Chinese Journal of Tissue Engineering Research ›› 2024, Vol. 28 ›› Issue (17): 2753-2758.doi: 10.12307/2024.478
Previous Articles Next Articles
Effect of graft type on knee function after anterior cruciate ligament reconstruction
Li Luyi1, Li Xiaojie2, Hei Zeming1, Liu Hua1
- 1Capital University of Physical Education And Sports, Beijing 100191, China; 2Department of Orthopedics, Air Force Medical Center, Beijing 100142, China
-
Received:2023-07-25Accepted:2023-09-12Online:2024-06-18Published:2023-12-16 -
Contact:Liu Hua, Associate professor, Capital University of Physical Education And Sports, Beijing 100191, China -
About author:Li Luyi, Master, Capital University of Physical Education And Sports, Beijing 100191, China -
Supported by:Quality Undergraduate Program in Beijing Universities, No. 145122005/004 (to LH); Beijing Higher Education “Undergraduate Teaching Reform and Innovation Project”, No. 145122002/007 (to LH); 2023 Connotation Development-Scientific Research-Science and Technology Strengthening Support Program, No. 155223021 (to LH)
CLC Number:
Cite this article
Li Luyi, Li Xiaojie, Hei Zeming, Liu Hua. Effect of graft type on knee function after anterior cruciate ligament reconstruction[J]. Chinese Journal of Tissue Engineering Research, 2024, 28(17): 2753-2758.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
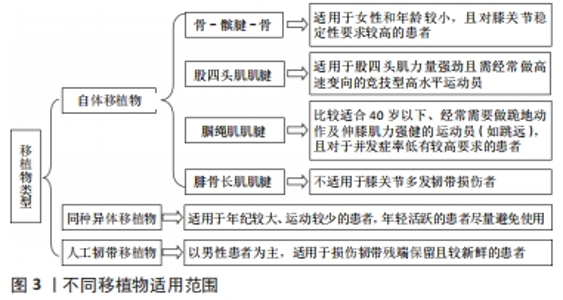
2.1 移植物类型 不同移植物适用范围见图3。"


2.1.1 自体肌腱移植物 自体移植物是进行前交叉韧带重建最早使用的移植物,具有较强的韧性,能更好地满足膝关节屈伸旋转时所要求的韧带张力,经过2年随访发现其具有较低的再断率[13],且免疫排斥反应与传播感染性疾病的可能性较低,成为前交叉韧带重建术的首选[9],这种移植物重建后并发症较少,利于患者更快地恢复至术前运动水平[14]。 骨-髌腱-骨:是取自髌腱中央1/3处两端保留了天然肌腱-骨移植物,保留的骨质通过螺钉挤压能够在隧道内形成较为可靠的愈合界面,使其更好地融合在股骨和胫骨中[15],增加了重建韧带附着点的稳定性,且移植失败率低、手术满意度高[16],因此最早作为前交叉韧带重建的“金标准”移植物类型。但也有研究表明,选用骨-髌腱-骨移植物的患者术后常常出现合并髌骨软化、髌骨骨折、髌前疼痛、屈曲挛缩等并发症,所以此类患者进行膝关节开链运动的时间均较选用其他移植物的患者延后,不利于肌肉力量的发展,这可能与移植物获取破坏了伸膝复合体有关[17]。因此对于既往存在髌股关节疾病、伸膝装置对线不良及髌腱较窄的患者,应尽量避免使用骨-髌腱-骨作为移植物[18]。 腘绳肌肌腱:腘绳肌肌腱自体移植物主要取自股薄肌和半腱肌肌腱。与骨-髌腱-骨移植物相比,腘绳肌肌腱提供的纤维间质多20%-30%、成纤维细胞多35%-50%,在实验室中被证明是所有移植物中韧性最强的[8],能够达到正常前交叉韧带力学强度的1.5倍[19],因此常被应用于重建后。此外,腘绳肌肌腱移植物可以减少髌股关节摩擦、膝前疼痛及伸直受限的发生率[20],这种移植物更适合40岁以下人群:运动爱好者[15],经常需要做跪地动作的人(如信教徒跪地祈祷等),要求伸膝肌力强健的运动员(如跳远),以及担心再次出现髌股关节不适的患者等[11]。但腘绳肌肌腱自体移植存在较高的移植失败率,同时容易引起腘绳肌无力和关节松弛[21]。 股四头肌肌腱:由3层组成,最深层为股中间肌,中间层则包括股内侧肌和股外侧肌,而最外层为股直肌肌腱[22]。组织学上,股四头肌肌腱厚度是骨-髌腱-骨的1.8倍,横截面积是相同厚度骨-髌腱-骨的2倍,最大有效载荷可达2 185-2352 N[8],这种组织结构使得股四头肌肌腱具有较强的力学强度和抗张能力,与天然前交叉韧带更为相似。因此,股四头肌肌腱移植物更适用于股四头肌力量强劲且需经常做高速变向的高竞技性水平运动员,如篮球、足球等[9]。相对于骨-髌腱-骨移植物,采用股四头肌肌腱移植物的患者出现膝前痛的比例较小、发生髌骨骨折的风险较低,但由于取腱位置血供较为丰富,出血和感染风险增加[9],同时不利于股四头肌肌力的恢复[7]。 腓骨长肌肌腱:位于外踝后上方,向下近垂直走行,经过外踝后沟在踝下转向前下走行,经骰骨跖面的腓骨长肌腱沟向前内方走行,最终止于内侧楔骨足底外侧面及第 1、2跖骨基底部。因此,在外踝尖上2 cm 的外踝后沟容易触及肌腱,且此处无重要血管神经,暴露更加方便,取腱更加快捷[23]。因取材方便、生物力学性能良好、供区并发症少、组织相容性优异及具有良好的临床效果等特点,腓骨长肌肌腱目前逐渐应用于临床前交叉韧带重建中。生物力学研究表明,腓骨长肌肌腱在解剖学和生物力学上具有足够的长度和弹性,其极限拉伸强度较原生前交叉韧带更强,且带有腱膜,具有良好的血液供应[24]。此外,使用自体腓骨长肌肌腱移植可有效避免对膝关节周围韧带造成二次损伤,尤其对于创伤所致的前交叉韧带损伤伴内外侧副韧带损伤患者,可进一步减少对残存膝关节稳定结构的破坏,提高其稳定性[25]。但腓骨长肌肌腱移植物不适用于膝关节多发韧带损伤者[26]。 2.1.2 同种异体移植物移植 对比自体移植物,同种异体移植物在手术过程中不会对机体造成额外的创伤,同时避免了取材部位并发症,在自体肌腱取材受限时存在更多选择性,例如髌韧带、跟腱、腘绳肌肌腱、胫骨前肌肌腱、胫骨后肌肌腱、腓骨长肌肌腱等均可为供区取材,其中以髌韧带、跟腱的应用最常见[19]。同种异体移植物在前交叉韧带手术中的使用比过去更普遍,但有证据表明,同种异体移植物出现再次断裂的风险高于自体移植物,同时组织学研究显示,同种异体移植物细胞增生和血管化的过程较长,愈合较缓慢,不适用于青少年和运动量较大的患者[27]。除此之外,同种异体移植物的使用还受到医疗成本和疾病传播的影响[28]。 2.1.3 人工韧带物移植 目前,人工韧带移植物主要分为永久型、支架型和加强型三类[29]。LARS人工韧带是近年来使用和研究的热点,它采用高韧性的聚酯纤维制成,抗疲劳强度高,并且最大载荷会随着韧带纤维数量的不同而变化,其中30-100根人工韧带纤维最大载荷为1 500-4 700 N,抗疲劳和抗重复弯曲扭转效果理想,可满足日常活动和高强度运动所需的韧带强度[30],而且力学性能良好,植入后即刻就可以得到足够的抗拉强度与关节稳定性,使患者能够早期适应较大强度的康复训练,更快地恢复至术前功能水平[31]。随着人工韧带材料的进展,其最大载荷也在不断提高,甚至能达到正常前交叉韧带载荷的273%[32]。因此,选用人工韧带的患者术后恢复快,可进行早期功能性活动,具有足够的膝关节稳定性,同时不损伤自体组织,避免了疾病传播及免疫排斥等并发症,受到了部分患者的欢迎,但因其价格昂贵、组织兼容性差可能引起医源性关节病,这些成为运动爱好患者的顾虑[33]。 2.2 不同移植物对前交叉韧带重建后患者下肢肌肉力量的影响 由于前交叉韧带断裂后关节源性肌肉抑制的出现,导致股四头肌萎缩、力量下降及恢复减缓等问题[34],而上述的下肢神经肌肉控制缺陷则被认为是继发性(再撕裂)前交叉韧带损伤的危险因素,经常用于评估重返运动的准备情况,特别是股四头肌的力量,与前交叉韧带重建后腿部的功能有关。 由于骨-髌腱-骨和股四头肌肌腱移植物取腱均对膝关节伸膝复合体存在创伤,因此,选用骨-髌腱-骨和股四头肌肌腱两种移植物的患者存在显著的股四头肌萎缩、力量下降、恢复速度变慢等问题[8]。选用骨-髌腱-骨移植物的患者股内侧肌、股外侧肌、股中间肌横截面积均小于选用其他移植物的患者,且以股内侧肌萎缩最为严重[35]。 研究显示,术后不同角速度和多个时间点的等速膝关节伸展力量缺陷明显较屈曲更大[36],例如前交叉韧带重建后6个月,等速膝关节屈曲力量的平均对称性指数值在80%-90%,1年后恢复可接近正常值。这种趋势并没有在等速膝关节伸展的结果中观察到,选用骨-髌腱-骨移植物的患者无论是低速或是高速测试其股四头肌肌力均低于选用其他移植物患者[37],且角速度越大表现的肌力不足越明显[38],因此,选用骨-髌腱-骨移植物的患者股四头肌肌力大约需要2年时间才能恢复到术前水平[39]。股四头肌肌腱移植6个月时对称性指数值通常在70%左右,1年后仍在90%以下,甚至股四头肌肌腱移植物患者3-7年的长期随访仍然存在伸膝无力[8]。由此可见,选用自体移植物的患者股四头肌肌力恢复需要较长时间才能达到伤前水平[39]。选用骨-髌腱-骨自体移植物与腘绳肌肌腱移植物患者术后任何时间点或者角度的等速伸展力量均无显著差异。同种异体移植物和人工韧带重建均未对患者机体造成额外的创伤,更有利于发展膝关节周围肌肉力量。研究发现,选用同种异体移植物患者术后6个月等速60°股四头肌峰值力矩高于选用自体移植物患者[40];1-5年的随访发现,早期选择人工韧带移植物能够更快地恢复股四头肌力量[41]。 选用腘绳肌肌腱移植物患者术后常出现明显的腘绳肌肌力下降,甚至重建术后18个月患侧峰值力矩仍然较健侧差,且随着屈膝角度的增大,腘绳肌无力现象越明显,尤其以屈膝70°-90°最为明显[42]。等速测试结果显示,选用自体腘绳肌肌腱移植物的患者患侧与健侧峰力矩比值在术后4个月下降,6个月后才逐渐增加,直至1年后才能恢复至伤前水平[39]。前交叉韧带重建后1年,腘绳肌肌腱移植物组患者等速60°和180°膝关节屈曲对称性指数明显低于骨-髌腱-骨自体移植物组。因此,选用腘绳肌肌腱移植物的患者尤其需要重视加强腘绳肌的力量训练[43]。 与自体腘绳肌腱移植物组相比,自体腓骨长肌肌腱移植物组患者术后1年的大腿周径下降值明显减小、大腿肌肉萎缩情况较少,具有良好的下肢肌力,这与移植物取腱位置密不可分,由于腓骨长肌肌腱取腱位置远离膝关节避免了对膝关节的二次创伤,减少了隐神经损伤、大腿内侧疼痛等供区并发症的发生,同时可尽早对膝关节周围肌肉进行力量训练,更好地维持下肢力量,且术后 1 年时踝关节功能并未见明显受累,推测其原因可能是腓骨短肌功能得到了完整保留[24]。 2.3 移植物类型对前交叉韧带重建后患者膝关节稳定性的影响 术后膝关节稳定性是评估患者恢复情况的重要指标之一,膝关节稳定性的评价包括静态和动态两方面。静态稳定性测试主要采用膝关节稳定性测试仪,对比评价放松状态下左右膝韧带和关节囊的松弛程度。一般女性的膝前关节松弛程度比男性更严重,更容易发生下肢损伤[44]。KT1000和KT2000主要用于评价膝关节韧带处于放松状态下的松弛度。研究表明,前交叉韧带重建后常采用KT1000对比患者双侧膝关节松弛度,大于6 mm认为韧带可能出现松弛,需要再次重建[45]。动态稳定性可通过脊髓水平、大脑活动和认知程序3种层次的神经肌肉反馈形式来反映。对于大脑活动水平神经反馈的重建主要通过膝关节挤压、不同屈膝角度的重心转移、反复的平衡训练等激活前交叉韧带及其周围组织器官的机械感受器,将关节位置、负荷、运动速度变化等信息传入神经中枢,并由神经中枢将这些信息与视觉、前庭传入的冲动进行不断调节、整合,以此调节肌肉兴奋,保持身体姿势及动态平衡[46]。 研究表明,采用不同自体移植物其后期静态稳定性存在差异。术后1年与健侧腿相比,采用自体骨-髌腱-骨移植物重建后的膝关节静态稳定性更高、松弛程度更小。术后1年与健侧腿相比,采用骨-髌腱-骨移植物患膝的松弛度仅为 1.3 mm,而腘绳肌肌腱移植物则为2.4 mm;术后2年,采用骨-髌腱-骨移植物与腘绳肌肌腱移植物患膝的松弛度分别为 1.5 mm和 2.5 mm[37]。通过2 年的随访也发现,相较于采用骨-髌腱-骨移植物患者,采用腘绳肌肌腱移植物患者更易出现膝前部松弛[47],这可能与移植物特性有关,髌腱移植物相较于肌腱移植物更为坚硬[48],同时也与腘绳肌肌腱和骨隧道融合速度较慢、耗费时间较长密不可分[49]。采用股四头肌肌腱和腘绳肌肌腱移植物患者膝关节静态稳定性无明显差异,这可能与膝关节伸肌肌力恢复导致的移植物所受生物力学应力有关[50]。采用腓骨长肌肌腱移植物患者术后具有较高的膝关节稳定性,术后6,12,18个月的随访发现膝关节KT2000松弛度均维持在2 mm以内[51],这与腓骨长肌肌腱移植物的物理特性密切相关,研究发现腓骨长肌肌腱极限张力负荷可达4 268 N,与4股的腘绳肌在最大拉力上相差无异,是自体前交叉韧带的2倍,且其最大负荷是半腱肌的0.97倍、股薄肌的1.4倍,具有较强的韧性,因此其膝关节稳定性较高[52]。 同种异体移植物由于需要辐射消毒导致韧带抗张力能力下降、愈合时间延长,韧带松弛问题高发[53]。Lachman和轴移试验测试结果均显示,相比自体移植物组,同种异体移植物组膝关节前后及旋转松弛更明显[54],且经过γ射线处理之后患者膝关节松弛愈发显著[55],术后6个月时膝关节松弛度增量最大[56],术后31个月时重建失败率高达34.4%[57]。使用人工韧带重建前交叉韧带则不需要考虑韧带松弛变化,能够尽早的进行肌肉力量训练[58]。一项针对人工韧带重建前交叉韧带的研究发现,术前韧带松弛度约为5.1 mm,经过7年的随访患者术后韧带松弛度约为1.4 mm,恢复了较高的膝关节稳定性,预后良好[59]。但TIEFENBOECK等[60]认为人工韧带的手术失败率较高,从X射线片观察看存在早期关节炎的表现。虽然移植人工韧带能够尽早地恢复患者运动,但从长远角度来讲不建议使用人工韧带。 膝关节的动态稳定性与屈伸肌肌肉力量密切有关。MAGALH?ES等[61]指出腘绳肌与股四头肌肌力比值在不同测试速度下的变化范围为50%-70%,一般认为在等速测试 60°角速度下,腘绳肌与股四头肌肌力正常比值为 60%左右。选用股四头肌肌腱和骨-髌腱-骨移植物的患者均表现出较高的腘绳肌与股四头肌肌力比,比值增高的原因可能与股四头肌肌力下降相关,由于取腱对伸膝复合体存在损伤,进一步导致伸膝力量降低,1年的随访发现选用这两种移植物患者的伸膝力量仅恢复至术前的87%[36]。选用腘绳肌肌腱移植物患者表现出较差的膝关节动态稳定性,这是由于腘绳肌肌腱移植物取材导致肌肉力量恢复较慢,1年的随访发现,骨-髌腱-骨移植物组患者腘绳肌肌力恢复至术前的99%,而腘绳肌肌腱移植物组患者腘绳肌肌力仅恢复至术前的91%,因而表现出动态稳定性降低[36],二次损伤的可能性更高[62]。 2.4 移植物类型对前交叉韧带重建后患者功能性活动的影响 前交叉韧带重建后功能性活动主要用来评估患者术后膝关节运动恢复情况,测试包括平衡功能、本体感觉、功能性跳跃以及各项功能自评量表。主观自评量表主要包括IKDC[63]、Lysholm膝关节评分、膝关节损伤与骨关节炎评分[64]、Tegner活动水平量表和辛辛那提膝关节量表[65-66],这些量表常用来评估前交叉韧带重建后患者膝关节功能恢复情况,其中IKDC还能预测膝关节功能恢复效果[67]。功能性跳跃测试中主要评估健患侧单腿跳[68]、单腿三级跳、单腿交叉跳和6 m计时跳,通过肢体对称指数来反映健患腿之间功能的对称性,以显示患者康复情况以及作为重返运动的标准[69]。其中,单腿跳还能用来评估神经肌肉控制和运动的信心[70]。 采用自体股四头肌肌腱移植物患者的IKDC评分高于选用其他自体移植物患者[71]。采用腓骨长肌肌腱移植物患者的IKDC评分和Lysholm评分均高于采用腘绳肌肌腱移植物患者,这可能与腘绳肌肌腱移植物取腱后鹅足区疼痛影响了患者早期膝关节功能训练,进而影响大腿肌力,使得膝关节稳定性下降,且部分患者出现了隐神经髌下支损伤导致的感觉减退或麻木,从而影响了患者的主观满意度有关[72]。采用骨-髌腱-骨移植物患者术后12周的KOOS评分和IKDC评分均显著低于采用腘绳肌肌腱移植物患者,其中采用腘绳肌肌腱移植物患者KOOS评分改善了24.2分,而采用骨-髌腱-骨移植物患者只改善了15.3分[73-75]。这些表现可能与骨-髌腱-骨移植物自身供体发病率有关,患者在术后易出现膝前疼痛,需要更长的时间来恢复完全的膝关节活动度、减少积液、恢复股四头肌的力量[73]。 在功能性跳跃测试中,采用腓骨长肌肌腱移植物患者术后2年的连续跳跃活动能力恢复最好[76],这可能与移植物的直径和长度有关,腓骨长肌肌腱自身完整度较高并带有腱膜,能够保证良好的血液供应,且直径大小均匀,对折编织即可使用,编织好的肌腱力量均衡、强度更大,所需缝线相对较少,对周围组织刺激较小、损伤更低,因此并发症较少、患者恢复更快[23]。选用骨-髌腱-骨移植物患者术后4个月时单腿跳能力表现最差,而6-24个月时逐渐恢复[39],这种功能表现的改变与股四头肌肌力恢复趋势相关。选用股四头肌肌腱移植物患者比选用骨-髌腱-骨移植物患者显示出更强的跳跃能力[77],从长远来看,选用自体股四头肌肌腱移植物患者的跳跃功能恢复方面更具优势。相较于选用骨-髌腱-骨移植物患者,选用自体腘绳肌肌腱移植物患者虽然运动功能恢复评分更好、拥有较高的运动水平[75],但也在动态平衡和功能性跳跃测试方面存在缺陷,动态平衡测试显示动态后内侧方向的平衡缺失,而功能跳跃测试中的患侧缺失则以单腿三级跳和交叉跳最为显著,其相对于健侧缺失约为29.5%[69],这可能与腘绳肌肌腱移植取腱位置影响本体感觉和腘绳肌力量有关[78]。 选用同种异体移植物患者功能性活动在术后6个月时恢复较快,辛辛那提评分、Lysholm评分和Tegner活动水平量表得分较高,而在6-12个月时恢复变慢,这可能与同种异体移植物的特性有关,选用同种异体移植物具有手术时间短、供区发病率低、早期功能活动开展快速等优势,可帮助患者在术后早期进行功能恢复,但其成熟较慢和效率较低,再断裂风险大也成为了后期恢复变慢的影响因素[79]。对比自体移植物和人工韧带发现,人工韧带移植物组患者重建术后0.5-2年的功能评分均高于自体移植物组,选用人工韧带的患者具有较高的生活质量[29]。陈文祥等[80]研究也显示,LARS人工韧带组患者术后Lysholm评分和 IKDC评分均有显著改善。在功能恢复方面,人工韧带虽然能够提供早期的稳定性,但不利于韧带周围细胞增生和组织重建,人工韧带破裂将引起膝关节慢性炎症,因此初次前交叉韧带重建不建议采用人工韧带[71]。 2.5 移植物类型对前交叉韧带重建后患者重返运动的影响 重返运动指前交叉韧带重建后患者成功且安全地恢复伤前的竞技水平[81]。选用骨-髌腱-骨移植物患者术后每周运动参与时间为73%[82],在术后10个月时达到重返运动标准[83],可进行跑步和恢复竞技运动的人数分别达到了60%和47%[8],且进行双切口骨-髌腱-骨移植患者恢复跑步率高达95%[84]。选用自体腘绳肌肌腱移植物患者术后每周运动参与时间为48%[82],术后7.5 个月左右可重返运动[85],恢复跑步标准和恢复竞技运动标准的人数分别为84%和26%。选用股四头肌肌腱移植物患者术后5-8个月可达到重返运动的标准,能进行跑步和恢复竞技运动的患者分别可达到26%和13%[86]。选用腓骨长肌肌腱移植物患者尽管允许在2个月后开始慢跑,但一般在术后6个月左右可重返运动,这可能与具备完整的腱膜结构、韧带血液供应良好、恢复较快有关[87]。 与自体移植物相比,选用同种异体移植物患者术后需要更长的愈合时间,应延长康复和恢复比赛的时间4-8周,这与移植物在骨道内愈合情况有关[88]。选用同种异体移植物患者大约在术后6.5个月时即可重返跑步以及进行灵敏性等活动,达到重返运动的水平[89]。 使用人工韧带重建的患者恢复快,术后2个月内就被允许进行非竞技体育活动,并在三四个月之间就可完全恢复到伤前活动水平[90],其恢复体育运动的优良率高达92.3%[91]。"

| [1] DELLA VILLA F, BUCKTHORPE M, GRASSI A, et al. Systematic video analysis of ACL injuries in professional male football (soccer): injury mechanisms, situational patterns and biomechanics study on 134 consecutive cases. Br J Sports Med. 2020;54(23):1423-1432. [2] ALI N, ROUHI G. Barriers to predicting the mechanisms and risk factors of non-contact anterior cruciate ligament injury. Open Biomed Eng J. 2010;4:178-189. [3] RODRIGUEZ K, SONI M, JOSHI PK, et al. Anterior Cruciate Ligament Injury: Conservative Versus Surgical Treatment. Cureus. 2021;13(12):e20206. [4] PARSONS J, COEN S, BEKKER S. Anterior cruciate ligament injury: towards a gendered environmental approach. Br J Sports Med. 2021;55(17):984-990. [5] SVOBODA SJ. ACL injury and posttraumatic osteoarthritis. Clin Sports Med. 2014;33(4):633-640. [6] 张含霁,杨默笛,张卓,等.膝关节镜下前十字韧带重建术的研究进展[J].中国实验诊断学,2018,22(4):742-745. [7] 王宇驰,孙强,张卫国.交叉韧带重建中自体及同种异体移植物的研究进展[J].医学与哲学,2014(16):67-69. [8] HUGHES J, BURNHAM J, HIRSH A, et al. Comparison of Short-term Biodex Results After Anatomic Anterior Cruciate Ligament Reconstruction Among 3 Autografts. Orthop J Sports Med. 2019;7(5):2325967119847630. [9] 杨冬冬,曾伟,刘荆陵.股四头肌腱重建前交叉韧带的研究进展[J].实用骨科杂志,2021, 27(11):1010-1014,1051. [10] 李君芳.人工韧带重建与膝关节前交叉韧带的运动损伤[J].中国组织工程研究与临床康复,2010,14(12):2221-2224. [11] KOSY J, PHILLIPS J, EDORDU A, et al. Failure to Return to Preinjury Activity Level after Hamstring Anterior Cruciate Ligament Reconstruction: Factors Involved and Considerations in Goal Setting. Indian J Orthop. 2019;53(6):714-720. [12] 杨松杰,张清旭,陈绪彪,等.关节镜下膝交叉韧带重建中自体与异体肌腱移植物的疗效比较[J].中国组织工程研究,2017,21(34):5513-5518. [13] GROUP M. Effect of graft choice on the outcome of revision anterior cruciate ligament reconstruction in the Multicenter ACL Revision Study (MARS) Cohort. Am J Sports Med. 2014; 42(10):2301-2310. [14] 黄晋,杨松杰,翁科捷,等.自体肌腱与同种异体肌腱在膝关节前交叉韧带重建中的疗效比较[J].中国临床医生杂志,2016,44(10):53-56. [15] LIN K, BOYLE C, MAROM N, et al. Graft Selection in Anterior Cruciate Ligament Reconstruction. Sports Med Arthrosc Rev. 2020;28(2):41-48. [16] POULSEN MR, JOHNSON DL. Graft selection in anterior cruciate ligament surgery. Orthopedics. 2010;33(11):832. [17] KARTUS J, MAGNUSSON L, STENER S, et al. Complications following arthroscopic anterior cruciate ligament reconstruction. A 2-5-year follow-up of 604 patients with special emphasis on anterior knee pain. Knee Surg Sports Traumatol Arthrosc. 1999;7(1):2-8. [18] MILLER SL, GLADSTONE JN. Graft selection in anterior cruciate ligament reconstruction. Orthop Clin North Am. 2002;33(4):675-683. [19] 王宇驰,孙强,张卫国.交叉韧带重建中自体及同种异体移植物的研究进展[J].医学与哲学,2014(16):67-69. [20] SAMUELSEN BT, WEBSTER KE, JOHNSON NR, et al. Hamstring Autograft versus Patellar Tendon Autograft for ACL Reconstruction: Is There a Difference in Graft Failure Rate? A Meta-analysis of 47,613 Patients. Clin Orthop Relat Res. 2017;475(10):2459-2468. [21] SHAKKED R, WEINBERG M, CAPO J, et al. Autograft Choice in Young Female Patients: Patella Tendon versus Hamstring. J Knee Surg. 2017;30(3):258-263. [22] LETTER M, BARAGA M, BEST T, et al. Comparison of Neuromuscular Firing Patterns of the Superficial Quadriceps in Soft Tissue Quadriceps Tendon Versus Bone-Patellar Tendon-Bone ACL Autografts. Orthop J Sports Med. 2019;7(12):2325967119887674. [23] 袁振中,唐刚健,伍业雄,等.关节镜下自体腓骨长肌腱和腘绳肌腱重建前交叉韧带的对比研究[J]. 中国内镜杂志,2021,27(11):83-88. [24] 金钢,仲海燕,邵为,等.关节镜下自体腘绳肌腱与腓骨长肌腱单束重建前交叉韧带[J].中国矫形外科杂志,2019,27(24):2252-2256. [25] 赵意华,余进伟,杨志远,等.关节镜下自体腓骨长肌肌腱移植重建前交叉韧带术后临床效果分析[J].中国骨与关节损伤杂志,2016,31(8):864-865. [26] 张磊,周鑫,祁冀,等.取自体同侧1/2腓骨长肌肌腱重建膝关节前交叉韧带[J].中国组织工程研究,2017,21(24):3815-3820. [27] 李韬,朱彦霖,林唐棣,等.同种异体肌腱重建膝关节前交叉韧带的研究进展与临床应用[J].中国组织工程研究,2019,23(10):1605-1610. [28] SLONE H, ROMINE S, PREMKUMAR A, et al. Quadriceps tendon autograft for anterior cruciate ligament reconstruction: a comprehensive review of current literature and systematic review of clinical results. Arthroscopy. 2015;31(3):541-554. [29] 曹福洋,许建中,陆世涛,等.自体韧带与LARS人工韧带编织物重建前交叉韧带:骨隧道扩大值、韧带生长因子及膝关节功能的评价[J].中国组织工程研究,2022,26(21):3281-3290. [30] 谢正阳,周珍珍,刘志元,等.人工膝关节交叉韧带材料学及其特点[J].中国组织工程研究与临床康复,2010,14(12):2213-2216. [31] 陈伟,邹刚,刘毅.LARS韧带在前交叉韧带重建中的临床应用与关注热点[J].中国组织工程研究,2020,24(8):1287-1292. [32] 丁国成,刘铭,项良碧,等.人工韧带联合自体肌腱在前交叉韧带重建失败后翻修手术中应用[J].临床军医杂志,2017,45(8):809-812. [33] 陈天午,蒋佳,陈世益.人工韧带的临床应用现状及进展[J].宁夏医学杂志,2016,38(8): 673-676. [34] BUCKTHORPE M, LA ROSA G, VILLA F. Restoring Knee Extensor Strength After Anterior Cruciate Ligament Reconstruction: A Clinical Commentary. Int J Sports Phys Ther. 2019;14(1):159-172. [35] HUNNICUTT J, GREGORY C, MCLEOD M, et al. Quadriceps Recovery After Anterior Cruciate Ligament Reconstruction With Quadriceps Tendon Versus Patellar Tendon Autografts. Orthop J Sports Med. 2019;7(4):2325967119839786. [36] ABRAMS GD, HARRIS JD, GUPTA AK, et al. Functional Performance Testing After Anterior Cruciate Ligament Reconstruction: A Systematic Review. Orthop J Sports Med. 2014;2(1): 2325967113518305. [37] HEIJNE A, WERNER S. A 2-year follow-up of rehabilitation after ACL reconstruction using patellar tendon or hamstring tendon grafts: a prospective randomised outcome study. Knee Surg Sports Traumatol Arthrosc. 2010;18(6):805-813. [38] FELLER J, WEBSTER K, GAVIN B. Early post-operative morbidity following anterior cruciate ligament reconstruction: patellar tendon versus hamstring graft. Knee Surg Sports Traumatol Arthrosc. 2001;9(5):260-266. [39] CRISTIANI R, MIKKELSEN C, WANGE P, et al. Autograft type affects muscle strength and hop performance after ACL reconstruction. A randomised controlled trial comparing patellar tendon and hamstring tendon autografts with standard or accelerated rehabilitation. Knee Surg Sports Traumatol Arthrosc. 2021;29(9):3025-3036. [40] KWAK Y, LEE S, LEE M, et al. Anterior cruciate ligament reconstruction with quadriceps tendon-patellar bone allograft: matched case control study. BMC Musculoskelet Disord. 2018;19(1):45. [41] CHEN J, GU A, JIANG H, et al. A comparison of acute and chronic anterior cruciate ligament reconstruction using LARS artificial ligaments: a randomized prospective study with a 5-year follow-up. Arch Orthop Trauma Surg. 2015;135(1):95-102. [42] TASHIRO T, KUROSAWA H, KAWAKAMI A, et al. Influence of medial hamstring tendon harvest on knee flexor strength after anterior cruciate ligament reconstruction. A detailed evaluation with comparison of single- and double-tendon harvest. Am J Sports Med. 2003;31(4):522-529. [43] LAUTAMIES R, HARILAINEN A, KETTUNEN J, et al. Isokinetic quadriceps and hamstring muscle strength and knee function 5 years after anterior cruciate ligament reconstruction: comparison between bone-patellar tendon-bone and hamstring tendon autografts. Knee Surg Sports Traumatol Arthrosc. 2008;16(11):1009-1016. [44] KIM SJ, KIM TE, LEE DH, et al. Anterior cruciate ligament reconstruction in patients who have excessive joint laxity. J Bone Joint Surg Am. 2008;90(4):735-741. [45] 汪益,董启榕,许建铭,等.负重位磁共振成像对前交叉韧带重建术后膝关节稳定性的评估[J].中华医学杂志,2019,99(27):2130-2134. [46] 王艳,吴珊红,戚彪,等.振动疗法结合常规康复训练对前交叉韧带重建术后膝关节本体感觉及动态稳定性的影响[J].中国康复医学杂志,2021,36(7):858-862. [47] KIM S, KIM T, LEE D, et al. Anterior cruciate ligament reconstruction in patients who have excessive joint laxity. J Bone Joint Surg Am. 2008;90(4):735-741. [48] NOYES F, BUTLER D, PAULOS L, et al. Intra-articular cruciate reconstruction. I: Perspectives on graft strength, vascularization, and immediate motion after replacement. Clin Orthop Relat Res. 1983;(172):71-77. [49] GORADIA V, ROCHAT M, GRANA W, et al. Tendon-to-bone healing of a semitendinosus tendon autograft used for ACL reconstruction in a sheep model. Am J Knee Surg. 2000;13(3):143-151. [50] AKOTO R, ALBERS M, BALKE M, et al. ACL reconstruction with quadriceps tendon graft and press-fit fixation versus quadruple hamstring graft and interference screw fixation - a matched pair analysis after one year follow up. BMC Musculoskelet Disord. 2019;20(1):109. [51] JOSHI S, SHETTY UC, SALIM MD, et al. Peroneus Longus Tendon Autograft for Anterior Cruciate Ligament Reconstruction: A Safe and Effective Alternative in Nonathletic Patients. Niger J Surg. 2021;27(1):42-47. [52] ZHAO J, HUANGFU X. The biomechanical and clinical application of using the anterior half of the peroneus longus tendon as an autograft source. Am J Sports Med. 2012;40(3): 662-671. [53] 王林林,陈亚洲,刘培倦,等.自体移植、同种异体移植、混合移植在关节镜下前交叉韧带重建中的效果研究[J].吉林医学,2021,42(11):2606-2609. [54] TIAN S, WANG B, LIU L, et al. Irradiated Hamstring Tendon Allograft Versus Autograft for Anatomic Double-Bundle Anterior Cruciate Ligament Reconstruction: Midterm Clinical Outcomes. Am J Sports Med. 2016;44(10):2579-2588. [55] LI J, WANG J, LI Y, et al. A Prospective Randomized Study of Anterior Cruciate Ligament Reconstruction With Autograft, gamma-Irradiated Allograft, and Hybrid Graft. Arthroscopy. 2015;31(7):1296-1302. [56] SMITH CK, HOWELL SM, HULL ML. Anterior laxity, slippage, and recovery of function in the first year after tibialis allograft anterior cruciate ligament reconstruction. Am J Sports Med. 2011;39(1):78-88. [57] SUN K, TIAN SQ, ZHANG JH, et al. ACL reconstruction with BPTB autograft and irradiated fresh frozen allograft. J Zhejiang Univ Sci B. 2009;10(4):306-316. [58] TSAI SH, LEE CH, TONG KM, et al. Activity-related outcome in anterior cruciate ligament reconstruction with synthetic ligament advanced reinforcement system. J Chin Med Assoc. 2019;82(3):235-238. [59] JIA Z, XUE C, WANG W, et al. Clinical outcomes of anterior cruciate ligament reconstruction using LARS artificial graft with an at least 7-year follow-up. Medicine (Baltimore). 2017;96(14):e6568. [60] TIEFENBOECK TM, THURMAIER E, TIEFENBOECK MM, et al. Clinical and functional outcome after anterior cruciate ligament reconstruction using the LARS system at a minimum follow-up of 10 years. Knee. 2015;22(6):565-568. [61] MAGALHÃES J, OLIVEIRA J, ASCENSÃO A, et al. Concentric quadriceps and hamstrings isokinetic strength in volleyball and soccer players. J Sports Med Phys Fitness. 2004;44(2):119-125. [62] AGEBERG E, ROOS H, SILBERNAGEL K, et al. Knee extension and flexion muscle power after anterior cruciate ligament reconstruction with patellar tendon graft or hamstring tendons graft: a cross-sectional comparison 3 years post surgery. Knee Surg Sports Traumatol Arthrosc. 2009;17(2):162-169. [63] ÇELIK D, ÇOBAN Ö, KıLıÇOĞLU Ö. Minimal clinically important difference of commonly used hip-, knee-, foot-, and ankle-specific questionnaires: a systematic review. J Clin Epidemiol. 2019;113:44-57. [64] BRIGGS K, LYSHOLM J, TEGNER Y, et al. The reliability, validity, and responsiveness of the Lysholm score and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years late. Am J Sports Med. 2009;37(5):890-897. [65] 刘凯,宋伟,阮槟,等.前交叉韧带损伤后膝关节功能评估量表的研究进展[J].中国康复理论与实践,2019,25(12):1395-1399. [66] RAMOS MARINHO A, NUNES G, BENETTI M, et al. Cross-cultural adaptation and measurement properties of the Brazilian-Portuguese version of the Cincinnati Knee Rating System. Disabil Rehabil. 2020;42(8):1183-1189. [67] LUBIS AM, DASRIL DF. Comparison of functional outcome between bone quadriceps tendon (BQT) and single-bundle hamstring tendon (SBHT) autograft in arthroscopic-assisted anterior cruciate ligament reconstruction cases: a prospective cohort study. Ann Med Surg (Lond). 2020;60:509-514. [68] LOGERSTEDT D, GRINDEM H, LYNCH A, et al. Single-legged hop tests as predictors of self-reported knee function after anterior cruciate ligament reconstruction: the Delaware-Oslo ACL cohort study. Am J Sports Med. 2012;40(10):2348-2356. [69] SUGIMOTO D, HEYWORTH B, BRODEUR J, et al. Effect of Graft Type on Balance and Hop Tests in Adolescent Males Following Anterior Cruciate Ligament Reconstruction. J Sport Rehabil. 2019;28(5):468-475. [70] 李玉周,王婧怡.前交叉韧带损伤后手术及重返运动时机的选择[J].南阳师范学院学报, 2019,18(1):48-53. [71] YANG X, WANG F, HE X, et al. Network meta-analysis of knee outcomes following anterior cruciate ligament reconstruction with various types of tendon grafts. Int Orthop. 2020;44(2): 365-380. [72] 陈国民,袁松,张廷玖,等.腓骨长肌腱与腘绳肌腱重建前交叉韧带中期疗效比较[J].中国现代手术学杂志,2022,26(4):270-276. [73] SMITH A, CAPIN J, ZARZYCKI R, et al. Athletes With Bone-Patellar Tendon-Bone Autograft for Anterior Cruciate Ligament Reconstruction Were Slower to Meet Rehabilitation Milestones and Return-to-Sport Criteria Than Athletes With Hamstring Tendon Autograft or Soft Tissue Allograft : Secondary Analysis From the ACL-SPORTS Trial. J Orthop Sports Phys Ther. 2020;50(5):259-266. [74] HANTES M, FYLLOS A, PAPAGEORGIOU F, et al. Long-term clinical and radiological outcomes after multiligament knee injury using a delayed ligament reconstruction approach: A single-center experience. Knee. 2019;26(6):1271-1277. [75] CRISTIANI R, SARAKATSIANOS V, ENGSTRÖM B, et al. Increased knee laxity with hamstring tendon autograft compared to patellar tendon autograft: a cohort study of 5462 patients with primary anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2019;27(2):381-388. [76] RHATOMY S, HARTOKO L, SETYAWAN R, et al. Single bundle ACL reconstruction with peroneus longus tendon graft: 2-years follow-up. J Clin Orthop Trauma. 2020;11(Suppl 3):S332-S336. [77] PIGOZZI F, DI SALVO V, PARISI A, et al. Isokinetic evaluation of anterior cruciate ligament reconstruction: quadriceps tendon versus patellar tendon. J Sports Med Phys Fitness. 2004; 44(3):288-293. [78] 覃华生,潘玮敏,李然,等.自体腘绳肌腱重建前交叉韧带后的康复策略[J].中国组织工程研究,2019,23(4): 628-635. [79] CUSUMANO A, CAPITANI P, MESSINA C, et al. Different timing in allograft and autograft maturation after primary anterior cruciate ligament reconstruction does not influence the clinical outcome at mid-long-term follow-up. Knee Surg Sports Traumatol Arthrosc. 2022;30(7): 2281-2290. [80] 陈文祥,谢煜,包倪荣,等.关节镜下LARS人工韧带与自体腘绳肌腱对前交叉韧带重建的早期疗效比较[J].医学研究生学报,2017,30(2):165-168. [81] BIEN DP, DUBUQUE TJ. Considerations for late stage acl rehabilitation and return to sport to limit re-injury risk and maximize athletic performance. Int J Sports Phys Ther. 2015;10(2):256-271. [82] WEBSTER K, FELLER J, HARTNETT N, et al. Comparison of Patellar Tendon and Hamstring Tendon Anterior Cruciate Ligament Reconstruction: A 15-Year Follow-up of a Randomized Controlled Trial. Am J Sports Med. 2016;44(1):83-90. [83] WALSTON Z, BARILLAS R. The impact of graft type on rehabilitation outcomes following ACL reconstruction: Bone patellar tendon bone versus quadriceps tendon grafts. Phys Ther Sport. 2021;52:234-238. [84] O’NEILL D. Arthroscopically assisted reconstruction of the anterior cruciate ligament. A prospective randomized analysis of three techniques. J Bone Joint Surg Am. 1996;78(6):803-813. [85] CAVAIGNAC E, COULIN B, TSCHOLL P, et al. Is Quadriceps Tendon Autograft a Better Choice Than Hamstring Autograft for Anterior Cruciate Ligament Reconstruction? A Comparative Study With a Mean Follow-up of 3.6 Years. Am J Sports Med. 2017;45(6):1326-1332. [86] LEE S, SEONG SC, JO CH, et al. Anterior cruciate ligament reconstruction with use of autologous quadriceps tendon graft. J Bone Joint Surg Am. 2007;89 Suppl 3:116-126. [87] HOSSAIN GMJ, ISLAM MS, RAHMAN KHAN MM, et al. A prospective study of arthroscopic primary ACL reconstruction with ipsilateral peroneus longus tendon graft: Experience of 439 cases. Medicine (Baltimore). 2023;102(9):e32943. [88] SINGHAL M, GARDINER J, JOHNSON D. Failure of primary anterior cruciate ligament surgery using anterior tibialis allograft. Arthroscopy. 2007;23(5):469-475. [89] SMITH AH, CAPIN JJ, ZARZYCKI R, et al. Athletes With Bone-Patellar Tendon-Bone Autograft for Anterior Cruciate Ligament Reconstruction Were Slower to Meet Rehabilitation Milestones and Return-to-Sport Criteria Than Athletes With Hamstring Tendon Autograft or Soft Tissue Allograft : Secondary Analysis From the ACL-SPORTS Trial. J Orthop Sports Phys Ther. 2020;50(5):259-266. [90] MACHOTKA Z, SCARBOROUGH I, DUNCAN W, et al. Anterior cruciate ligament repair with LARS (ligament advanced reinforcement system): a systematic review. Sports Med Arthrosc Rehabil Ther Technol. 2010;2:29. [91] PARCHI P, GIANLUCA C, DOLFI L, et al. Anterior cruciate ligament reconstruction with LARS™ artificial ligament results at a mean follow-up of eight years. Int Orthop. 2013;37(8):1567-1574. [92] ABOUREZK M, ITHURBURN M, MCNALLY M, et al. Hamstring Strength Asymmetry at 3 Years After Anterior Cruciate Ligament Reconstruction Alters Knee Mechanics During Gait and Jogging. Am J Sports Med. 2017;45(1):97-105. [93] JALALI M, FARAHMAND F, ESFANDIARPOUR F, et al. The effect of functional bracing on the arthrokinematics of anterior cruciate ligament injured knees during lunge exercise. Gait Posture. 2018;63:52-57. [94] LOWE WR, WARTH RJ, DAVIS EP, et al. Functional Bracing After Anterior Cruciate Ligament Reconstruction: A Systematic Review. J Am Acad Orthop Surg. 2017;25(3):239-249. [95] NIEDERER D, KELLER M, ACHTNICH A, et al. Effectiveness of a home-based re-injury prevention program on motor control, return to sport and recurrence rates after anterior cruciate ligament reconstruction: study protocol for a multicenter, single-blind, randomized controlled trial (PReP). Trials. 2019;20(1):495. [96] 王雪臣,魏威,王力兴,等.关节镜下同侧腓骨长肌腱重建前交叉韧带的疗效及对踝关节、足功能的影响[J].河北医药,2023,45(12):1803-1806,1811. [97] YANKE AB, BELL R, LEE A, et al. The biomechanical effects of 1.0 to 1.2 Mrad of gamma irradiation on human bone-patellar tendon-bone allografts. Am J Sports Med. 2013;41(4):835-840. [98] KAYA D, GUNEY-DENIZ H, SAYACA C, et al. Effects on Lower Extremity Neuromuscular Control Exercises on Knee Proprioception, Muscle Strength, and Functional Level in Patients with ACL Reconstruction. Biomed Res Int. 2019;2019:1694695. [99] NELSON IR, CHEN J, LOVE R, et al. A comparison of revision and rerupture rates of ACL reconstruction between autografts and allografts in the skeletally immature. Knee Surg Sports Traumatol Arthrosc. 2016;24(3):773-779. [100] CIPOLLA M, SCALA A, GIANNI E, et al. Different patterns of meniscal tears in acute anterior cruciate ligament (ACL) ruptures and in chronic ACL-deficient knees. Classification, staging and timing of treatment. Knee Surg Sports Traumatol Arthrosc. 1995;3(3):130-134. |
| [1] | Wu Jing, Yao Yingce, Yang Xiaowei, Xue Boshi, Zhao Jianbin, Yang Chen, Luan Tianfeng, Zhou Zhipeng. Intervention of muscle strength training combined with neuromuscular electrical stimulation on lower limb function and biomechanical changes in patients with patellofemoral pain [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(9): 1365-1371. |
| [2] | Qi Haodong, Lu Chao, Xu Hanbo, Wang Mengfei, Hao Yangquan. Effect of diabetes mellitus on perioperative blood loss and pain after primary total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(9): 1383-1387. |
| [3] | Bai Chen, Yang Wenqian, Meng Zhichao, Wang Yuze. Strategies for repairing injured anterior cruciate ligament and promoting graft healing [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(9): 1457-1463. |
| [4] | Zhang Xihui, Li Zhengrong, Li Shineng, Xing Zengyu, Wang Jiao. Effect of rehabilitation training guided by Pro-kin balance system on proprioception and balance function of the affected knee after anterior cruciate ligament reconstruction [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(8): 1259-1264. |
| [5] | Zhang Ming, Wang Bin, Jia Fan, Chen Jie, Tang Wei. Application of brain-computer interface technology based on electroencephalogram in upper limb motor function rehabilitation of stroke patients [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(4): 581-586. |
| [6] | Wang Juan, Wang Ling, Zuo Huiwu, Zheng Cheng, Wang Guanglan, Chen Peng. Rehabilitative efficacy of kinesio taping following anterior cruciate ligament reconstruction: a Meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(4): 651-656. |
| [7] | Yan Hailong, Huo Jiangtao, Zhou Wucheng, Bai Xuehua, Liang Yuanyuan. Application and mechanism of tissue flossing in sports and rehabilitation [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(3): 464-471. |
| [8] | Wang Chunhong, Lu Ming. Universal stepwise rehabilitation training promotes the functional recovery of quadriceps femoris after intertrochanteric femoral fracture surgery [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(26): 4216-4220. |
| [9] | Wang Yuetong, Peng Liang, Su Yuying, Liu Jiajun. Effect of balance training on chronic ankle instability: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(24): 3930-3936. |
| [10] | Xie Enli, Tao Huimin. Application trends of blood flow restriction training in clinical rehabilitation [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(2): 258-262. |
| [11] | Lyu Moran, Xu Wenxin, Wang Di, Li Ming. New trends and developments of functional training research in the field of health care [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(2): 302-307. |
| [12] | Chang Wanpeng, Zhang Zhongwen, Yang Yulin, Zi Yang, Yang Mengqi, Du Bingyu, Wang Nan, Yu Shaohong. Efficacy of rehabilitation exoskeleton robots on post-stroke lower limb motor dysfunction: a Meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(2): 321-328. |
| [13] | Liu Guoli, Li Liang, Xie Kunnan, Yin Xianghui, Zhang Yanrui, Yi Fan, Dai Shifeng. Application of different grafts in anterior cruciate ligament revision [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(17): 2647-2652. |
| [14] | Wang Ling, Jiang Xia, Chen Peng, Zheng Cheng, Xu Jinrong. Biomechanical characteristics of the lower limbs of athletes after anterior cruciate ligament reconstruction during bilateral vertical jumping [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(14): 2215-2220. |
| [15] | Xiong Bohan, Lu Xiaojun, Xue Wenqiang, Liu Jinrui, Gao Xianling, Yu Hong, Li Yajuan, Liu Haolong, Li Yanlin. Protective effect of anterior cruciate ligament reconstruction assisted by internal tension-reduction technique on the articular cartilage of southern Yunnan small-ear pigs [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(14): 2221-2226. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||