Chinese Journal of Tissue Engineering Research ›› 2021, Vol. 25 ›› Issue (26): 4217-4222.doi: 10.12307/2021.124
Previous Articles Next Articles
Reconstruction of medial patellofemoral ligament: selection of single- and double-bundle graft and fixation technique of patellar and femoral insertion point
Lin Chaosheng, Liu Yuwei, Zhu Weimin, Xiong Jianyi
- Second Clinical College of Anhui Medical University, Shenzhen Second People’s Hospital, Shenzhen 518000, Guangdong Province, China
-
Received:2020-06-22Revised:2020-06-30Accepted:2020-08-28Online:2021-09-18Published:2021-05-12 -
Contact:Xiong Jianyi, Master, Chief physician, Second Clinical College of Anhui Medical University, Shenzhen Second People’s Hospital, Shenzhen 518000, Guangdong Province, China -
About author:Lin Chaosheng, Master candidate, Physician, Second Clinical College of Anhui Medical University, Shenzhen Second People’s Hospital, Shenzhen 518000, Guangdong Province, China
CLC Number:
Cite this article
Lin Chaosheng, Liu Yuwei, Zhu Weimin, Xiong Jianyi. Reconstruction of medial patellofemoral ligament: selection of single- and double-bundle graft and fixation technique of patellar and femoral insertion point[J]. Chinese Journal of Tissue Engineering Research, 2021, 25(26): 4217-4222.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
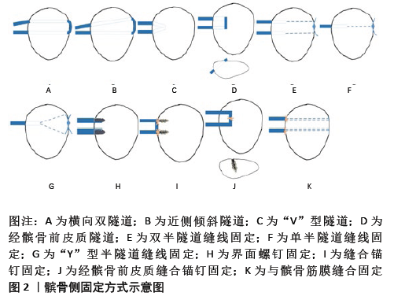
2.1 MPFL解剖 MPFL是一个由股骨侧向髌骨侧放射的扇形结构[9],包含上斜束和下直束双束结构。研究表明,上、下束是两个功能独立的区域[10-11],受到的应力各不相同。与单束重建比较,双束重建能更好地模拟MPFL的机械功能[12]。髌骨关节的内侧稳定装置除了MPFL,还包括内侧髌胫韧带和内侧髌半月板韧带。既往研究普遍认为MPFL在内侧稳定装置中起最为重要的作用,重建MPFL也是治疗髌骨脱位的有效治疗方案[13]。然而,LAPRADE等[13]发现MPFL和内侧髌胫韧带具有相似的平均刚度、破坏应力和破坏载荷,这表明内侧髌胫韧带对内侧稳定装置也可能具有重要作用。内侧髌半月板韧带的机械特性也提示了其在内侧稳定结构中有着潜在的作用。在开始的屈膝30°过程中,MPFL对于抵抗髌骨外侧移位和外侧倾斜非常重要,提供了髌骨内侧稳定结构的总约束力的50%-60%[13-15]。重建MPFL的目标是在膝关节屈伸时为髌骨外侧移位提供内侧约束应力,并引导髌骨到滑车沟中[16]。 2.2 单独MPFL重建适应证 受到解剖异常的影响,进行单独MPFL重建有一定的局限性。然而,大量研究对单独MPFL重建并没有一个明确的适应证[17-18]。对于骨性结构发育异常、软组织缺陷或为了加强内侧稳定结构等原因,临床医生们常常会合并有其他术式,如胫骨结节-滑车沟距离过大(大于20 mm)或高位髌骨(Caton指数>1.2)患者可联合胫骨结节远端或内侧移位术;矫正滑车形态异常的滑车成形术;不通过在滑车形成凹槽而是在不改变髌股结合的情况下减少髌骨突出的滑车后缩楔形截骨术及股骨去旋截骨术;平衡外侧支持带张力的外侧支持带松解术及外侧支持带成形术[16,19-24]。是否进行单独MPFL重建主要是对TT-TG、高位髌骨、滑车发育不良、Q角进行考虑,结合大部分研究总结了不需要进行骨性手术的标准:①胫骨结节-滑车沟距离< 20 mm;②Caton指数< 1.2;③滑车发育不良Dejour分级为A、B级;④Q 角< 20°[17-18]。此外,ERICKSON等[25]对90例接受不伴有其他合并术式的MPFL重建术患者进行了1年和2年的早期随访,提出了即使有胫骨结节-滑车沟距离过大、滑车发育不良、高位髌骨等因素,接受单独MPFL重建术的患者其再脱位率及不稳定率都有较大程度的改善。考虑到大多数患者骨骺未闭合,为了避免对其生长的影响,可以适当放宽合并骨性手术的指征,进行单独MPFL重建。临床上,对于髌骨脱位患者,无论有无解剖结构的异常,都需要进行MPFL重建,改善其膝关节功能及减小再脱位率。同时,需要进一步高质量研究来制定标准化的临床和影像学标准,作为选择合适患者进行单独MPFL重建的指南,并优化患者的预后。 2.3 MPFL的重建 到目前为止,重建MPFL的手术方式众多,多达上百种,许多文献都提出了具有较好临床预后的重建方法,但还没有一种技术被认为是重建MPFL的“金标准”,大部分术式都能很好地改善患者的功能评分,但是不同术式的再脱位率和并发症发生率存在差别,具有各自的优劣势。MPFL重建方法的区别主要在于移植物单双束的选择、股骨侧及髌骨侧固定方式的选择。 MPFL双束解剖重建在解剖特征方面更加符合天然的MPFL扇形结构[9]。WANG等[26]通过对成人膝关节标本进行研究,发现单束和双束MPFL重建都可以恢复髌骨的稳定性。双束重建具有角度协同效应,在屈曲角度较小时重建双束MPFL能够重现自然情况下MPFL的生物力学,使得髌骨在进入股骨滑车前具有更大的抵抗髌骨外移的能力。同时,有一些临床研究表明,与单束重建相比,双束重建在长期随访中获得了更好的临床结果[27]。 股骨插入点的选择可以通过术中手法触摸定位在内收肌结节与股骨内侧髁中点处,以及术中透视精准定位,大多数研究者还是采用在术中透视下股骨解剖止点用7 mm钻头钻取40 mm长的隧道,然后使用生物可吸收界面螺钉固定[28]。MOCHIZUKI等[29]使用和移植物直径相同的钻头从股骨插入点钻孔约30 mm,然后使用直径4.5 mm的钻头向股骨外侧形成贯通隧道,将移植物及可调节的皮质固定系统翻转通过隧道,将可调节皮质固定系统固定在股骨外侧。此外,LEAL-BLANQUET等[30]在MPFL重建术中采用了不需要在股骨钻隧道及放置固定装置的软组织固定法,将重建的移植物拉至股骨内侧并环绕内收肌远端进行缝合固定。KUMAHASHI等[31]在内侧副韧带近端后1/3处切开 1 cm,将该切口作为股骨侧固定点,移植物一端绕过切口后再返回到髌骨进行固定。对60例患者进行一两年的术后随访,LIND等[32]发现股骨软组织固定技术与界面螺钉技术无明显差异,软组织技术也可以安全地运用于MPFL重建。 各种MPFL重建的区别主要在于髌骨侧移植物的固定方式不同,可以大致分为骨隧道、缝合锚钉固定和软组织缝合固定3类。 2.3.1 髌骨隧道固定 比较常用的髌骨隧道固定方式是在髌骨上采用横向双隧道进行固定,见图2A,在髌骨近2/3处用4.5 mm钻头钻出2个横向隧道,隧道相距10-15 mm,移植物以环状方式穿过隧道,结果显示44例患者Kujala评分较术前明显提高以及较低的再脱位率,但由于钻孔导致骨皮质变弱也有患者出现了髌骨骨折的并发症[33]。PANNI等[28]在其技术中进行了改良,见图2B,在髌骨内缘中点钻1条水平隧道,近端10 mm处钻向髌骨外侧和近侧倾斜的隧道,这样的隧道能减少上束支在插入点处的剪切力,但同时由于上隧道的倾斜,移植物所需长度也相应增加,在2年的随访中取得了明显的膝关节评分改善且无再发脱位。使用双隧道重建MPFL时,因为重建的MPFL比天然的MPFL更坚强,刚度更大,在生物力学上远强于人体髌股关节活动的需要,所以因移植物定位错位而增加髌股接触压力的问题会更加严重。为了避免横穿整个髌骨的隧道技术带来的骨折并发症,AHMAD等[34]采用了在髌骨内侧形成V形隧道的术式,见图2C,通过斜向钻孔,将两隧道在髌骨内进行交汇,形成“V”型,将移植物拉入V形隧道固定,避免了破坏髌骨的外侧皮质,但还是存在着隧道爆裂的风险,所以在使用该技术时需要保证内侧两孔之间骨桥距离大于10 mm。HINTERWIMMER等[35]也考虑到了长隧道会产生更大的髌骨骨折风险,所以选择了经髌骨前皮质的双隧道技术,见图2D,两隧道从髌骨内侧穿向髌骨前皮质,移植物穿过髌骨前皮质进行固定,15个月内随访的19例患者无再脱位,膝关节功能评分得到明显改善,重返运动评分也较术前提高,鉴于随访时间较短,该术式对髌骨前皮质损伤引起的潜在风险也值得注意。通过生物力学研究,确保了半隧道技术能够提供足够大的破坏载荷,NIU等[36]通过双半隧道缝线固定技术对两股与四股移植物的临床预后进行了分组随访研究,见图2E,结果显示四股移植物预后优于两股移植物,但是差异较小,无临床统计学差异,所有患者的髌骨外倾角都得到了明显改善,且无再脱位发生,NIU等[36]认为不管是两股还是四股移植物,使用双半隧道缝合技术都能够提供足够的MPFL破坏载荷,对重建后的髌骨关节稳定有明显优势,同时也避免了长隧道带来的高髌骨骨折并发症发生率。类似的半隧道重建技术还有Ellera GOMES等[37]采用的单隧道缝合重建,见图2F,13例(87%)患者都对自己手术结果感到满意,根据Crosby-Insall标准进行主观评价后发现1例患者出现髌骨轨迹异常、髌股疼痛和恐惧试验阳性。AHMAD等[38]进行的单隧道缝合技术则略有不同,采用的是“Y”型半隧道,见图2G,同样是在髌骨外侧进行缝合打结固定,18例患者IKDC主观膝关节评估、Lysholm评分、吉隆坡评分和Tegner评分从术前到最近1次随访均有统计学上的改善,除了术后1例患者出现膝关节僵直外,无其他并发症的发生。由于挤压螺钉固定技术也是在髌骨侧形成了较大的半隧道后再将移植物拉入用界面螺钉挤压固定,见图2H,故将其归类为隧道技术,使用该技术也能提供足够的腱骨愈合以及较大的移植物破坏载荷,由于固定强度足够大,所以早期就能进行关节全范围活动的康复锻炼,减少了关节僵硬的发生[39]。"
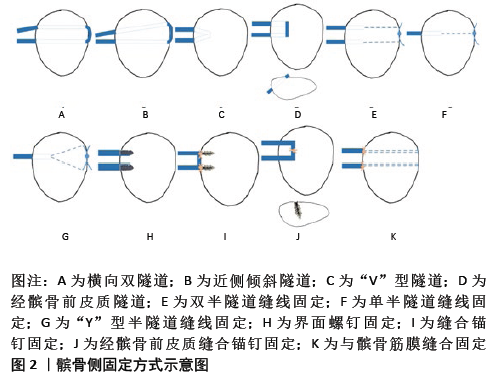

2.3.2 缝合锚钉固定 缝合锚钉固定技术与界面螺钉固定相同,都需要在髌骨放置内植物进行固定,但侵袭性相对小。SCHOTTLE等[40]在髌骨内侧形成骨槽,将带有缝线的2枚缝合锚钉置入骨槽的近端和远端,将移植物中间段嵌入骨槽并缝合到锚钉上进行固定,见图2I,86%的患者认为手术改善了他们的膝关节,1例患者出现了影响其生活的膝关节剧烈疼痛。SONG等[41]则是对锚钉固定进行了改良,在将移植物与锚钉的一条缝线缝合固定后,另一条缝线将移植物与周围软组织(内侧支持带及残留的MPFL)缝合固定,在至少2年的随访中,所有评估的临床评分和放射学参数都有明显的改善。WANG等[42]考虑到在髌骨内侧向外侧钻孔可能是造成髌骨骨折的危险因素,所以选择在髌骨前皮质插入单枚锚钉进行固定来降低内侧边缘骨折的风险,在髌骨前皮质近侧1/3处和内侧1/4处形成2 cm长的骨槽,骨槽中点置入直径3 mm锚钉,钻孔的方向是根据髌骨形态确定了安全角之后形成的,移植物置入骨槽,中间与锚钉固定,然后将骨槽周围骨膜和深筋膜覆盖缝合,见图2J,该技术使用了骨槽可以起到腱骨愈合的作用,鉴于使用双锚钉也会有髌骨骨折的风险,该术式中只使用了1枚锚钉,减少对髌骨血液供应的影响,确实在其随访的26例患者中均未发生髌骨骨折,使用该技术值得注意的一点是安全角的选择,通常女性髌骨较男性更小、更薄,钻孔的方向建议小于安全角,避免钻孔过深,损伤了髌股关节。与隧道固定技术相比,缝合锚钉固定技术有几个潜在的优势[18]。首先,髌骨隧道可能使髌骨的应力提升,而锚钉固定技术通过创造骨槽而不是骨隧道来降低髌骨骨折的潜在风险;其次,它为短肌腱提供了重建MPFL的可能性,因为不需要通过骨隧道来固定移植物。 2.3.3 软组织缝合固定 KANG等[43]对比了两种移植物与髌骨筋膜缝合固定技术,第1组使用的是C形移植物,将移植物两游离端分别用缝线缝合加强,用咬骨钳在髌骨内侧缘上半部形成骨槽,移植物中段置于骨槽内,移植物游离端分别位于髌骨内侧缘的中点和近侧端,在骨槽两端和中点分别将移植物与髌前筋膜缝合固定;第2组使用的是Y形移植物,将移植物中段折叠缝合,先将折叠端在股骨插入点用界面螺钉进行固定,再将两游离端分别经髌骨内缘中点和近端穿过髌骨筋膜,然后游离端从筋膜前折返与自身进行缝合固定。在至少2年的随访中,两组之间没有显著的统计学差异。SIEBOLD等[44]将缝线穿过克氏针钻的小孔来固定移植物,首先在髌骨内缘钻1条浅的骨槽,骨槽两端靠近髌骨内缘上角和髌骨内侧缘的中心,用1.6 mm克氏针从骨槽内侧穿到外侧钻4个小骨道,将2根2号不可吸收线分别从髌骨内侧带至外侧,再从另一孔带回髌骨内侧,肌腱中间段固定在骨槽中,在髌骨外侧骨槽处缝线打结固定,见图2K。软组织缝合固定技术既不需要大的骨隧道,也不用放置内植物进行固定,避免了可能导致髌骨骨折及异物反应。通过生物力学研究,软组织缝合技术重建的MPFL强度并不低于天然MPFL和缝合锚钉固定技术,临床上许多随访研究结果显示患者术后Lysholm、Kuajla评分和锚钉固定技术一样好[44],这也缓和了大家对软组织缝合固定技术的一些担忧。"

| [1] ABBASI D, MAY MM, WALL EJ, et al. MRI findings in adolescent patients with acute traumatic knee hemarthrosis. J Pediatr Orthop. 2012;32(8):760-764. [2] STEFANCIN JJ, PARKER RD. First-time traumatic patellar dislocation: a systematic review. Clin Orthop Relat Res. 2007;455:93-101. [3] FELUS J, KOWALCZYK B. Age-related differences in medial patellofemoral ligament injury patterns in traumatic patellar dislocation: case series of 50 surgically treated children and adolescents. Am J Sports Med. 2012;40(10):2357-2364. [4] FITHIAN DC, PAXTON EW, STONE ML, et al. Epidemiology and natural history of acute patellar dislocation. Am J Sports Med. 2004;32(5): 1114-1121. [5] POST WR. Clinical evaluation of patients with patellofemoral disorders. Arthroscopy. 1999;15(8):841-851. [6] ZHANG Z, ZHANG H, SONG G, et al. A High-Grade J Sign Is More Likely to Yield Higher Postoperative Patellar Laxity and Residual Maltracking in Patients With Recurrent Patellar Dislocation Treated With Derotational Distal Femoral Osteotomy. Am J Sports Med. 2020;48(1):117-127. [7] BEST MJ, TANAKA MJ, DEMEHRI S, et al. Accuracy and Reliability of the Visual Assessment of Patellar Tracking. Am J Sports Med. 2020;48(2): 370-375. [8] ELIAS JJ, SOEHNLEN NT, GUSEILA LM, et al. Dynamic tracking influenced by anatomy in patellar instability. Knee. 2016;23(3):450-455. [9] AMIS AA, FIRER P, MOUNTNEY J, et al. Anatomy and biomechanics of the medial patellofemoral ligament. Knee. 2003;10(3):215-220. [10] SONG SY, PANG CH, KIM CH, et al. Length change behavior of virtual medial patellofemoral ligament fibers during in vivo knee flexion. Am J Sports Med. 2015;43(5):1165-1171. [11] VICTOR J, WONG P, WITVROUW E, et al. How isometric are the medial patellofemoral, superficial medial collateral, and lateral collateral ligaments of the knee? Am J Sports Med. 2009;37(10):2028-2036. [12] HUBER C, ZHANG Q, TAYLOR WR, et al. Properties and Function of the Medial Patellofemoral Ligament: A Systematic Review. Am J Sports Med. 2020;48(3):754-766. [13] LAPRADE MD, KALLENBACH SL, AMAN ZS, et al. Biomechanical Evaluation of the Medial Stabilizers of the Patella. Am J Sports Med. 2018;46(7):1575-1582. [14] PHILIPPOT R, BOYER B, TESTA R, et al. The role of the medial ligamentous structures on patellar tracking during knee flexion. Knee Surg Sports Traumatol Arthrosc. 2012;20(2):331-336. [15] KRUCKEBERG BM, CHAHLA J, MOATSHE G, et al. Quantitative and Qualitative Analysis of the Medial Patellar Ligaments: An Anatomic and Radiographic Study. Am J Sports Med. 2018;46(1):153-162. [16] REAGAN J, KULLAR R, BURKS R. MPFL reconstruction: technique and results. Orthop Clin North Am. 2015;46(1):159-169. [17] YEUNG M, LEBLANC MC, AYENI OR, et al. Indications for Medial Patellofemoral Ligament Reconstruction: A Systematic Review. J Knee Surg. 2016;29(7):543-554. [18] LONGO UG, BERTON A, SALVATORE G, et al. Medial Patellofemoral Ligament Reconstruction Combined With Bony Procedures for Patellar Instability: Current Indications, Outcomes, and Complications. Arthroscopy. 2016;32(7):1421-1427. [19] NERI T, PARKER DA, BEACH A, et al. Medial patellofemoral ligament reconstruction with or without tibial tubercle transfer is an effective treatment for patellofemoral instability. Knee Surg Sports Traumatol Arthrosc. 2019;27(3):805-813. [20] MULLIEZ A, LAMBRECHT D, VERBRUGGEN D, et al. Clinical outcome in MPFL reconstruction with and without tuberositas transposition. Knee Surg Sports Traumatol Arthrosc. 2017;25(9):2708-2714. [21] NELITZ M, DREYHAUPT J, LIPPACHER S. Combined trochleoplasty and medial patellofemoral ligament reconstruction for recurrent patellar dislocations in severe trochlear dysplasia: a minimum 2-year follow-up study. Am J Sports Med. 2013;41(5):1005-1012. [22] THAUNAT M, BESSIERE C, PUJOL N, et al. Recession wedge trochleoplasty as an additional procedure in the surgical treatment of patellar instability with major trochlear dysplasia: early results. Orthop Traumatol Surg Res. 2011;97(8):833-845. [23] IMHOFF FB, COTIC M, LISKA F, et al. Derotational osteotomy at the distal femur is effective to treat patients with patellar instability. Knee Surg Sports Traumatol Arthrosc. 2019;27(2):652-658. [24] LIU C, DUAN G, NIU Y, et al. Lateral retinaculum plasty instead of lateral retinacular release with concomitant medial patellofemoral ligament reconstruction can achieve better results for patellar dislocation. Knee Surg Sports Traumatol Arthrosc. 2018;26(10):2899-2905. [25] ERICKSON BJ, NGUYEN J, GASIK K, et al. Isolated Medial Patellofemoral Ligament Reconstruction for Patellar Instability Regardless of Tibial Tubercle-Trochlear Groove Distance and Patellar Height: Outcomes at 1 and 2 Years. Am J Sports Med. 2019;47(6):1331-1337. [26] WANG Q, HUANG W, CAI D, et al. Biomechanical comparison of single- and double-bundle medial patellofemoral ligament reconstruction. J Orthop Surg Res. 2017;12(1):29. [27] WANG CH, MA LF, ZHOU JW, et al. Double-bundle anatomical versus single-bundle isometric medial patellofemoral ligament reconstruction for patellar dislocation. Int Orthop. 2013;37(4):617-624. [28] PANNI AS, ALAM M, CERCIELLO S, et al. Medial patellofemoral ligament reconstruction with a divergent patellar transverse 2-tunnel technique. Am J Sports Med. 2011;39(12):2647-2655. [29] MOCHIZUKI Y, KANEKO T, KAWAHARA K, et al. A 2-year follow-up of isolated Medial Patellofemoral Ligament Reconstruction by using soft suture anchor and adjustable cortical fixation system. J Orthop. 2019;16(4):356-360. [30] LEAL-BLANQUET J, ALENTORN-GELI E, TORRES-CLARAMUNT R, et al. Partial quadriceps tendon transfer for revision medial patellofemoral ligament reconstruction: A new surgical technique. Acta Orthop Traumatol Turc. 2017;51(3):258-261. [31] KUMAHASHI N, KUWATA S, TADENUMA T, et al. A “sandwich” method of reconstruction of the medial patellofemoral ligament using a titanium interference screw for patellar instability in skeletally immature patients. Arch Orthop Trauma Surg. 2012;132(8):1077-1083. [32] LIND M, NIELSEN T, MILLER L, et al. No Difference in Outcome Between Femoral Soft-Tissue and Screw Graft Fixation for Reconstruction of the Medial Patellofemoral Ligament: A Randomized Controlled Trial. Arthroscopy. 2019;35(4):1130-1137. [33] CHRISTIANSEN SE, JACOBSEN BW, LUND B, et al. Reconstruction of the medial patellofemoral ligament with gracilis tendon autograft in transverse patellar drill holes. Arthroscopy. 2008;24(1):82-87. [34] AHMAD R, JAYASEKERA N, SCHRANZ P, et al. Medial patellofemoral ligament reconstruction: a technique with a “v”-shaped patellar tunnel. Arthrosc Tech. 2014;3(5):e589-592. [35] HINTERWIMMER S, IMHOFF AB, MINZLAFF P, et al. Anatomical two-bundle medial patellofemoral ligament reconstruction with hardware-free patellar graft fixation: technical note and preliminary results. Knee Surg Sports Traumatol Arthrosc. 2013;21(9):2147-2154. [36] NIU J, LIN W, QI Q, et al. Anatomical Medial Patellofemoral Ligament Reconstruction for Recurrent Patella Dislocation: Two-Strand Grafts versus Four-Strand Grafts. J Knee Surg. 2021;34(2):147-154. [37] ELLERA GOMES JL, STIGLER MARCZYK LR, CÉSAR DE CÉSAR P, et al. Medial patellofemoral ligament reconstruction with semitendinosus autograft for chronic patellar instability: a follow-up study. Arthroscopy. 2004;20(2):147-151. [38] AHMAD CS, BROWN GD, SHUBIN STEIN BE. The docking technique for medial patellofemoral ligament reconstruction: surgical technique and clinical outcome. Am J Sports Med. 2009;37(10):2021-2027. [39] SCHÖTTLE PB, HENSLER D, IMHOFF AB. Anatomical double-bundle MPFL reconstruction with an aperture fixation. Knee Surg Sports Traumatol Arthrosc. 2010;18(2):147-151. [40] SCHÖTTLE PB, FUCENTESE SF, ROMERO J. Clinical and radiological outcome of medial patellofemoral ligament reconstruction with a semitendinosus autograft for patella instability. Knee Surg Sports Traumatol Arthrosc. 2005;13(7):516-521. [41] SONG SY, KIM IS, CHANG HG, et al. Anatomic medial patellofemoral ligament reconstruction using patellar suture anchor fixation for recurrent patellar instability. Knee Surg Sports Traumatol Arthrosc. 2014;22(10):2431-2437. [42] WANG HD, DONG JT, GAO SJ. Medial patellofemoral ligament reconstruction using a bone groove and a suture anchor at patellar: a safe and firm fixation technique and 3-year follow-up study. J Orthop Surg Res. 2016;11(1):138. [43] KANG H, CAO J, YU D, et al. Comparison of 2 different techniques for anatomic reconstruction of the medial patellofemoral ligament: a prospective randomized study. Am J Sports Med. 2013;41(5): 1013-1021. [44] SIEBOLD R, CHIKALE S, SARTORY N, et al. Hamstring graft fixation in MPFL reconstruction at the patella using a transosseous suture technique. Knee Surg Sports Traumatol Arthrosc. 2010;18(11): 1542-1544. [45] HEO JW, RO KH, LEE DH. Patellar Redislocation Rates and Clinical Outcomes After Medial Patellofemoral Ligament Reconstruction: Suture Anchor Versus Double Transpatellar Tunnel Fixation. Am J Sports Med. 2019;47(5):1254-1262. [46] DESAI VS, TAGLIERO AJ, PARKES CW, et al. Systematic Review of Medial Patellofemoral Ligament Reconstruction Techniques: Comparison of Patellar Bone Socket and Cortical Surface Fixation Techniques. Arthroscopy. 2019;35(5):1618-1628. [47] HIGUCHI T, ARAI Y, TAKAMIYA H, et al. An analysis of the medial patellofemoral ligament length change pattern using open-MRI. Knee Surg Sports Traumatol Arthrosc. 2010;18(11):1470-1475. [48] SANCHIS-ALFONSO V, RAMIREZ-FUENTES C, MONTESINOS-BERRY E, et al. Femoral insertion site of the graft used to replace the medial patellofemoral ligament influences the ligament dynamic changes during knee flexion and the clinical outcome. Knee Surg Sports Traumatol Arthrosc. 2017;25(8):2433-2441. |
| [1] | Pu Rui, Chen Ziyang, Yuan Lingyan. Characteristics and effects of exosomes from different cell sources in cardioprotection [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(在线): 1-. |
| [2] | Xu Feng, Kang Hui, Wei Tanjun, Xi Jintao. Biomechanical analysis of different fixation methods of pedicle screws for thoracolumbar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1313-1317. |
| [3] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [4] | Du Xiupeng, Yang Zhaohui. Effect of degree of initial deformity of impacted femoral neck fractures under 65 years of age on femoral neck shortening [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1410-1416. |
| [5] | Zhang Shangpu, Ju Xiaodong, Song Hengyi, Dong Zhi, Wang Chen, Sun Guodong. Arthroscopic suture bridge technique with suture anchor in the treatment of acromioclavicular dislocation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1417-1422. |
| [6] | Liang Yan, Zhao Yongfei, Xu Shuai, Zhu Zhenqi, Wang Kaifeng, Liu Haiying, Mao Keya. Imaging evaluation of short-segment fixation and fusion for degenerative lumbar scoliosis assisted by highly selective nerve root block [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1423-1427. |
| [7] | Zhang Chao, Lü Xin. Heterotopic ossification after acetabular fracture fixation: risk factors, prevention and treatment progress [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1434-1439. |
| [8] | Zhou Jihui, Li Xinzhi, Zhou You, Huang Wei, Chen Wenyao. Multiple problems in the selection of implants for patellar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1440-1445. |
| [9] | Wang Debin, Bi Zhenggang. Related problems in anatomy mechanics, injury characteristics, fixed repair and three-dimensional technology application for olecranon fracture-dislocations [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1446-1451. |
| [10] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [11] | Hu Kai, Qiao Xiaohong, Zhang Yonghong, Wang Dong, Qin Sihe. Treatment of displaced intra-articular calcaneal fractures with cannulated screws and plates: a meta-analysis of 15 randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1465-1470. |
| [12] | Shen Jinbo, Zhang Lin. Micro-injury of the Achilles tendon caused by acute exhaustive exercise in rats: ultrastructural changes and mechanism [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1190-1195. |
| [13] | Ji Zhixiang, Lan Changgong. Polymorphism of urate transporter in gout and its correlation with gout treatment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1290-1298. |
| [14] | Yuan Mei, Zhang Xinxin, Guo Yisha, Bi Xia. Diagnostic potential of circulating microRNA in vascular cognitive impairment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1299-1304. |
| [15] | Wang Xianyao, Guan Yalin, Liu Zhongshan. Strategies for improving the therapeutic efficacy of mesenchymal stem cells in the treatment of nonhealing wounds [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1081-1087. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||