Chinese Journal of Tissue Engineering Research ›› 2016, Vol. 20 ›› Issue (35): 5187-5194.doi: 10.3969/j.issn.2095-4344.2016.35.003
Previous Articles Next Articles
Effects of compression and non-compression fusion cage on lumbar fusion
Gu Yong, Wang Ling-jun, Chen Liang
- Department of Orthopedic Surgery, the First Affiliated Hospital of Soochow University, Suzhou 215006, Jiangsu Province, China
-
Revised:2016-06-23Online:2016-08-26Published:2016-08-26 -
Contact:Chen Liang, M.D., Chief physician, Professor, Doctoral supervisor, Department of Orthopedic Surgery, the First Affiliated Hospital of Soochow University, Suzhou 215006, Jiangsu Province, China -
About author:Gu Yong, Master, Attending physician, Department of Orthopedic Surgery, the First Affiliated Hospital of Soochow University, Suzhou 215006, Jiangsu Province, China -
Supported by:the National Natural Science Foundation of China, No. 81371930, 81071450; the Social Development-Standardized Diagnosis and Treatment Project of Jiangsu Province, No. BE2015641; the General Project of Natural Science Foundation of Higher Learning School of Jiangsu Province, No. 15KJB320012
CLC Number:
Cite this article
Gu Yong, Wang Ling-jun, Chen Liang. Effects of compression and non-compression fusion cage on lumbar fusion[J]. Chinese Journal of Tissue Engineering Research, 2016, 20(35): 5187-5194.
share this article

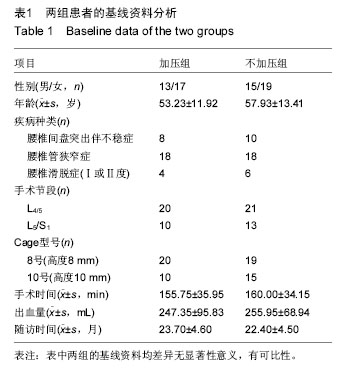
2.1 参与者数量分析 纳入随访患者共计70例,中途退出及失访6例,无新受试者纳入,最终计入结果分析64例,其中加压组30例,不加压组34例。 2.2 患者基线资料分析 两组性别、年龄、疾病种类,融合节段、cage型号、手术时间及出血量的差异均无显著性意义(表1)。"
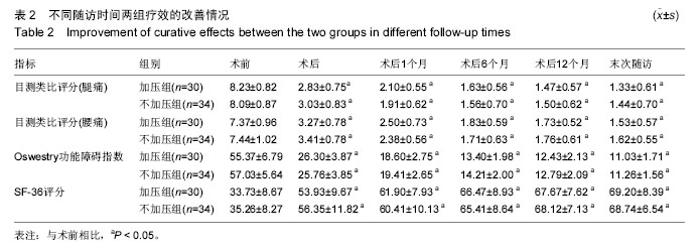
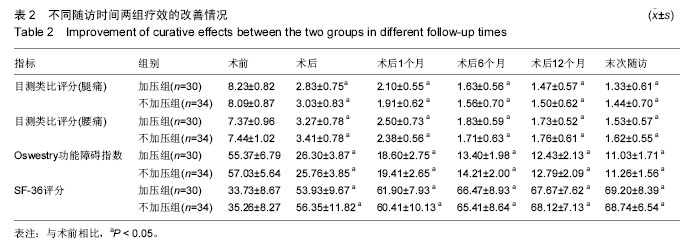
2.3 两组疗效差异 所有患者均获得随访,随访时间15-31个月,平均(23.0±4.6)个月。术后每组腿痛目测类比评分、腰痛目测类比评分、Oswestry功能障碍指数及SF-36评分均较术前明显改善(P < 0.05;表2)。"
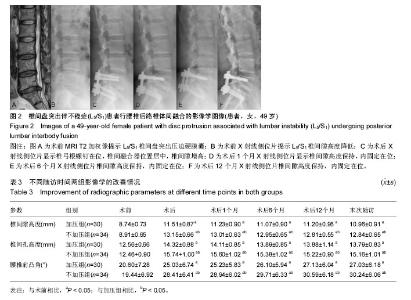
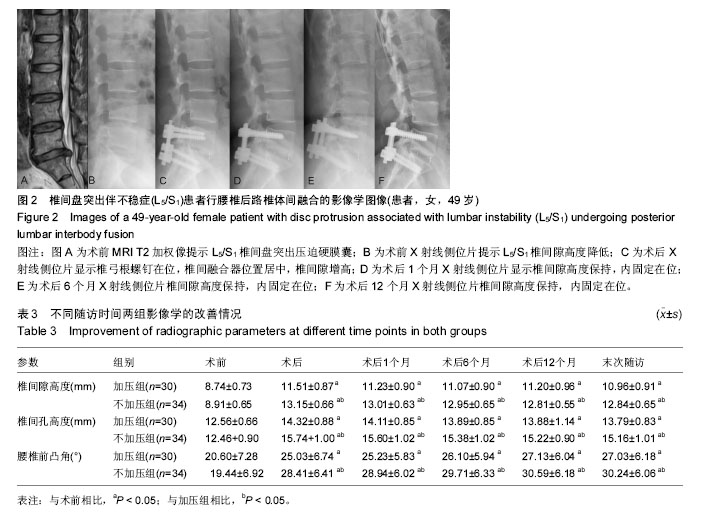
2.4 两组腰椎影像学特点 术后每组椎间隙高度、椎间孔高度及腰椎前凸角均较术前明显改善(P < 0.05;表3);而术后不同时刻差异均无显著性意义。术后不同时刻,不加压组的椎间隙高度、椎间孔高度及腰椎前凸角均高于加压组(P < 0.05)。术后6个月时加压组融合率为76.7%,不加压组融合率为70.6%,两组差异无显著性意义;术后12个月时融合率分别为93.3%及91.2%;而末次随访时分别为100%及97.1%,两组差异均无显著性意义。 2.5 两组疗效与影像学之间的相关性 加压组椎间隙及椎间孔高度的增加与腿痛目测类比评分、Oswestry功能障碍指数及SF-36评分的改善无明显相关性(椎间隙高度与腿痛目测类比评分:r=-0.23,P=0.23;椎间隙高度与Oswestry功能障碍指数:r=-0.19,P=0.35;椎间隙高度与SF-36:r=0.08,P=0.69;椎间孔高度与腿痛目测类比评分:r=0.06,P=0.75;椎间孔高度与Oswestry功能障碍指数:r=0.22,P=0.25;椎间孔高度与SF-36:r=0.00,P=1.00)。 不加压组椎间隙及椎间孔高度的增加与腿痛目测类比评分、Oswestry功能障碍指数及SF-36评分的改善也无相关性(椎间隙高度与腿痛目测类比评分:r= 0.07,P=0.68;椎间隙高度与Oswestry功能障碍指数:r=0.18,P=0.32;椎间隙高度与SF-36:r=0.05,P=0.79。椎间孔高度与腿痛目测类比评分:r=-0.28,P=0.11;椎间孔高度与Oswestry功能障碍指数:r=-0.04,P=0.83;椎间孔高度与SF-36:r=-0.23,P=0.19)。 2.6 两组并发症情况分析 加压组1例硬膜囊撕裂,予以缝合,术后无脑脊液漏;2例患侧下肢根性痛加重,1例出现对侧下肢根性痛,予以脱水消肿及神经营养,3周内好转。不加压组2例硬膜囊撕裂,予以缝合,其中1例脑脊液漏,予以头低脚高位,切口加压包扎,换药2周,伤口愈合;1例患肢根性痛加重,神经营养2周后恢复。随访期间未见椎弓根螺钉松动或断裂,或融合器移位。 2.7 典型病例 患者,女,49岁,L5/S1椎间盘突出伴不稳症,施行腰椎后路椎体间融合,椎间融合器予以加压固定,随访17个月,无融合器移位或下沉,无椎弓根螺钉松动或断裂,见图2。"
| [1] Aizawa T, Kokubun S, Ozawa H, et al. Increasing incidence of degenerative spinal diseases in Japan during 25 years: the registration system of spinal surgery in Tohoku University Spine Society. Tohoku J Exp Med. 2016;238(2):153-163. [2] Pereira BJ, de Holanda CV, Ribeiro CA, et al. Spinal surgery for degenerative lumbar spine disease: predictors of outcome. Clin Neurol Neurosurg. 2016; 140:1-5. [3] Hoppe S, Schwarzenbach O, Aghayev E, et al. Long-term outcome after monosegmental L4/5 stabilization for degenerative spondylolisthesis with the Dynesys device. Clin Spine Surg. 2016;29(2): 72-77. [4] Lu SB, Hai Y, Kong C, et al. An 11-year minimum follow-up of the Charite III lumbar disc replacement for the treatment of symptomatic degenerative disc disease. Eur Spine J. 2015;24(9):2056-2064. [5] 米东,杨明坤,张旭,等.椎弓根螺钉系统内固定联合椎间融合器修复腰椎峡部裂性滑脱症:椎间隙高度恢复的评价[J].中国组织工程研究,2014,18(44):7122-7126. [6] Lee GW, Lee SM, Ahn MW, et al. Comparison of posterolateral lumbar fusion and posterior lumbar interbody fusion for patients younger than 60 years with isthmic spondylolisthesis. Spine. 2014;39(24): E1475-E1480. [7] Liu XY, Qiu GX, Weng XS, et al. What is the optimum fusion technique for adult spondylolisthesis -PLIF or PLF or PLIF plus PLF? A meta-analysis from 17 comparative studies. Spine. 2014;39(22):1887-1898. [8] Zdeblick TA, Phillips FM. Interbody cage devices. Spine. 2003;28(15 Suppl):S2-S7. [9] Blumenthal SL, Ohnmeiss DD; NASS. Intervertebral cages for degenerative spinal diseases. Spine J. 2003; 3(4):301-309. [10] Zhao J, Hou T, Wang X, et al. Posterior lumbar interbody fusion using one diagonal fusion cage with transpedicular screw/rod fixation. Eur Spine J. 2003; 12(2):173-177. [11] Kaito T, Hosono N, Fuji T, et al. Disc space distraction is a potent risk factor for adjacent disc disease after PLIF. Arch Orthop Trauma Surg. 2011;131(11):1499-1507. [12] Liu J, Deng H, Long X, et al. A comparative study of perioperative complications between transforaminal versus posterior lumbar interbody fusion in degenerative lumbar spondylolisthesis. Eur Spine J, 2016;25(5):1575-1580. [13] Sears W. Posterior lumbar interbody fusion for degenerative spondylolisthesis: restoration of sagittal balance using insert-and-rotate interbody spacers. Spine J. 2005;5(2):170-179. [14] Wewers ME, Lowe NK. A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health. 1990;13(4):227-236. [15] Fairbank JC, Pynsent PB. The Oswestry Disability Index. Spine. 2000;25(22):2940-2952. [16] Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992; 30(6):473-483. [17] McHorney CA, Ware JE Jr, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care. 1993; 31(3):247-263. [18] McHorney CA, Ware JE Jr, Lu JF, et al. The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care. 1994; 32(1):40-66. [19] Liu X, Wang Y, Qiu G, et al. A systematic review with meta-analysis of posterior interbody fusion versus posterolateral fusion in lumbar spondylisthesis. Eur Spine J. 2014;23(1):43-56. [20] Cinotti G, Santis PD, Nofroni I, et al. Stenosis of lumbar intervertebral foramen anatomic study on predisposing factors. Spine. 2002;27:223-229. [21] Mehta VA, McGirt MJ, Garcs Ambrossi GL, et al. Trans-foraminal versus posterior lumbar interbody fusion: comparison of surgical morbidity. Neurol Res. 2011;33(1):38-42. [22] Lain FC, Alkalay R, Greff MW. The effects of design and positioning of carbon fiber lumbar interbody cages and their subsidence in vertebral bodies. J Spinal Disord Tech. 2012;25:116-122. [23] Oh KW, Lee JH, Lee JH, et al. The correlation between cage subsidence, bone mineral density, and clinical results in posterior lumbar interbody fusion. J Spinal Disord Tech. 2015. [24] 王洪立,姜建元,吕飞舟,等.腰椎融合器后移的原因分析及处理对策[J].中华骨科杂志,2012,32(10):916-921. [25] Kimura H, Shikata J, Odate S, et al. Risk factors for cage retropulsion after posterior lumbar interbody fusion: analysis of 1070 cases. Spine. 2012;37(13): 1164-1169. [26] Chen L, Yang H, Tang T. Cage migration in spondylolisthesis treated with posterior lumbar interbody fusion using BAK cages. Spine. 2005;30(19):2171-2175. [27] Verbiest H. Results of surgical treatment of idiopathic development stenosis of the lumbar vertebral canal. J Bone Joint Surg Br. 1977;59(2):181-188 [28] Yasar B, Simsek S, Er U, et al. Functional and clinical evaluation for the surgical treatment of degenerative stenosis of the lumbar spinal canal. J Neurosurg Spine. 2009;11(3):347-352. [29] Sobottke R, Schluter-Brust K, Kaulhausen T, et al. Interspinous implants (X Stop, Wallis, Diam) for the treatment of LSS: is there a correlation between radiological parametersand clinical outcome. Eur Spine J. 2009;18(10):1494-1503. [30] Abdul QR, Qayum MS, Saradhi MV, et al. Clinico-radiological profile of indirect neural decompression using cage or auto graft as interbody construct in posterior lumbar interbody fusion in spondylolisthesis: which is better. J Craniovertebr Junction Spine. 2011;2(1):12-16. [31] 孙永生,孙卫东,温建民,等.腰椎后路椎体间融合的改良:椎间融合器植入联合椎体间颗粒状骨加压植骨术[J].中华损伤与修复杂志,2010,5(5):592-603. [32] Alimi M, Shin B, Macielak M, et al. Expandable polyaryl-ether-ether-ketone spacers for interbody distraction in the lumbar spine. Global Spine J. 2015; 5(3):169-178. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||