial frame for limb deformities. Orthop Res Rev. 2017;9:51-61. [24] FERREIRA N, MARAIS LC, ALDOUS C. Hexapod external fixator closed distraction in the management of stiff hypertrophic tibial nonunions. Bone Joint J. 2015;97-b(10):1417-1422. [25] BLONDEL B, LAUNAY F, GLARD Y, et al. Hexapodal external fixation in the management of children tibial fractures. J Pediatr Orthop B. 2010;19(6):487-491. [26] AHREND MD, RÜHLE M, SPRINGER F, et al. Distance from the magnification device contributes to differences in lower leg length measured in patients with TSF correction. Arch Orthop Trauma Surg. 2021. doi: 10.1007/s00402-021-03831-1. [27] CHAVOSHNEJAD P, AYATI M, ABBASSPOUR A, et al. Optimization of Taylor spatial frame half-pins diameter for bone deformity correction: application to femur. Proc Inst Mech Eng H. 2018;232:673-681. [28] MANGGALA Y, ANGTHONG C, PRIMADHI A, et al. The deformity correction and fixator-assisted treatment using Ilizarov versus Taylor spatial frame in the foot and ankle. Orthop Rev (Pavia). 2018;(4):7337. [29] GANTSOUDES G, FRAGOMEN A, ROZBRUCH S. Intraoperative measurement of mounting parameters for the Taylor Spatial Frame. J Orthop Trauma. 2010;24(4):258-262. [30] 王亚洲,徐佳,康庆林.Taylor空间支架的临床应用进展[J].中国矫形外科杂志,2014,22(19):1773-1777. [31] DABASH S, POTTER E, CATLETT G, et al. Taylor spatial frame in treatment of equinus deformity. Strategies Trauma Limb Reconstr. 2020;15(1):28-33. [32] LIU Z, TANG G, GUO S, et al. Effects of Taylor Spatial Frame on tumors and tumor-like lesions with pathological fractures of lower extremities. Pak J Med Sci. 2018;34:440-445. [33] GESSMANN J, FRIELER S, KÖNIGSHAUSEN M, et al. Accuracy of radiographic measurement techniques for the Taylor spatial frame mounting parameters. BMC Musculoskelet Disord. 2021;22(1):284. [34] FRIHAGEN F, MADSEN JE, SUNDFELDT M, et al. Taylor spatial frame or reamed intramedullary nailing for closed fractures of the tibial shaft: a randomized controlled trial. J Orthop Trauma. 2020;34(11):612-619. [35] LIU Y, LI H, LIU J, et al. Long bone fracture reduction and deformity correction using the hexapod external fixator with a new method: a feasible study and preliminary results. BMC Musculoskelet Disord. 2021;22(1):221. [36] 刘长山.俄罗斯骨科奥尔托夫(Ortho-SUV)技术在创伤骨科应用现状[J].转化医学杂志,2013,2(6):366-3669. [37] 傅超,范佳程,王石刚,等.Ortho-SUV支架空间位姿建模与求解[J].上海交通大学学报,2020,54(10):1007-1014. [38] SKOMOROSHKO PV, VILENSKY VA, HAMMOUDA AI, et al. Determination of the maximal corrective ability and optimal placement of the Ortho-SUV frame for femoral deformity with respect to the soft tissue envelope, a biomechanical modelling study. Adv Orthop. 2014; 2014:268567. [39] 王金国,闫秀中,韦庆申,等.计算机辅助Ortho-SUV外固定支架用于开放性胫腓骨骨折患者效果观察[J].山东医药,2017,57(40): 72-74. [40] PESENTI S, IOBST C, LAUNAY F. Evaluation of the external fixator TrueLok Hexapod System for tibial deformity correction in children. Orthop Traumatol Surg Res. 2017;103(5):761-764. [41] ROY A, PESENTI S, CHALOPIN A, et al. Can the TrueLok Hexapod System™ be used to accurately correct lower limb deformity in children? Orthop Traumatol Surg Res. 2020;106(7):1361-1366. [42] FERREIRA N, BIRKHOLTZ F. Radiographic analysis of hexapod external fixators: fundamental differences between the Taylor Spatial Frame and TrueLok-Hex. J Med Eng Technol. 2015;39(3):173-176. [43] BAUMGARTNER H, GRÜNWALD L, AHREND MD. The application of the taylor spatial frame for deformity correction at the lower extremity. Z Orthop Unfall. 2020;158(4):414-416. [44] AHREND MD, FINGER F, GRÜNWALD L, et al. Improving the accuracy of patient positioning for long-leg radiographs using a Taylor Spatial Frame mounted rotation rod. Arch Orthop Trauma Surg. 2021;141(1):55-61. [45] AL-UZRI M, THAHIR A, ABDULKARIM A, et al. Improving radiographic imaging for circular frames: the Cambridge experience. Arch Orthop Trauma Surg. 2020;140(12):1965-1970. [46] 曹海鲲,万春友,姚辉,等.计算机辅助Taylor空间支架治疗开放性胫腓骨骨折[J].中国矫形外科杂志,2019,27(4):331-335. [47] 赵远航,万春友,张涛,等.Taylor空间支架外固定治疗闭合性胫腓骨骨折合并膝内翻畸形[J].中医正骨,2019,31(10):60-62. [48] 吴刚,陈建文,郭悦,等.后足截骨结合泰勒空间外固定支架矫正严重马蹄足畸形临床研究[J].足踝外科电子杂志,2020,7(1):1-5,38. [49] 姚恩洋,田野.胫骨高位截骨联合Taylor外固定架治疗膝骨性关节炎并膝内翻的临床疗效[J].中国医科大学学报,2020,49(7):597-600, 605. [50] 王学,乔锋,刘曙光.基于CT数据六轴数字化骨科外固定架在膝关节复杂畸形中的临床应用[J].实用骨科杂志,2020,26(12): 1118-1122. |
| [1] | Shi Yao, Han Shufeng, Yuan Yitong, Du Ruochen, Jing Zhijie, Zhao Bichun, Zhang Ruxin, Zhang Yujuan, Wang Chunfang. Efficacy and safety of human umbilical cord mesenchymal stem cells in the treatment of spinal cord injury: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(25): 4093-4100. |
| [2] | Xu Jie, Zhou Wenqi, Luo Xiaobing. Visual analysis of patellofemoral pain syndrome research hotspots and content [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(12): 1877-1887. |
| [3] | Lü Shuaiyao, Guan Haishan, Hao Chen, Ding Zhuangzhi. Cervical spondylotic amyotrophy: problems about classification, diagnosis, treatment, and prognosis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(11): 1788-1792. |
| [4] | Zhang Xinlong, Ci Wentao, Luo Kaiwen, Yan shi. Internal fixation failure after proximal femoral nail antirotation: causes and reoperation strategies [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(6): 973-979. |
| [5] | Liu Yubo, Zhang Huizeng, Zhang Tongrun, Sui Gengyi, Ma Nan, Cheng Xu, Gao Xupeng, Xu Jing, Wang Chaoliang. Correlation analysis between the morphological changes of ankle acupoints and the ankle function after ankle fracture surgery [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(3): 440-445. |
| [6] | Liu Zemin, Lü Xin. Application of intramedullary nailing in the treatment of long tubular bone fractures of the extremities: reaming and non-reaming [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(3): 461-467. |
| [7] | Zhang Qiang, Yue Xianhu, Zhang Shu, Gu Mingyong, Li Rui. Biomechanical properties of the OmniSpan device versus the RapidLoc device for meniscus repair [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(36): 5777-5781. |
| [8] | Chen Chaofeng, He Dadong, Liang Jincheng, He Zhijun. Predicting the possibility of blood transfusion after total knee arthroplasty based on machine learning algorithm [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(36): 5792-5797. |
| [9] | Xiong Chen, He Guiping, Zhang Kun, He Xiao, Yang Jiarui, He Changjun, Wang Xiaolong, Wang Chen, Shi Zhengwei, Zhu Yangjun, Heng Lisong. Conservative treatment, open reduction, percutaneous minimally invasive plate internal fixation and intramedullary nail fixation in the treatment of humeral shaft fractures: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(36): 5878-5887. |
| [10] | Wan Dadi, Duan Xiangrui, Fan Xinchao, Yuan Ye, Huang Teng, Pan Dikang, Liu Jingyan, Li Xicheng. Efficacy of posterior cruciate ligament retaining versus posterior stabilized prostheses in total knee arthroplasty: a systematic review and a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(36): 5897-5904. |
| [11] | Zhang Feng. Long-term effects and adverse events of polyetheretherketone versus titanium mesh materials in repairing skull defects: a prospective, single-center, non-randomized controlled, 2-year follow-up clinical trial protocol [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(34): 5501-5505. |
| [12] | Yang Jiujie, Wang Tao, Li Zhi, Yang Lifeng, Tian Ye, Bi Zheng, Zeng Yaling. Cervical spondylosis with osteoporosis treated by the new pedicle fixation system through the anterior cervical approach with three-dimensional printing technology: three-dimensional finite element analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(33): 5249-5253. |
| [13] | Gu Jinshan, Yang Chaohui, Li Shuwei. Mechanical difference between anterior approach and anterior combined with posterior approach in the treatment of acetabular both-column fractures [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(33): 5254-5258. |
| [14] | Qiao Renqiu, Yin Li, Zhang Yi, Wang Haitao, Xia Peige, Kong Zhiheng. Medium- and long-term assessment of lateral compartment and patellofemoral compartment osteoarthritis after medial unicompartmental knee arthroplasty with Oxford mobile-bearing [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(33): 5318-5323. |
| [15] | Gao Yuan, Xia Tienan, Liu Jinxin, Shang Guanning. Effect of muscle flap in limb salvage operation of tumor type prosthesis of proximal tibia [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(33): 5329-5334. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||