Chinese Journal of Tissue Engineering Research ›› 2026, Vol. 30 ›› Issue (35): 9294-9301.doi: 10.12307/2026.469
Previous Articles Next Articles
Efficacy and safety of romozumab in the treatment of osteoporosis in adults: a meta-analysis
Wang Xiaochen1, Guo Lin1, Wang Changcheng2, Xu Tan3, Gu Mingxi3
- 1Department of Orthopedics, Zhongshan Hospital of Dalian University, Dalian 116001, Liaoning Province, China; 2Medical Department of Dalian University of Technology, Dalian 116001, Liaoning Province, China; 3Peking University Shenzhen Hospital, Shenzhen 518000, Guangdong Province, China
-
Received:2025-10-29Revised:2026-02-15Online:2026-12-18Published:2026-04-29 -
Contact:Gu Mingxi, MS, Physician, Peking University Shenzhen Hospital, Shenzhen 518000, Guangdong Province, China -
About author:Wang Xiaochen, Department of Orthopedics, Zhongshan Hospital of Dalian University, Dalian 116001, Liaoning Province, China
CLC Number:
Cite this article
Wang Xiaochen, Guo Lin, Wang Changcheng, Xu Tan, Gu Mingxi. Efficacy and safety of romozumab in the treatment of osteoporosis in adults: a meta-analysis[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(35): 9294-9301.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks

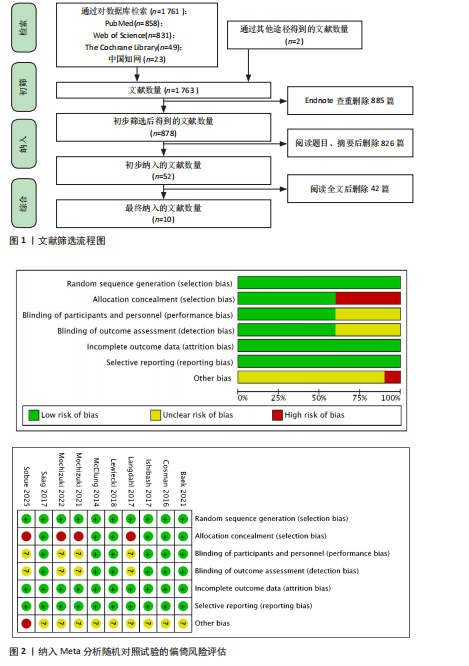
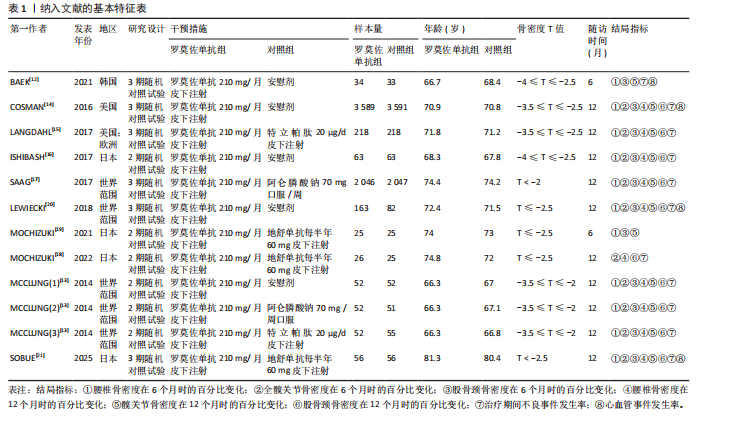
2.1 文献筛选结果 总共从PubMed、Web of Science、Cochrane Library和中国知网数据库中检索了1 763篇文章。将文献导入EndNote X9软件查重排除885篇;根据其标题和摘要将另外826篇文献排除在外,初步纳入52篇文献进行全文评估。详细阅读全文后,42篇文献因不符合选择标准而被删除,最后有10项随机对照试验、共12 570例患者被纳入此项Meta分析[12-21]。图1总结了文献检索和筛选过程,表1列出了10项入选研究的主要特征。 2.2 文献质量评价及偏倚风险评估结果 使用RevMan 5.4软件中的风险和偏倚表对随机对照试验研究进行了文献质量评估。如图2所示,10篇文献均描述了随机序列是如何生成的[12-21],其中6项随机对照试验使用了相同的药物[12-14,16-17,20],并没有影响试验,因此,将它们归类为低风险;4项研究为开放标签研究[15,18-19,21],未进行分配隐藏,存在高选择偏倚风险,而且未描述对结局评估者是否设盲,偏倚风险不明确。所有纳入分析的随机试验均"
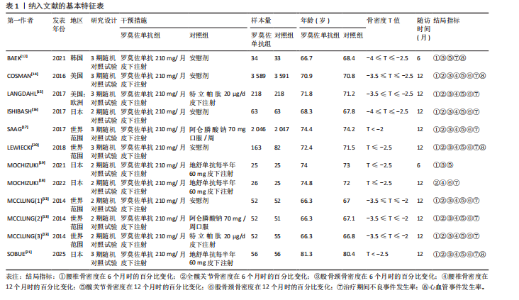
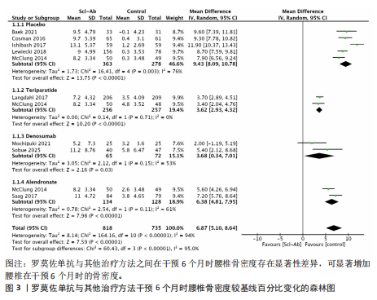
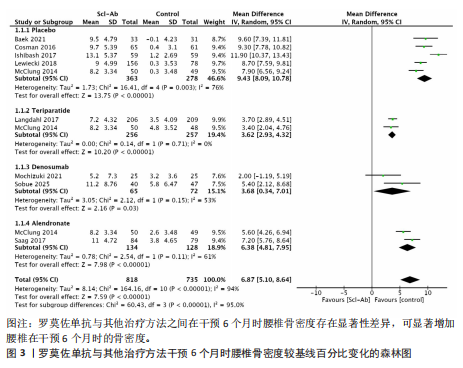
报告了预定措施的结果,没有高风险偏倚,1项研究报告了高风险的其他偏倚来源,即SOBUE团队[21]主要研究人员由于搬迁或退休在试验期间发生了变动。 2.3 主要结果 2.3.1 干预6个月时腰椎骨密度的百分比变化 9项研究报告了干预6个月时腰椎骨密度与基线相比的百分比变化[12-17,19-21],各研究之间的异质性很高(I2=95%)。在亚组分析中,安慰剂亚组的研究存在高度异质性(I2=76%),阿仑膦酸钠亚组和地舒单抗亚组存在中度异质性(I2=61%,53%),特立帕肽亚组存在同质性(I2=0%)。因此采用随机效应模型合并分析数据,Meta分析结果显示在干预6个月时腰椎骨密度在各亚组中差异有显著性意义(MD=6.87,95%CI:5.10-8.64,P < 0.000 01),见图3。罗莫佐单抗可显著增加腰椎在干预6个月时的骨矿物质密度(与安慰剂相比,MD=9.43,95%CI:8.09-10.78,P < 0.000 01;与阿仑膦酸钠相比,MD=6.38,95%CI:4.81-7.95,P < 0.000 01;与特立帕肽相相比,MD=3.62,95%CI:2.93-4.32,P < 0.000 01;与地舒单抗相比,MD=3.68,95%CI:0.34-7.01,P=0.03)。 2.3.2 干预12个月时腰椎骨密度的百分比变化 8项研究报告了12个月时腰椎骨密度与基线相比的百分比变化[13-18,20-21],各研究之间的异质"
"

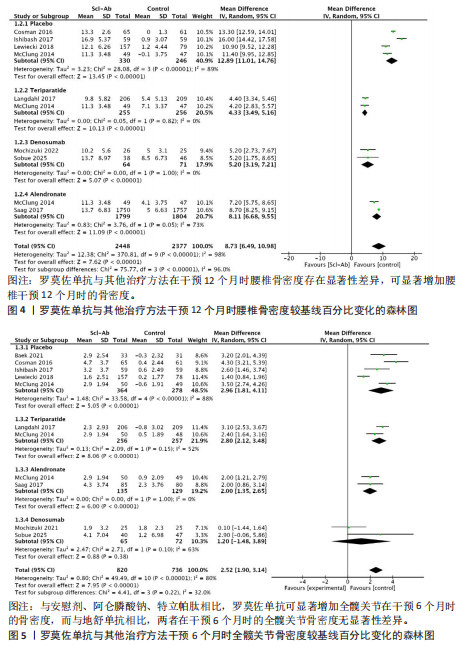
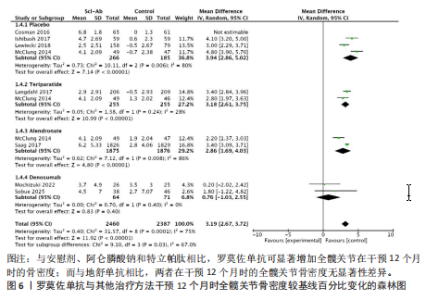
性很高(I2=98%)。在亚组分析中,安慰剂亚组的研究存在高度异质性(I2=89%),阿仑膦酸钠亚组存在中度异质性(I2=73%),特立帕肽亚组和地舒单抗存在同质性(I2=0%)。采用随机效应模型合并分析数据,Meta分析结果显示罗莫佐单抗与其他治疗方法之间在12个月时腰椎骨密度存在显著性差异(MD=8.73,95%CI:6.49-10.98,P < 0.000 01),见图4。罗莫佐单抗可显著增加腰椎在12个月时的骨矿物质密度骨密度(安慰剂MD=12.89,95%CI:11.01-14.76,P < 0.000 01;阿仑膦酸钠MD=8.11,95%CI:6.68-9.55,P < 0.000 01;特立帕肽MD=4.33,95%CI:3.49-5.16,P < 0.000 01;地舒单抗MD=5.20,95%CI:3.19-7.21,P < 0.000 01)。 2.3.3 干预6个月时全髋关节骨密度的百分比变化 9项研究报告了干预6个月时全髋关节骨密度从基线开始的百分比变化[12-17,19-21],各研究之间的异质性很高(I2=80%)。在亚组分析中,安慰剂亚组的研究存在高度异质性(I2=88%),特立帕肽亚组和地舒单抗亚组的研究存在中度异质性(I2=52%,63%),阿仑膦酸钠亚组存在同质性(I2=0%)。采用随机效应模型合并分析数据,Meta分析结果显示罗莫佐单抗与其他治疗方法之间在干预6个月时全髋关节骨密度方面存在显著性差异(MD=2.52,95%CI: 1.90-3.14,P < 0.000 01),见图5。与安慰剂、阿仑膦酸钠、特立帕肽相比,罗莫佐单抗可显著增加全髋关节在6个月时的骨密度(安慰剂MD=2.96,95%CI:1.81-4.11,P < 0.000 01;阿仑膦酸钠MD=2.00,95%CI:1.35-2.65,P < 0.000 01;特立帕肽MD=2.8,95%CI:2.12-3.48,P < 0.000 01);而与地舒单抗相比,两者在干预6个月时的全髋关节骨密度无显著性差异(MD=1.20,95%CI:-1.48-3.89,P=0.38)。 2.3.4 干预12个月时全髋关节骨密度的百分比变化 8项研究报告了干预12个月时全髋关节骨密度从基线开始的百分比变化[13-18,20-21],各研究之间的异质性很高(I2=75%)。在亚组分析中,安慰剂亚组、阿仑膦酸钠亚组的研究存在高度异质性(I2=80%,86%),特立帕肽亚组的研究存在中度异质性(I2 =28%),地舒单抗亚组存在同质性(I2 =0%)。采用随机效应模型合并分析数据,Meta分析结果显示罗莫佐单抗与其他治疗方法之间存在显著性差异(MD=3.19,95%CI:2.67-3.72,P < 0.000 01),见图6。与安慰剂、阿仑膦酸钠和特立帕肽相比,罗莫佐单抗可显著增加全髋关节在干预12个月时的骨密度(安慰剂MD=3.94,95%CI:2.86-5.02,P < 0.000 01;阿仑膦酸钠MD=2.86,95%CI:1.69-4.03,P < 0.000 01;特立帕肽MD=3.18,95%CI:2.61-3.75,P < 0.000 01);而与地舒单"
"
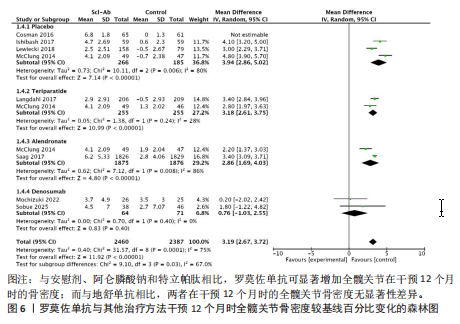

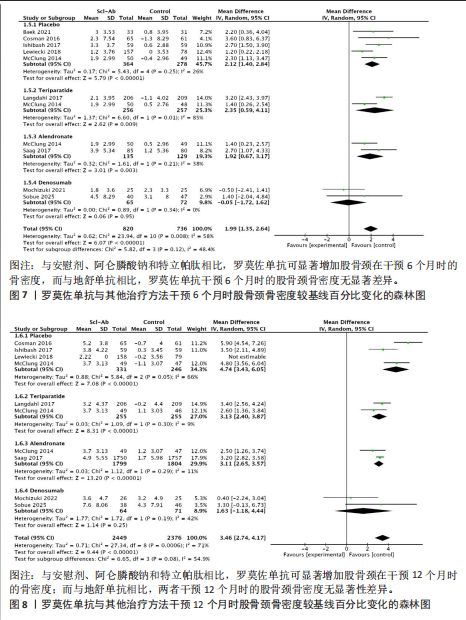
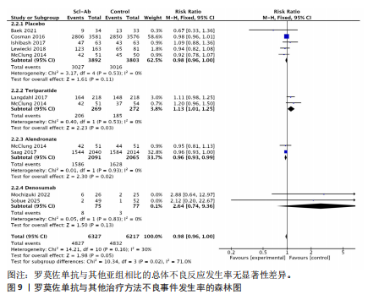
抗相比,两者在干预12个月时的全髋关节骨密度无显著性差异(MD=0.76,95%CI:-1.03-2.55,P=0.4)。 2.3.5 干预6个月时股骨颈骨密度的百分比变化 9项研究报告了干预6个月时股骨颈骨密度从基线开始的百分比变化[12-17,19-21],各研究之间存在中度异质性(I2=58%)。在亚组分析中,地舒单抗亚组存在同质性(I2=0%),安慰剂亚组、阿仑膦酸钠亚组的研究存在中度异质性(I2=26%,I2=38%),特立帕肽亚组的研究存在高度异质性(I2=85%)。采用随机效应模型合并分析数据,Meta分析结果显示罗莫佐单抗与其他治疗方法之间存在显著性差异(MD=1.99,95%CI:1.35-2.64,P < 0.000 01),见图7,与安慰剂、阿仑膦酸钠和特立帕肽相比,罗莫佐单抗可显著增加股骨颈在6个月时的骨密度(安慰剂MD=2.12,95%CI:1.40-2.84,P < 0.000 01;阿仑膦酸钠MD=1.92,95%CI:0.67-3.17,P=0.003;特立帕肽MD=2.35,95%CI:0.59-4.11,P=0.009);而与地舒单抗相比,两者在干预6个月时的股骨颈骨密度无显著性差异(MD=-0.05,95%CI:-1.72-1.62,P=0.95)。 2.3.6 干预12个月时股骨颈骨密度的百分比变化 8项研究报告了干预12个月时股骨颈骨密度从基线开始的百分比变化[13-18,20-21],各研究之间存在中度异质性(I2=71%)。在亚组分析中,安慰剂亚组和地舒单抗亚组存在中度异质性(I2=66%,I2=42%),阿仑膦酸钠亚组和特立帕肽亚组的研究存在同质性(I2=11%,I2=9%)。采用随机效应模型合并分析数据,Meta分析结果显示罗莫佐单抗与其他治疗方法之间存在显著性差异(MD=3.46,95%CI:2.74-4.17,P < 0.000 01),见图8。与安慰剂、阿仑膦酸钠和特立帕肽相比,罗莫佐单抗可显著增加股骨颈在干预12个月时的骨密度(安慰剂MD=4.74,95%CI:3.43-6.05,P < 0.000 01;阿仑膦酸钠MD=3.11,95%CI:2.65-3.57,P < 0.000 01;特立帕肽MD=3.13,95%CI:2.40-3.87,P < 0.000 01);而与地舒单抗相比,两者在干预12个月时的股骨颈骨密度无显著性差异(MD=1.63,95%CI:-1.18-4.44,P=0.25)。 2.4 次要结果 2.4.1 不良事件发生率 有9项纳入研究记录了“任何不良事件”这一结果[12-18,20-21],1项研究只记录了严重不良事件[21],亚组分析显示安慰剂、阿仑膦酸钠和特立帕肽、地舒单抗亚组研究之间异质性较低(均为I2=0%),因此采用了固定效应模型合并数据。结果表明,罗莫佐单抗与其他药物的总体不良反应发生率无显著性差异(RR=0.98,95%CI:0.96-1,P=0.05),见图9。然而亚组分析显示,与阿仑膦酸钠组相比,罗莫佐单抗的不良事件发生率较低(RR=0.96,95%CI:0.93-0.99,P=0.02);与特立帕肽组相比,罗莫佐单抗的不良事件发生率较高(RR=1.13,95%CI:1.01-1.25,P=0.03)。而罗莫佐单抗与安慰剂、地诺单抗在不良事件发生率上无显著性差异(RR=0.98,95%CI:0.96-1.00,P=0.11;RR=2.64,95%CI:0.74-9.36,P=0.13)。 2.4.2 心血管事件发生率 有4项纳入研究记录了“心血管事件”这一并发症发生情"
"
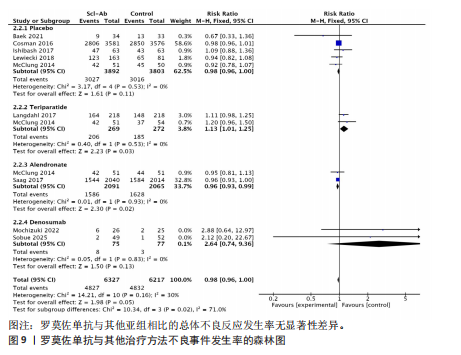
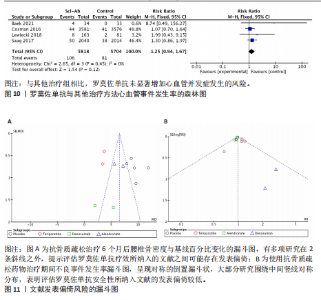
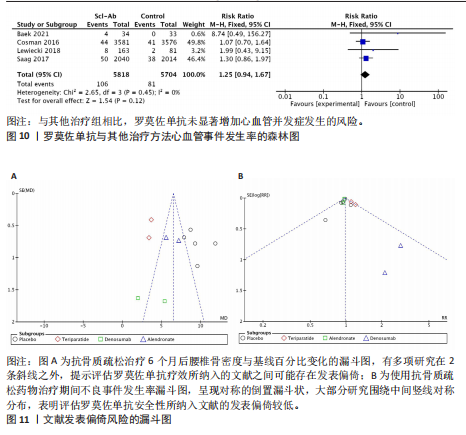
况[12,14,20-21]。罗莫佐单抗与安慰剂、阿仑膦酸钠和特立帕肽、地舒单抗的各研究之间存在同质性(I2=0%),因此采用了固定效应模型合并数据。Meta分析表明,与其他研究组相比,罗莫佐单抗未显著增加心血管并发症发生的风险(RR=1.25,95%CI:0.94-1.67,P=0.12),见图10。 2.5 发表偏倚和敏感性分析 为了评估主要目的报告指标的发表偏倚,对抗骨质疏松治疗6个月后腰椎骨密度与基线百分比变化的漏斗图进行分析。虽然各个研究应该平均分布于竖线两侧,但有多项研究在2条斜线之外,提示评估罗莫佐单抗疗效所纳入的文献之间可能存在发表偏倚,见图11A。为了评估次要目的报告指标的发表偏倚,对抗骨质疏松药物治疗期间不良事件发生率漏斗图进行分析。漏斗图呈现对称的倒置漏斗状,大部分研究围绕中间竖线对称分布,且点都落在95%可信区间内,表明评估罗莫佐单抗安全性所纳入文献的发表偏倚比较低,见图11B。总的来说,由于此次Meta分析纳入的研究只有10篇,漏斗图的对称性可能不准确,难以准确判断发表偏倚,因此通过敏感性分析将每项研究单独剔除,评估汇总结果的异质性和稳健性。敏感性分析结果表明此项Meta分析的结果是稳定的。"
| [1] HUANG W, NAGAO M, YONEMOTO N, et al. Evaluation of the efficacy and safety of romosozumab (evenity) for the treatment of osteoporotic vertebral compression fracture in postmenopausal women: A systematic review and meta-analysis of randomized controlled trials (CDM-J). Pharmacoepidemiol Drug Saf. 2023; 32(6):671-684. [2] HERNANDEZ AV, PÉREZ-LÓPEZ FR, PISCOYA A, et al. Comparative efficacy of bone anabolic therapies in women with postmenopausal osteoporosis: A systematic review and network meta-analysis of randomized controlled trials. Maturitas. 2019; 129:12-22. [3] HÄNDEL MN, CARDOSO I, VON BÜLOW C, et al. Fracture risk reduction and safety by osteoporosis treatment compared with placebo or active comparator in postmenopausal women: systematic review, network meta-analysis, and meta-regression analysis of randomised clinical trials. BMJ. 2023;381:e068033. [4] LEWIECKI EM, BETAH D, HUMBERT L, et al. 3D-modeling from hip DXA shows improved bone structure with romosozumab followed by denosumab or alendronate. J Bone Miner Res. 2024;39(4):473-483. [5] ZHIVODERNIKOV IV, KIRICHENKO TV, MARKINA YV, et al. Molecular and Cellular Mechanisms of Osteoporosis. Int J Mol Sci. 2023;24(21):15772. [6] KOBAYAKAWA T, MIYAZAKI A, TAKAHASHI J, et al. Verification of efficacy and safety of ibandronate or denosumab for postmenopausal osteoporosis after 12-month treatment with romosozumab as sequential therapy: The prospective VICTOR study. Bone. 2022;162:116480. [7] POUTOGLIDOU F, SAMOLADAS E, RAIKOS N, et al. Efficacy and safety of anti-sclerostin antibodies in the treatment of osteoporosis: A meta-analysis and systematic review. J Clin Densitom. 2022; 25(3):401-415. [8] LEWIECKI EM, BLICHARSKI T, GOEMAERE S, et al. A Phase III Randomized Placebo-Controlled Trial to Evaluate Efficacy and Safety of Romosozumab in Men With Osteoporosis. J Clin Endocrinol Metab. 2018;103(9):3183-3193. [9] LAU EMC, DINAVAHI R, WOO YC, et al. Romosozumab or alendronate for fracture prevention in East Asian patients: a subanalysis of the phase III, randomized ARCH study. Osteoporos Int. 2020;31(4):677-685. [10] MCCOLM J, HU L, WOMACK T, et al. Single- and multiple-dose randomized studies of blosozumab, a monoclonal antibody against sclerostin, in healthy postmenopausal women. J Bone Miner Res. 2014;29:935-43. [11] MOHER D, LIBERATI A, TETZLAFF J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010; 8:336-341. [12] BAEK KH, CHUNG YS, KOH JM, et al. Romosozumab in Postmenopausal Korean Women with Osteoporosis: A Randomized, Double-Blind, Placebo-Controlled Efficacy and Safety Study. Endocrinol Metab (Seoul). 2021;36(1):60-69. [13] MCCLUNG MR, GRAUER A, BOONEN S, et al. Romosozumab in postmenopausal women with low bone mineral density. N Engl J Med. 2014;370(5):412-420. [14] COSMAN F, CRITTENDEN DB, ADACHI JD, et al. Romosozumab Treatment in Postmenopausal Women with Osteoporosis. N Engl J Med. 2016; 375(16):1532-1543. [15] LANGDAHL BL, LIBANATI C, CRITTENDEN DB, et al. Romosozumab (sclerostin monoclonal antibody) versus teriparatide in postmenopausal women with osteoporosis transitioning from oral bisphosphonate therapy: a randomised, open-label, phase 3 trial. Lancet. 2017;390(10102): 1585-1594. [16] ISHIBASHI H, CRITTENDEN DB, MIYAUCHI A, et al. Romosozumab increases bone mineral density in postmenopausal Japanese women with osteoporosis: A phase 2 study. Bone. 2017; 103:209-215. [17] SAAG KG, PETERSEN J, BRANDI ML, et al. Romosozumab or Alendronate for Fracture Prevention in Women with Osteoporosis. N Engl J Med. 2017;377(15):1417-1427. [18] MOCHIZUKI T, YANO K, IKARI K, et al. Comparison of romosozumab versus denosumab treatment on bone mineral density after 1 year in rheumatoid arthritis patients with severe osteoporosis: A randomized clinical pilot study. Mod Rheumatol. 2023;33(3):490-495. [19] MOCHIZUKI T, YANO K, IKARI K, et al. Effects of romosozumab or denosumab treatment on the bone mineral density and disease activity for 6 months in patients with rheumatoid arthritis with severe osteoporosis: An open-label, randomized, pilot study. Osteoporos Sarcopenia. 2021;7(3): 110-114. [20] LEWIECKI EM, BLICHARSKI T, GOEMAERE S, et al. A Phase III Randomized Placebo-Controlled Trial to Evaluate Efficacy and Safety of Romosozumab in Men With Osteoporosis. J Clin Endocrinol Metab. 2018;103(9):3183-3193. [21] SOBUE Y, KOSUGIYAMA H, ASAI S, et al. A randomized controlled trial comparing romosozumab and denosumab in elderly women with primary osteoporosis and knee osteoarthritis. Sci Rep. 2025;15(1):22441. [22] RECKNOR CP, RECKER RR, BENSON CT, et al. The Effect of Discontinuing Treatment With Blosozumab: Follow-up Results of a Phase 2 Randomized Clinical Trial in Postmenopausal Women With Low Bone Mineral Density. J Bone Miner Res. 2015;30:1717-1725. [23] WEN F, DU H, DING L, et al. Clinical efficacy and safety of drug interventions for primary and secondary prevention of osteoporotic fractures in postmenopausal women: Network meta-analysis followed by factor and cluster analysis. PLoS One. 2020;15(6):e0234123. [24] BHANDARI M, SCHEMITSCH EH, KARACHALIOS T, et al. Romosozumab in Skeletally Mature Adults with a Fresh Unilateral Tibial Diaphyseal Fracture: A Randomized Phase-2 Study. J Bone Joint Surg Am. 2020;102(16):1416-1426. [25] SCHEMITSCH EH, MICLAU T, KARACHALIOS T, et al. A Randomized, Placebo-Controlled Study of Romosozumab for the Treatment of Hip Fractures. J Bone Joint Surg Am. 2020;102(8):693-702. [26] PADHI D, ALLISON M, KIVITZ AJ, et al. Multiple doses of sclerostin antibody romosozumab in healthy men and postmenopausal women with low bone mass: a randomized, double-blind, placebo-controlled study. J Clin Pharmacol. 2014; 54(2):168-178. [27] TAKADA J, DINAVAHI R, MIYAUCHI A, et al. Relationship between P1NP, a biochemical marker of bone turnover, and bone mineral density in patients transitioned from alendronate to romosozumab or teriparatide: a post hoc analysis of the STRUCTURE trial. J Bone Miner Metab. 2020;38(3):310-315. [28] HU M, ZHANG Y, GUO J, et al. Meta-analysis of the effects of denosumab and romosozumab on bone mineral density and turnover markers in patients with osteoporosis. Front Endocrinol (Lausanne). 2023;14:1188969. [29] KEAVENY TM, CRITTENDEN DB, BOLOGNESE MA, et al. Greater Gains in Spine and Hip Strength for Romosozumab Compared With Teriparatide in Postmenopausal Women With Low Bone Mass. J Bone Miner Res. 2017;32(9):1956-1962. [30] GENANT HK, ENGELKE K, BOLOGNESE MA, et al. Effects of Romosozumab Compared With Teriparatide on Bone Density and Mass at the Spine and Hip in Postmenopausal Women With Low Bone Mass. J Bone Miner Res. 2017; 32(1):181-187. [31] CHENG SH, CHU W, CHOU WH, et al. Cardiovascular Safety of Romosozumab Compared to Commonly Used Anti-osteoporosis Medications in Postmenopausal Osteoporosis: A Systematic Review and Network Meta-analysis of Randomized Controlled Trials. Drug Saf. 2025;48(1):7-23. [32] GOLLEDGE J, THANIGAIMANI S. Role of Sclerostin in Cardiovascular Disease. Arterioscler Thromb Vasc Biol. 2022;42(7):e187-e202. [33] BOVIJN J, KREBS K, CHEN CY, et al. Evaluating the cardiovascular safety of sclerostin inhibition using evidence from meta-analysis of clinical trials and human genetics. Sci Transl Med. 2020; 12(549):eaay6570. [34] MIGLIORINI F, COLAROSSI G, BARONCINI A, et al. Pharmacological Management of Postmenopausal Osteoporosis: a Level I Evidence Based-Expert Opinion. Expert Rev Clin Pharmacol. 2021;14(1): 105-119. [35] ALTMAN DG, BLAND JM. Absence of evidence is not evidence of absence. BMJ. 1995; 311(7003):485. [36] SINGH S, DUTTA S, KHASBAGE S, et al. A systematic review and meta-analysis of efficacy and safety of Romosozumab in postmenopausal osteoporosis. Osteoporos Int. 2022;33(1):1-12. |
| [1] | Chen Huiting, Zeng Weiquan, Zhou Jianhong, Wang Jie, Zhuang Congying, Chen Peiyou, Liang Zeqian, Deng Weiming. Tail anchoring technique of vertebroplasty in treatment of osteoporotic vertebral compression fractures with intravertebral cleft: a finite element analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2145-2152. |
| [2] | Zeng Xuan, Weng Rui, Ye Shicheng, Tang Jiadong, Mo Ling, Li Wenchao. Two lumbar rotary manipulation techniques in treating lumbar disc herniation: a finite element analysis of biomechanical differences [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2153-2161. |
| [3] | Cheng Qisheng, Julaiti·Maitirouzi, Xiao Yang, Zhang Chenwei, Paerhati·Rexiti. Finite element analysis of novel variable-diameter screws in modified cortical bone trajectory of lumbar vertebrae [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2162-2171. |
| [4] | Liu Wenlong, Dong Lei, Xiao Zhengzheng, Nie Yu. Finite element analysis of tibial prosthesis loosening after fixed-bearing unicompartmental knee arthroplasty for osteoporosis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2191-2198. |
| [5] | Chen Long, Wang Xiaozhen, Xi Jintao, Lu Qilin. Biomechanical performance of short-segment screw fixation combined with expandable polyetheretherketone vertebral body replacement in osteoporotic vertebrae [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2226-2235. |
| [6] | Hu Xiongke, Liu Shaohua, Tan Qian, Liu Kun, Zhu Guanghui. Shikonin intervention with bone marrow mesenchymal stem cells improves microstructure of femur in aged mice [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(7): 1609-1615. |
| [7] | Wu Zhilin, , He Qin, Wang Pingxi, Shi Xian, Yuan Song, Zhang Jun, Wang Hao . DYRK2: a novel therapeutic target for rheumatoid arthritis combined with osteoporosis based on East Asian and European populations [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(6): 1569-1579. |
| [8] | Zhang Haiwen, Zhang Xian, Xu Taichuan, Li Chao. Bibliometric and visual analysis of the research status and trends of senescence in osteoporosis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(6): 1580-1591. |
| [9] | Wen Guangwei, Zhen Yinghao, Zheng Taikeng, Zhou Shuyi, Mo Guoye, Zhou Tengpeng, Li Haishan, Lai Yiyi. Effects and mechanisms of isoginkgetin on osteoclastogenesis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(6): 1348-1358. |
| [10] | Huang Jie, Zeng Hao, Wang Wenchi, Lyu Zhucheng, Cui Wei. Visualization analysis of literature on the effect of lipid metabolism on osteoporosis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(6): 1558-1568. |
| [11] | Chen Qiang, Wu Wenjuan, Jiang Shuhua, Huang Da. Physical exercise improves physical function in burn patients: a systematic review and meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(5): 1269-1281. |
| [12] | Yang Zhijie, Zhao Rui, Yang Haolin, Li Xiaoyun, Li Yangbo, Huang Jiachun, Lin Yanping, Wan Lei, HuangHongxing. Postmenopausal osteoporosis: predictive values of muscle mass, grip strength, and appendicular skeletal muscle index [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(5): 1073-1080. |
| [13] | Zhou Jian, Zhang Tao, Zhou Weili, Zhao Xingcheng, Wang Jun, Shen Jie, Qian Li, Lu Ming. Effects of resistance training on quadriceps mass and knee joint function in patients with osteoporosis and sarcopenia [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(5): 1081-1088. |
| [14] | Cao Wenqi, Feng Xiuzhi, Zhao Yi, Wang Zhimin, Chen Yiran, Yang Xiao, Ren Yanling. Effect of macrophage polarization on osteogenesis-angiogenesis coupling in type 2 diabetic osteoporosis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(4): 917-925. |
| [15] | Jiang Yang, Peng Hao, Song Yanping, Yao Na, Song Yueyu, Yin Xingxiao, Li Yanqi, Chen Qigang. Isometric exercise reduces resting blood pressure: a meta-analysis of moderating factors and dose effects [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(4): 975-986. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||