Chinese Journal of Tissue Engineering Research ›› 2019, Vol. 23 ›› Issue (8): 1282-1290.doi: 10.3969/j.issn.2095-4344.1054
Previous Articles Next Articles
Posterior cruciate-retaining versus posterior cruciate-stabilized prostheses for total knee arthroplasty: a meta-analysis
Shi Junheng1, Zhong Degui1, Fan Zhirong1, Huang Yongquan2
- 1Guangzhou University of Chinese Medicine, Guangzhou 510006, Guangdong Province, China; 2Guangdong Provincial Hospital of Traditional Chinese Medicine, Guangzhou 510120, Guangdong Province, China
-
Online:2019-03-18Published:2019-03-18 -
Contact:Huang Yongquan, Master, Guangdong Provincial Hospital of Traditional Chinese Medicine, Guangzhou 510120, Guangdong Province, China -
About author:Shi Junheng, Doctoral candidate, Guangzhou University of Chinese Medicine, Guangzhou 510006, Guangdong Province, China -
Supported by:the Research Project of Traditional Chinese Medicine Bureau of Guangdong Province, No. 20182043 (to HYQ)
CLC Number:
Cite this article
Shi Junheng, Zhong Degui, Fan Zhirong, Huang Yongquan. Posterior cruciate-retaining versus posterior cruciate-stabilized prostheses for total knee arthroplasty: a meta-analysis[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(8): 1282-1290.
share this article
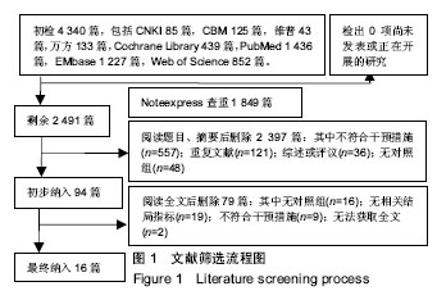
2.1 文献筛选过程 检索各数据库共计检索到4 340篇文献,Noteexpress软件查重排除1 849篇文献。根据既定纳入排除标准,阅读文献题目和摘要排除762篇文献,初步纳入59篇文献。详细阅读全文后,排除46篇文献,最终共纳入13篇,都是已经公开发表的文献,文献筛选流程图见图1。"
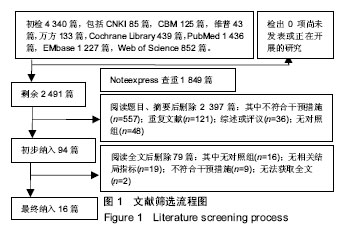

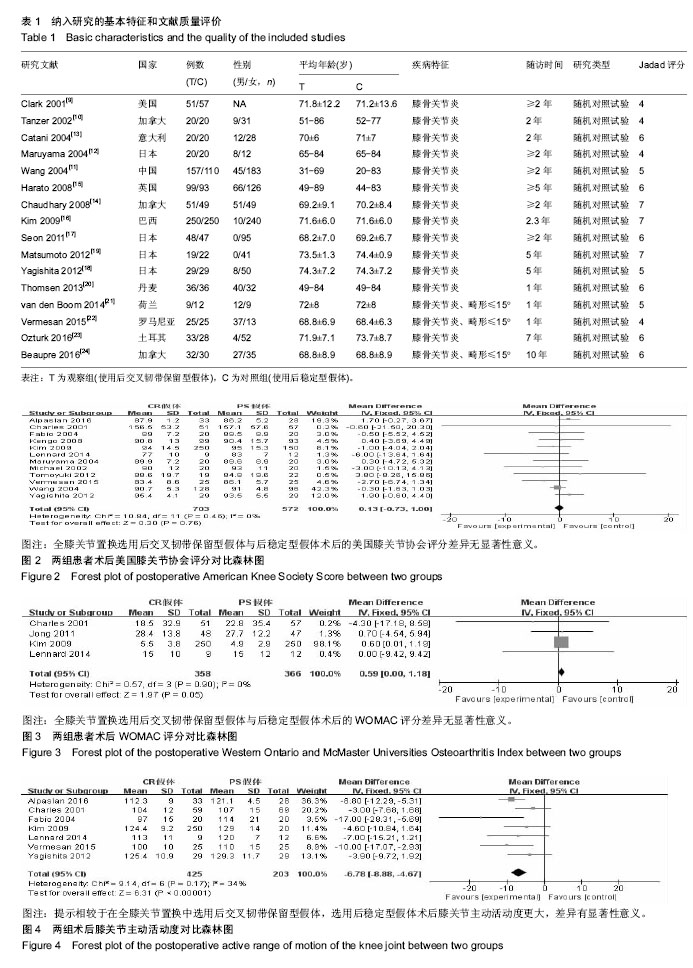
2.2 纳入文献的基本特征和文献质量评价 此次研究中观察组是在全膝关节置换术中使用后交叉韧带保留型假体,对照组是在全膝关节置换术中使用后稳定型假体。共纳入16个随机对照试验[9-24],有1 747例患者行全膝关节置换术,其中观察组的899例患者采用后交叉韧带保留型假体,对照组有848例患者采用后稳定型假体。所有纳入的随机对照试验中均报道了纳入排除标准,且方法学质量均较好,Jadad评分都在4分及以上,Jadad评分最低分是4分,最高分则达到7分。纳入研究的一般情况详见表1。 2.3 结局指标Meta分析 2.3.1 术后美国膝关节协会评分 有12项研究报道了全膝关节置换术后美国膝关节协会评分[9-13,15-16,18-19,21-23],其中后交叉韧带保留型假体组患者703例、后稳定型假体组患者572例。经异质性检验,χ2=10.84,P=0.46≥ 0.1,I2=0%,即12项纳入的研究之间存在同质性,因而应用固定效应模型合并,[MD=0.13,95%CI(-0.73,1.00)],合并效应量检验,Z=0.30,P=0.76 > 0.05,提示全膝关节置换选用后交叉韧带保留型假体与后稳定型假体术后的美国膝关节协会评分差异无显著性意义,见图2。 2.3.2 术后WOMAC评分 有4项研究报道了全膝关节置换术后WOMAC评分[9,16-17,21],其中后交叉韧带保留型假体组患者358例、后稳定型假体组患者366例。经异质性检验,χ2= 0.57,P=0.90≥ 0.1,I2=0%,即4项纳入的研究之间存在同质性,因而应用固定效应模型合并,[MD=0.59,95%CI(0.00,1.18)],合并效应量检验,Z=1.97,P=0.05≥0.05,提示全膝关节置换选用后交叉韧带保留型假体与后稳定型假体术后的WOMAC评分差异无显著性意义,见图3。 2.3.3 术后膝关节主动活动度 有7项研究报道了全膝关节置换术后膝关节主动活动度[9,13,16,18,21-23],其中后交叉韧带保留型假体组患者425例、后稳定型假体组患者203例。经异质性检验,χ2=9.14,P=0.17≥ 0.1,I2=34%,即7项纳入的研究之间存在同质性,因而应用固定效应模型合并, [MD=-6.78,95%CI (-8.88,-4.67)],合并效应量检验,Z=6.31,P < 0.000 01,提示相较于在全膝关节置换中选用后交叉韧带保留型假体,选用后稳定型假体术后膝关节主动活动度更大,差异有显著性意义,见图4。"

2.3.4 术后膝关节伸直活动度 有5项研究报道了全膝关节置换术后膝关节伸直活动度[12,14,18,21,23],其中后交叉韧带保留型假体组患者131例、后稳定型假体组患者127例。经异质性检验,χ2=4.92,P=0.30≥ 0.1,I2=19%,即5项纳入的研究之间存在同质性,因而应用固定效应模型合并,[MD=0.04,95%CI (-0.36,0.45)],合并效应量检验,Z=0.21,P=0.84≥ 0.05,提示全膝关节置换选用后交叉韧带保留型假体与后稳定型假体术后膝关节伸直活动度的差异无显著性意义,见图5。 2.3.5 术后膝关节屈曲活动度 有10项研究报道了全膝关节置换术后膝关节屈曲活动度[10,12,14-15,17-21,23],其中后交叉韧带保留型假体组患者350例、后稳定型假体组患者346例。经异质性检验,χ2=14.04,P=0.12≥ 0.1,I2=36%,即10项纳入的研究之间存在同质性,因而应用固定效应模型合并,[MD=-4.22,95%CI (-6.03,-2.41)],合并效应量检验,Z=4.57,P < 0.000 01,提示相较于在全膝关节置换中选用后交叉韧带保留型假体,选用后稳定型假体术后膝关节屈曲活动度更大,差异有显著性意义,见图6。 2.3.6 术后机械胫股角 有3项研究报道了全膝关节置换术后机械胫股角[11,17-18],其中后交叉韧带保留型假体组患者205例、后稳定型假体组患者172例。经异质性检验,χ2= 2.36,P=0.31≥ 0.1,I2=15%,即3项纳入的研究之间存在同质性,因而应用固定效应模型合并,[MD=0.85,95%CI (0.46,1.25)],合并效应量检验,Z=4.25,P < 0.000 1,提示相较于在全膝关节置换中选用后交叉韧带保留型假体,选用后稳定型假体术后机械胫股角更小,更接近于理想的6°机械胫股角[25],差异有显著性意义,见图7。 2.3.7 术后胫骨后倾角 有4项研究报道了全膝关节置换术后胫骨后倾角[13,16-17,22],其中后交叉韧带保留型假体组患者347例、后稳定型假体组患者346例。经异质性检验, χ2=4.27,P=0.23≥ 0.1,I2=30%,即4项纳入的研究之间存在同质性,因而应用固定效应模型合并,[MD=-0.09,95%CI (-0.52,0.33)],合并效应量检验,Z=0.43,P=0.67,提示全膝关节置换选用后交叉韧带保留型假体与后稳定型假体术后胫骨后倾角的差异无显著性意义,见图8。 2.3.8 术后膝关节疼痛残留率 有7项研究报道了全膝关节置换术后膝关节疼痛残留率[10,12-13,15-16,18,22],其中后交叉韧带保留型假体组患者463例、后稳定型假体组患者457例,后交叉韧带保留型假体组术后出现膝关节疼痛残留14例,后稳定型假体组术后出现膝关节疼痛残留11例。经异质性检验,χ2=3.06,P=0.69≥ 0.1,I2=0%,即7项纳入的研究之间存在同质性,因而应用固定效应模型合并,[OR=1.26,95%CI (0.57,2.78)],合并效应量检验,Z=0.56,P=0.58 > 0.05,提示全膝关节置换选用后交叉韧带保留型假体与后稳定型假体术后膝关节疼痛残留率的差异无显著性意义,见图9。"

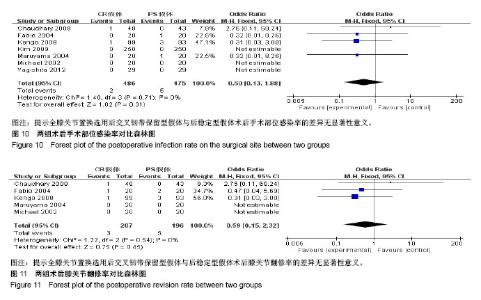
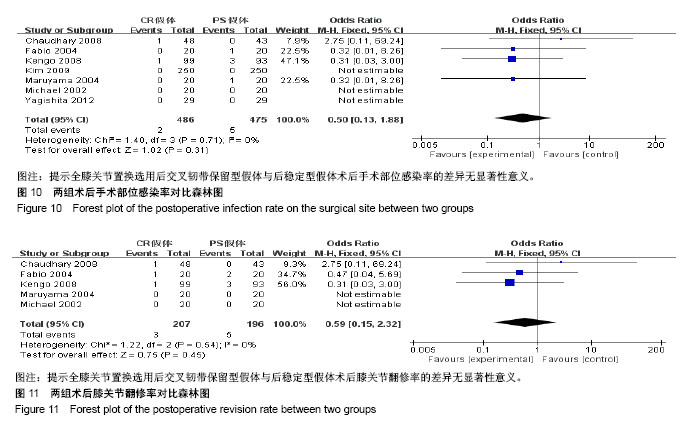
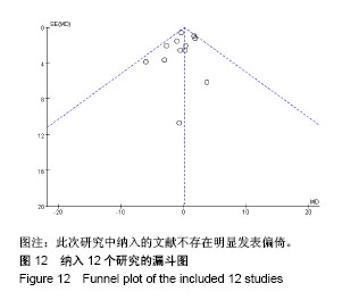
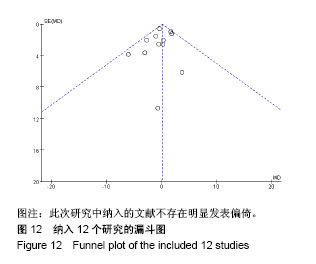
2.3.9 术后手术部位感染率 有7项研究报道了全膝关节置换术后手术部位感染率[10,12-16,18],其中后交叉韧带保留型假体组患者486例、后稳定型假体组患者475例,后交叉韧带保留型假体组术后出现手术部位感染2例,后稳定型假体组术后出现手术部位感染5例。经异质性检验,χ2=1.40,P=0.71≥ 0.1,I2=0%,即7项纳入的研究之间存在同质性,因而应用固定效应模型合并,[OR=0.50,95%CI (0.13,1.88)],合并效应量检验,Z=1.02,P=0.31 > 0.05,提示全膝关节置换选用后交叉韧带保留型假体与后稳定型假体术后手术部位感染率的差异无显著性意义,见图10。 2.3.10 术后膝关节翻修率 有5项研究报道了全膝关节置换术后膝关节翻修率[10,12-15],其中后交叉韧带保留型假体组患者207例、后稳定型假体组患者196例,后交叉韧带保留型假体组术后出现手术部位感染3例,后稳定型假体组术后出现手术部位感染5例。经异质性检验,χ2=1.22,P=0.54≥ 0.1,I2=0%,即5项纳入的研究之间存在同质性,因而应用固定效应模型合并,[OR=0.59,95%CI(0.15,2.32)],合并效应量检验,Z=0.75,P=0.45 > 0.05,提示全膝关节置换选用后交叉韧带保留型假体与后稳定型假体术后膝关节翻修率的差异无显著性意义,见图11。 2.3.11 漏斗图分析 16个纳入的研究中有12个以术后美国膝关节协会评分作为结局指标,在这项结局指标的Meta分析中,只有1研究分布在漏斗图底部,其他研究散在分布于漏斗图的上部,漏斗图上部的结果分布大致对称,且这12个研究的结果都在规定区间范围内,表明此次研究中纳入的文献不存在明显发表偏倚,见图12。"
"
| [1] Sherman MF, Warren RF, Marshall JL, et al. A clinical and radiographical analysis of 127 anterior cruciate insufficient knees. Clin Orthop Relat Res. 1988;227:229-237.[2] Johnson DL, Urban WJ, Caborn DN, et al. Articular cartilage changes seen with magnetic resonance imaging-detected bone bruises associated with acute anterior cruciate ligament rupture. Am J Sports Med. 1998;26(3):409-414.[3] Nielsen A B, Yde J. Epidemiology of acute knee injuries: a prospective hospital investigation. J Trauma. 1991;31(12): 1644-1648.[4] Ritter MA, Lutgring JD, Davis KE, et al. Total knee arthroplasty effectiveness in patients 55 years old and younger: osteoarthritis vs. rheumatoid arthritis. Knee. 2007;14(1):9-11.[5] Swanik CB, Lephart SM, Rubash HE. Proprioception, kinesthesia, and balance after total knee arthroplasty with cruciate-retaining and posterior stabilized prostheses. J Bone Joint Surg Am. 2004;86-A(2):328-334.[6] Conditt MA, Noble PC, Bertolusso R, et al. The PCL significantly affects the functional outcome of total knee arthroplasty. J Arthroplasty. 2004;19(7 Suppl 2):107-112.[7] Straw R, Kulkarni S, Attfield S, et al. Posterior cruciate ligament at total knee replacement. Essential, beneficial or a hindrance? J Bone Joint Surg Br. 2003;85(5):671-674.[8] Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17(1):1-12.[9] Clark CR, Rorabeck CH, MacDonald S, et al. Posterior-stabilized and cruciate-retaining total knee replacement: a randomized study. Clin Orthop Relat Res, 2001(392):208-212.[10] Tanzer M, Smith K, Burnett S. Posterior-stabilized versus cruciate-retaining total knee arthroplasty: balancing the gap. J Arthroplasty. 2002;17(7):813-819.[11] Wang CJ, Wang JW, Chen HS. Comparing cruciate-retaining total knee arthroplasty and cruciate-substituting total knee arthroplasty: a prospective clinical study. Chang Gung Med J. 2004;27(8):578-585.[12] Maruyama S, Yoshiya S, Matsui N, et al. Functional comparison of posterior cruciate-retaining versus posterior stabilized total knee arthroplasty. J Arthroplasty. 2004;19(3): 349-353.[13] Catani F, Leardini A, Ensini A, et al. The stability of the cemented tibial component of total knee arthroplasty: posterior cruciate-retaining versus posterior-stabilized design. J Arthroplasty. 2004;19(6):775-782.[14] Chaudhary R, Beaupre LA, Johnston DW. Knee range of motion during the first two years after use of posterior cruciate-stabilizing or posterior cruciate-retaining total knee prostheses. A randomized clinical trial. J Bone Joint Surg Am. 2008;90(12):2579-2586.[15] Harato K, Bourne RB, Victor J, et al. Midterm comparison of posterior cruciate-retaining versus -substituting total knee arthroplasty using the Genesis II prosthesis. A multicenter prospective randomized clinical trial. Knee. 2008;15(3): 217-221.[16] Kim YH, Choi Y, Kwon OR, et al. Functional outcome and range of motion of high-flexion posterior cruciate-retaining and high-flexion posterior cruciate-substituting total knee prostheses. A prospective, randomized study. J Bone Joint Surg Am. 2009;91(4):753-760.[17] Seon JK, Park JK, Shin YJ, et al. Comparisons of kinematics and range of motion in high-flexion total knee arthroplasty: cruciate retaining vs. substituting designs. Knee Surg Sports Traumatol Arthrosc. 2011;19(12):2016-2022.[18] Yagishita K, Muneta T, Ju YJ, et al. High-flex posterior cruciate-retaining vs posterior cruciate-substituting designs in simultaneous bilateral total knee arthroplasty: a prospective, randomized study. J Arthroplasty. 2012;27(3):368-374.[19] Matsumoto T, Muratsu H, Kubo S, et al. Intraoperative soft tissue balance reflects minimum 5-year midterm outcomes in cruciate-retaining and posterior-stabilized total knee arthroplasty. J Arthroplasty. 2012;27(9):1723-1730.[20] Thomsen MG, Husted H, Otte KS, et al. Do patients care about higher flexion in total knee arthroplasty? A randomized, controlled, double-blinded trial. BMC Musculoskelet Disord. 2013;14:127.[21] van den Boom LG, Halbertsma JP, van Raaij JJ, et al. No difference in gait between posterior cruciate retention and the posterior stabilized design after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014;22(12):3135-3141.[22] Vermesan D, Trocan I, Prejbeanu R, et al. Reduced operating time but not blood loss with cruciate retaining total knee arthroplasty. J Clin Med Res. 2015;7(3):171-175.[23] Ozturk A, Akalin Y, Cevik N, et al. Posterior cruciate-substituting total knee replacement recovers the flexion arc faster in the early postoperative period in knees with high varus deformity: a prospective randomized study. Arch Orthop Trauma Surg. 2016;136(7):999-1006.[24] Beaupre LA, Sharifi B, Johnston D. A Randomized Clinical Trial Comparing Posterior Cruciate-Stabilizing vs Posterior Cruciate-Retaining Prostheses in Primary Total Knee Arthroplasty: 10-Year Follow-Up. J Arthroplasty. 2017;32(3): 818-823.[25] 汪锡龙,尚希福,李国远,等. 个体化股骨远端外翻角度截骨技术在初次人工全膝关节置换术中的应用[J]. 中国修复重建外科杂志, 2015,29(1):27-30.[26] 吴彦生,李永胜,陈百成. 后交叉韧带保留与否对膝关节本体感觉的影响[J]. 中国修复重建外科杂志, 2013,27(7):851-854.[27] Matsumoto T, Muratsu H, Kubo S, et al. Soft tissue tension in cruciate-retaining and posterior-stabilized total knee arthroplasty. J Arthroplasty. 2011;26(5):788-795.[28] 吴伟山. 应用CR型和PS型人工膝关节假体置换术后早期临床疗效分析[D]. 济南:山东中医药大学, 2016.[29] 吕新凯. CR型假体与PS型假体全膝置换的早期临床疗效对比[D]. 济南:山东大学, 2014.[30] White SH, O'Connor JJ, Goodfellow JW. Sagittal plane laxity following knee arthroplasty. J Bone Joint Surg Br. 1991;73(2): 268-270.[31] Lee SM, Seong SC, Lee S, et al. Outcomes of the different types of total knee arthroplasty with the identical femoral geometry. Knee Surg Relat Res. 2012;24(4):214-220.[32] Chaudhary R, Beaupre LA, Johnston DW. Knee range of motion during the first two years after use of posterior cruciate-stabilizing or posterior cruciate-retaining total knee prostheses. A randomized clinical trial. J Bone Joint Surg Am. 2008;90(12):2579-2586.[33] Lee SM, Seong SC, Lee S, et al. Outcomes of the different types of total knee arthroplasty with the identical femoral geometry. Knee Surg Relat Res. 2012;24(4):214-220.[34] Becker R, Hirschmann MT, Karlsson J. The role of ligament tension and sensomotoric system in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2017;25(6):1663-1665.[35] Callaghan JJ, O'Rourke MR, Goetz DD, et al. Tibial post impingement in posterior-stabilized total knee arthroplasty. Clin Orthop Relat Res. 2002;(404):83-88.[36] 罗世兴,赵劲民,苏伟,等. 保留和不保留后交叉韧带全膝置换疗效的Meta分析[J]. 中国矫形外科杂志, 2010,18(14):1145-1149.[37] 陈良军. 保留和不保留后交叉韧带的全膝关节置换术的系统评价[D]. 南宁:广西医科大学, 2010.[38] Victor J, Banks S, Bellemans J. Kinematics of posterior cruciate ligament-retaining and -substituting total knee arthroplasty: a prospective randomised outcome study. J Bone Joint Surg Br. 2005;87(5):646-655.[39] Vermesan D, Prejbeanu R, Laitin S, et al. Meniscal tears left in situ during anatomic single bundle anterior cruciate ligament reconstruction. Eur Rev Med Pharmacol Sci. 2014; 18(2):252-256.[40] 王林,宋磊,韩伟峰. 全膝关节置换术中后交叉韧带保留与切除与否的对比研究[J]. 首都医科大学学报, 2017,38(6):915-918.[41] Pang HN, Yeo SJ, Chong HC, et al. Joint line changes and outcomes in constrained versus unconstrained total knee arthroplasty for the type II valgus knee. Knee Surg Sports Traumatol Arthrosc. 2013;21(10):2363-2369.[42] Abdel MP, Morrey ME, Jensen MR, et al. Increased long-term survival of posterior cruciate-retaining versus posterior cruciate-stabilizing total knee replacements. J Bone Joint Surg Am. 2011;93(22):2072-2078.[43] 凌卓彦,李柳炳,董启榕. 全膝关节置换术中切除后交叉韧带的优缺点[J]. 中国骨与关节损伤杂志, 2009,24(10):958-960.[44] Ishii Y, Noguchi H, Takeda M, et al. Prediction of range of motion 2 years after mobile-bearing total knee arthroplasty: PCL-retaining versus PCL-sacrificing. Knee Surg Sports Traumatol Arthrosc. 2011;19(12):2002-2008. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Zhang Yu, Tian Shaoqi, Zeng Guobo, Hu Chuan. Risk factors for myocardial infarction following primary total joint arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1340-1345. |
| [3] | Li Dadi, Zhu Liang, Zheng Li, Zhao Fengchao. Correlation of total knee arthroplasty efficacy with satisfaction and personality characteristics [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1346-1350. |
| [4] | Wei Wei, Li Jian, Huang Linhai, Lan Mindong, Lu Xianwei, Huang Shaodong. Factors affecting fall fear in the first movement of elderly patients after total knee or hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1351-1355. |
| [5] | Wang Jinjun, Deng Zengfa, Liu Kang, He Zhiyong, Yu Xinping, Liang Jianji, Li Chen, Guo Zhouyang. Hemostatic effect and safety of intravenous drip of tranexamic acid combined with topical application of cocktail containing tranexamic acid in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1356-1361. |
| [6] | Xiao Guoqing, Liu Xuanze, Yan Yuhao, Zhong Xihong. Influencing factors of knee flexion limitation after total knee arthroplasty with posterior stabilized prostheses [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1362-1367. |
| [7] | Huang Zexiao, Yang Mei, Lin Shiwei, He Heyu. Correlation between the level of serum n-3 polyunsaturated fatty acids and quadriceps weakness in the early stage after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1375-1380. |
| [8] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [9] | Yuan Jiawei, Zhang Haitao, Jie Ke, Cao Houran, Zeng Yirong. Underlying targets and mechanism of Taohong Siwu Decoction in prosthetic joint infection on network pharmacology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1428-1433. |
| [10] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [11] | Chen Jinping, Li Kui, Chen Qian, Guo Haoran, Zhang Yingbo, Wei Peng. Meta-analysis of the efficacy and safety of tranexamic acid in open spinal surgery [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1458-1464. |
| [12] | Hu Kai, Qiao Xiaohong, Zhang Yonghong, Wang Dong, Qin Sihe. Treatment of displaced intra-articular calcaneal fractures with cannulated screws and plates: a meta-analysis of 15 randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1465-1470. |
| [13] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Comparison of the short-term efficacy of extracorporeal shock wave therapy for middle-aged and elderly knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1471-1476. |
| [14] | Wang Yongsheng, Wu Yang, Li Yanchun. Effect of acute high-intensity exercise on appetite hormones in adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1305-1312. |
| [15] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||