Chinese Journal of Tissue Engineering Research ›› 2026, Vol. 30 ›› Issue (21): 5614-5620.doi: 10.12307/2026.327
Previous Articles Next Articles
Bone grafting for repairing scaphoid nonunion
Guo Wen, Gao Binli, Wang Yang, Lin Sen
- Department of Orthopedics, Affiliated Hospital of Inner Mongolia Medical University, Hohhot 010030, Inner Mongolia Autonomous Region, China
-
Accepted:2025-04-16Online:2026-07-28Published:2026-03-06 -
Contact:Lin Sen, MS, Associate chief physician, Department of Orthopedics, Affiliated Hospital of Inner Mongolia Medical University, Hohhot 010030, Inner Mongolia Autonomous Region, China -
About author:Guo Wen, MS, Attending physician, Department of Orthopedics, Affiliated Hospital of Inner Mongolia Medical University, Hohhot 010030, Inner Mongolia Autonomous Region, China
CLC Number:
Cite this article
Guo Wen, Gao Binli, Wang Yang, Lin Sen. Bone grafting for repairing scaphoid nonunion[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(21): 5614-5620.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
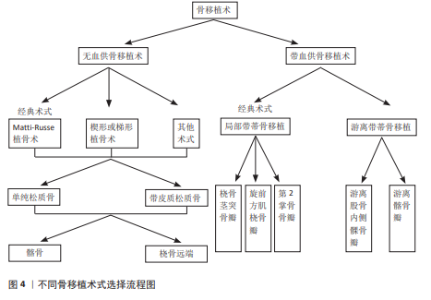
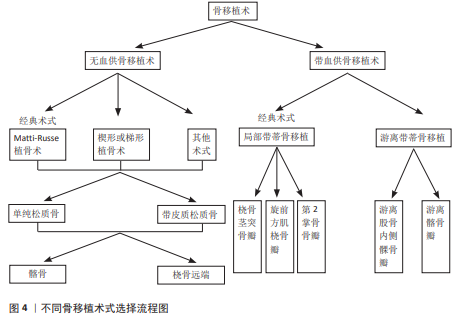
2.1 无血供的骨移植术治疗舟骨骨折不愈合 尽管骨移植术用于治疗腕舟骨骨折已有很长的历史,但腰部和近端舟状骨骨折不愈合仍然是手外科医生面临的挑战[13]。无血供的骨移植是一种可靠的治疗手舟骨骨折不愈合的方法,同样是目前比较主流的手术方式[14],经典的植骨方式常包括Matti-Russe植骨术、楔形或梯形植骨术及其他多种植骨术[9],上述手术方式的植骨供体常来源于髂骨和桡骨远端[15],植骨类型常括单纯松质骨和带皮质的松质骨两种。无血供骨移植术的选择见图4。 2.1.1 经典的骨移植方式 (1)Matti-Russe植骨术:此方法首先由德国波恩医生HERMANN MATTI在1937年提出,并率先应用于临床,他采用背侧入路刮除折端所有死骨、软骨和纤维组织,并刮出一个骨槽,插入松质骨;1956年奥地利维也纳医生Russe对Matti的术式作出了改良:他采用掌侧入路,在骨折处刮出卵圆形的骨腔植入矩形骨栓,并在周围填充松质骨条,故后来称为Matti-Russe 植骨术,并从此被广泛应用于临床。但现在看来Matti-Russe植骨术仅适用于简单、对线好的骨折,不愈合且近侧骨折块完全缺血者不适合使用该法。 (2)楔形或梯形植骨术:1970年,FISK[16]经桡侧入路切除桡骨茎突暴露舟骨,并用切下的茎突修整为楔形或梯形填充舟骨缺损。1984年FERNANDEZ对上述方法作出改良,利用影像学资料提前评估好缺损的形状和大小同时取相应的髂骨进行移植,结合内固定很大程度上提高了骨折的愈合率。 (3)其他术式:1934年MURRAY率先描述纵行骨栓植骨[17];1979年ERBS等报道了使用双凹形植骨[17];1988年殷铭东等[18]应用同种异体骨植骨、1998年SANDOW[19]采用肋骨软骨进行舟骨置换等,上述方法均获得了满意的临床疗效。 2.1.2 不同类型的骨移植物 (1)单纯的松质骨移植:对于不需要纠正畸形且无骨坏、移位较小的舟骨骨折不愈合,单纯松质骨移植加坚强内固定可以达到很好的治疗效果,已成为大多数外科医生的治疗选择。YASUDA等[20]研究显示在28例舟骨骨折不愈合患者中,采用掌侧入路从桡骨远端打磨成双凹松质骨进行移植,克氏针内固定,获得了100%的愈合率,且未见并发症的发生。BAE等[21]采用桡骨远端松质骨移植物和无头螺钉固定治疗31例不稳定腰部舟状骨骨不连患者,愈合率达到93.3%,并获得了良好的腕关节功能。 (2)带皮质松质骨移植:对于骨坏死、骨缺损、驼背畸形的舟骨骨折不愈合,临床上常使用带皮质松质骨移植物来纠正舟状骨缩短和掌侧成角[4]。SCH?FER等[22]在对16例复杂顽固性手舟骨骨折不愈合患者进行治疗时,使用自体带皮质松质骨进行移植辅助加压螺钉内固定,通过长达平均54个月的随访,术后通过腕关节功能和影像学评定,得出皮质松质骨移植辅助加压螺钉内固定是一种很好的方法。HEGAZY等[23]选择122例不稳定腰部舟骨骨折不愈合患者随机分成2组,分别接受自体皮质松质髂骨植骨结合多根克氏针或赫伯特螺钉内固定,结果显示两组的愈合率分别为91%和 88%。MARKOWICZ等[24]对48例术后舟骨骨折不愈合患者进行自体带皮质松质骨移植手术,愈合率达88%,进一步证明皮质松质骨移植是一种有效的外科术式,不仅有助于骨折愈合而且有助于恢复舟骨的形态和长度,还可以很好地预防创伤后腕关节炎。 虽然单纯松质骨和带皮质松质骨在最终促进骨折愈合方面无明显差异,但二者各有优缺点。HEGAZY等[25]于2006年将98例舟状骨骨折不愈合的患者随机分成2组,其中一组患者接受自体单纯松质骨移植,另一组采用带皮质松质骨移植,二者均采用掌侧入路,使用3 mm赫伯特螺钉进行固定,结果显示在骨折愈合方面二者没有明显差异;但是单纯松质骨移植物具有更强的成骨能力,愈合时间明显较皮质松质骨缩短;带皮质松质骨具有更高的骨密度,具有很好的支撑作用,可以更好地恢复舟状骨高度、腕关节面平整度,显著改善腕关节功能,在纠正骨折畸形方面更有优势。SAYEGH等[26]在2014年的回顾性分析中纳入604例患者,对术后骨折愈合率和腕关节功能评分进行综合评价分析后得出同样的结论。KIM等[27]连续治疗了38例腰部不稳定舟骨骨折不愈合的患者,采用带皮质松质骨和单纯松质骨移植结合不同内固定方式得出同样的结论。 (3)不同供体部位对手舟骨骨折不愈合的影响:骨移植的首选供体部位仍有待明确,但研究表明无论供体部位是髂骨还是桡骨远端对舟骨的愈合率和腕关节功能恢复方面并无明显差异[28]。TAMBE等[29]回顾性研究了68例采用带皮质松质骨移植治疗有症状的舟骨骨折不愈合患者,其中44例来自用髂骨,24例来自桡骨远端,结果显示二者在愈合率、腕关节平整度和腕关节功能恢复方面无明显差异。DUNCUMB等[30]在一项关于自体骨移植治疗舟骨不愈合的系统回顾和荟萃分析中证实,移植物来源对愈合率无明显影响。SHIN等[31]在2024年对38例舟骨折不愈合患者(其中桡骨远端组15例,髂骨组23例)进行皮质松质骨移植内固定治疗,结果进一步证实上述结论,但在供区并发症方面,桡骨远端明显低于髂骨[32]。 2.2 带血供的骨移植术治疗骨折不愈合 带血供骨移植术的选择见图4。 2.2.1 局部带血管蒂骨瓣移植 随着对腕部血管解剖认识的提高和显微外科技术的进步,带血管蒂骨移植物越来越多地被应用于舟状骨骨折不愈合。相比于传统的非血管化骨移植物,带血管的骨移植物为直接愈合而非爬行替代过程,舟骨骨折不愈合的血运重建更快、丢失的骨量更少、骨质融合更快和骨形态更好。目前常用的局部带蒂骨瓣包括桡骨茎突骨瓣、旋前方肌带蒂桡骨瓣、第二掌骨带蒂骨瓣等。 (1)桡骨茎突骨瓣:是以桡动脉茎突返支为蒂切取大小合适的骨瓣逆行嵌入舟骨缺损骨槽中并进行内固定,同时根据具体情况可适当辅助外固定[33-34]。1987年王成琪等[35]使用上述方法治疗10例舟骨骨折不愈合均获得愈合,但并未正式命名;1990年何尚宽和郭涛等首次报道了桡动脉茎突返支为蒂的骨瓣治疗舟骨骨折不愈合并获得成功[36];后来ZAIDEMBERG等[37]于1991年提出同样术式;SCHEETZ等[38]于1995年做了更详尽的研究及报道,现已被广泛用于临床;?OLAK等[39]收集了2014-2018年68例舟骨骨折不愈合的患者,用桡动脉茎突返支骨瓣逆行转移结合克氏针或螺钉内固定,平均随访31.6个月,最终骨折愈合率高达81%,同时腕关节功能得到了很好的改善。2023年MOHIUDDIN等[34]用上述方法治疗了50例舟骨骨折不愈合的患者,同样取得了很高的愈合率和很好的腕关节功能,进一步证实了桡骨茎突骨瓣对于舟骨骨折不愈合是一种很好的治疗选择。邢志利等[40]随访了采用桡骨茎突骨瓣治疗18例舟骨骨不愈合患者得出了同样的结论。 (2)旋前方肌带蒂桡骨瓣:即将旋前方肌、桡骨骨膜、桡骨骨片一同取下形成以旋前方肌为蒂的骨瓣嵌入舟骨缺损骨槽中同时进行内固定[41]。1983年,BRAUN[42]报道采用旋前方肌桡骨瓣成功治疗了5例舟骨骨折不愈合患者,其中包括2例Russe植骨失败的患者。1998年,日本的KAWAI和YAMAMOTO等详细介绍了旋前方肌桡骨瓣的手术要点[17]。此外,KAPOOR等[43]在2013年使用旋前方肌蒂骨瓣结合内固定治疗2例手舟骨骨折不愈合患者,6个月时骨折完全愈合,2年后完全恢复到了受伤前的腕关节功能。2015年一项利用带旋前方肌蒂骨瓣和无头加压螺钉治疗27例舟骨骨折不愈合患者的回顾性研究中,获得了良好的愈合率和满意的腕关节功能[44]。?ZDEMIR等[45]在2022年进行的带旋前方肌蒂骨瓣移植与自体骨移植治疗舟骨骨折不愈合的对比研究中发现,旋前方肌带蒂桡骨瓣组16例患者愈合率为93.3%,自体骨移植组24例患者愈合率为79.2%,两组术后Mayo腕关节评分差异无显著性意义,证明旋前方肌带血管带蒂肌皮瓣治疗缺血型舟骨骨折不愈合要优于自体骨移植。 旋前方肌的血供来源丰富且呈多元性,主要供血动脉为骨间前动脉。选择旋前方肌带蒂桡骨瓣是因为旋前方肌解剖变异少且血供来源丰富;尽管此方法取得了成功,但目前并未成为治疗舟骨骨折不愈合的主流方式。 (3)第2掌骨带蒂骨瓣:是以桡动脉发出的第1骨间背侧肌浅动脉和深动脉为蒂营养第2掌骨干和掌骨头为基础设计的带血管蒂骨瓣。1996年马玉林等[46]采用第2,3掌骨带蒂骨瓣治疗25例陈旧性舟骨骨折,随访7个月至5年,结果显示23例骨愈合,1例失访,1例舟骨头部硬化,功能优良率为95.8%,证实了该术式操作简单,对腕部血管网破坏小,可明显缩短骨折愈合时间,特别适用于舟骨骨折不愈合的患者。SAWAIZUMI等[47]在2004年使用第2掌骨带蒂骨瓣治疗14例手舟骨骨折不愈合患者,在10.2周后所有患者均获得很好的骨折愈合,进一步证实了该术式是一种治疗舟骨骨折不愈合的有效方法。 2.2.2 游离骨瓣 对于难治性舟骨骨折不愈合或者合并舟骨近极缺血坏死的患者而言,游离骨瓣同样是一个不错的选择,由于其相对恒定的血管走行、较粗的管径,可以获得精准且足够的移植骨量,愈合率高、愈合时间短,目前被广泛应用于临床。目前最常用的两种游离骨瓣包括游离股骨内髁骨瓣和游离髂骨瓣。 (1)游离股骨内侧髁骨(软骨)瓣:游离股骨内侧髁骨(软骨)瓣是以膝降动横支(或少见的膝内上动脉分支)为蒂切取的股骨内侧髁软骨(骨)瓣(必要时可同时切取观察皮岛),重建舟骨软骨关节面是其突出的优点。周家顺[48]以膝降动脉关节支为蒂切取股骨内髁游离骨瓣治疗5例舟骨近端缺血坏死病例,手术彻底清除了坏死的腕舟骨近端并重建了一个类似于解剖学上带关节面软骨的舟骨凸段,同时恢复了桡舟关节及舟月关节的解剖关系,术后所有患者腕部疼痛均明显缓解,腕关节功能均达到优良标准,而骨瓣供区功能完全正常。KORIEM等[49]回顾性分析了使用游离股骨内侧髁骨(软骨)瓣进行治疗的16例腕舟骨骨折不愈合患者,随访至术后24个月发现舟骨骨折愈合率极高,舟骨畸形及腕关节功能都得到了很大的改善。ZHOU等[50]通过文献检索回顾性分析了262例腕舟骨不愈合通过游离股骨内侧髁骨(软骨)瓣治疗的患者,同样得出此术式是治疗舟骨骨折不愈合一种很好的选择,但由于其对手术者的显微技术要求较高,目前还不能被广泛应用于大部分基层医院。 (2)游离髂骨瓣:游离髂骨瓣是以旋髂深动、静脉为蒂切取的髂骨瓣,又称为Pechlaner-Hussl带血管骨移植术,是因为PECHLANER等首先用吻合旋髂深动静脉的髂骨移植治疗舟骨不愈合取得了很好的效果,由于该术式血管蒂走行恒定、管径适宜被广泛应用于临床[17]。HARPF等[51]报道使用同样的方法治疗60例舟骨骨折不愈合患者,愈合率为 91.7%。邹阳平等[52]以旋髂深血管为蒂切取游离髂骨瓣治疗9 例陈旧性骨折不愈合患者并随访10个月,结果显示了100%的愈合率,进一步证明游离髂骨瓣治疗舟骨骨折不愈合临床效果确切、骨愈合更快、并发症少、预后良好。"
| [1] NAKAMURA T. Scaphoid Fracture/Nonunion. J Wrist Surg. 2024;13(3):193. [2] BASSO MA, SMERAGLIA F, OCAMPOS-HERNANDEZ M, et al. Scaphoid fracture non-union: a systematic review of the arthroscopic management. Acta Biomed. 2023;94(5):e2023194. [3] GUZZINI M, LANZETTI RM, PROIETTI L, et al. The role of vascularized flaps in the treatment of proximal pole avascular necrosis in scaphoid non-unions. Acta Biomed. 2019;90(12-s):64-68. [4] VAN NEST D, ILYAS AM. Scaphoid Nonunion: A Review of Surgical Strategies. Orthopedics. 2022;45(5):e235-e242. [5] DUCKWORTH AD, JENKINS PJ, AITKEN SA, et al. Scaphoid fracture epidemiology. J Trauma Acute Care Surg. 2012;72(2):E41-5. [6] KAKAR S, BISHOP AT, SHIN AY. Role of vascularized bone grafts in the treatment of scaphoid nonunions associated with proximal pole avascular necrosis and carpal collapse. J Hand Surg. 2011;36(4):722-725; quiz 5. [7] FUJIHARA Y, YAMAMOTO M, HIDAKA S, et al. Vascularised versus non-vascularised bone graft for scaphoid nonunion: Meta-analysis of randomised controlled trials and comparative studies. JPRAS open. 2023;35:76-88. [8] AL-JABRI T, MANNAN A, GIANNOUDIS P. The use of the free vascularised bone graft for nonunion of the scaphoid: a systematic review. J Orthop Surg Res. 2014;9:21. [9] 曹树明, 张建兵, 詹海华, 等. 陈旧性腕舟状骨骨折的治疗进展[J]. 中国矫形外科杂志,2021,29(15):1392-1395. [10] STEINMANN SP, ADAMS JE. Scaphoid fractures and nonunions: diagnosis and treatment. J Orthop Sci. 2006;11(4): 424-431. [11] REIGSTAD O, GRIMSGAARD C, THORKILDSEN R, et al. Scaphoid non-unions, where do they come from? The epidemiology and initial presentation of 270 scaphoid non-unions. Hand Surg. 2012;17(3):331-335. [12] 陈山林, 田光磊. 舟骨骨折不愈合的植骨术[J].中华关节外科杂志(电子版), 2010,4(2):150-154. [13] DUSTMANN M, BAJINSKI R, TRIPP A, et al. A modified Matti-Russe technique of grafting scaphoid non-unions. Arch Orthop Trauma Surg. 2017;137(6):867-873. [14] TAVAKOLIAN PA, ADAMS NS, EDWARDS SG. Scaphoid Nonunion Volar Plating with Pure Nonvascularized Cancellous Autograft. JBJS Essent Surg Tech. 2021;11(2):e20.00029. [15] MAHAPATRA S, AGGARWAL P, MISHRA P, et al. Outcome of Scaphoid Nonunion Using Open Reduction and Internal Fixation With Iliac Crest Bone Graft (Fisk-Fernandez Technique). Cureus. 2023;15(2):e34661. [16] FISK GR. Carpal instability and the fractured scaphoid. Ann Royal Coll Surg Eng. 1970; 46(2):63-76. [17] 刘泳君, 闫立伟, 周翔, 等. 植骨术治疗舟骨骨折不愈合的研究进展[J]. 中华创伤骨科杂志,2021,23(5):453-457. [18] 殷铭东,刘光东,张新宇,等. 深低温冷冻同种异体骨植入治疗腕舟骨陈旧性骨折[J].中华骨科杂志,1995(7):479. [19] SANDOW MJ. Proximal scaphoid costo-osteochondral replacement arthroplasty. J Hand Surg (Edinburgh, Scotland). 1998; 23(2):201-208. [20] YASUDA M, ANDO Y, MASADA K. Treatment of scaphoid nonunion using volar biconcave cancellous bone grafting. Hand Surg. 2007; 12(2):135-140. [21] BAE JY, CHOI SW, LEE W, et al. Cancellous bone graft from the distal radius and headless screw fixation for unstable scaphoid waist nonunion. Int Orthop. 2024; 48(2):487-493. [22] SCHÄFER RC, NUSCHE A, EINZMANN A, et al. The corticocancellous press fit iliac crest bone dowel for recalcitrant scaphoid nonunion: analysis of union rate and clinical outcome. Arch Orthop Trauma Surg. 2023;143(9):6001-6010. [23] HEGAZY G, ALSHAL E, ABDELAAL M, et al. Kirschner wire versus Herbert screw fixation for the treatment of unstable scaphoid waist fracture nonunion using corticocancellous iliac bone graft: randomized clinical trial. Int Orthop. 2020;44(11):2385-2393. [24] MARKOWICZ A, BACZKOWSKI B, LORCZYŃSKI A, et al. Evaluating degenerative changes in the wrist after surgical treatment for scaphoid pseudarthrosis using a corticocancellous graft for anatomical reconstruction. Ortop Traumatol Rehabil. 2006;8(5):495-506. [25] HEGAZY G, MASSOUD AH, SEDDIK M, et al. Structural Versus Nonstructural Bone Grafting for the Treatment of Unstable Scaphoid Waist Nonunion Without Avascular Necrosis: A Randomized Clinical Trial. J Hand Surg. 2021;46(6):462-470. [26] SAYEGH ET, STRAUCH RJ. Graft choice in the management of unstable scaphoid nonunion: a systematic review. J Hand Surg. 2014;39(8):1500-1506.e7. [27] KIM JY, LEE SL, PARK SY, et al. A Comparison of Non-vascularized Bone Grafting and Internal Fixation in the Treatment of Unstable Scaphoid Waist Nonunion. J Hand Surg Asian. 2021;26(4):697-704. [28] SEVERO AL, LEMOS MB, LECH OLC, et al. Bone graft in the treatment of nonunion of the scaphoid with necrosis of the proximal pole: a literature review. Rev Bras Ortop. 2017;52(6):638-643. [29] TAMBE AD, CUTLER L, MURALI SR, et al. In scaphoid non-union, does the source of graft affect outcome? Iliac crest versus distal end of radius bone graft. J Hand Surg (Edinburgh, Scotland). 2006;31(1):47-51. [30] DUNCUMB JW, ROBINSON PG, WILLIAMSON TR, et al. Bone grafting for scaphoid nonunion surgery : a systematic review and meta-analysis. Bone Joint J. 2022; 104-b(5):549-558. [31] SHIN SC, KIM NY, KANG HJ, et al. Comparison of corticocancellous bone graft from the anterolateral metaphysis of the distal radius versus iliac crest for the treatment of unstable scaphoid nonunion with humpback deformity. BMC musculoskelet Disord. 2024;25(1):20. [32] TESTA G, LUCENTI L, D’AMATO S, et al. Comparison between Vascular and Non-Vascular Bone Grafting in Scaphoid Nonunion: A Systematic Review. J Clin Med. 2022;11(12):3402. [33] 刘建寅, 郭强, 王丹,等. 桡动脉茎突返支为蒂桡骨茎突骨瓣植入术治疗舟骨骨折不愈合[J]. 中华创伤骨科杂志,2004(4): 48-50. [34] MOHIUDDIN M, DAS BK, MANZUR RM, et al. The Outcome of Scaphoid Fracture Nonunion Managed by 1,2 Intercompartmental Supraretinacular Artery (1,2 ICSRA) Vascularized Bone Graft. Cureus. 2023;15(10):e47489. [35] 王成琪, 张永亮,任志勇,等. 带蒂的桡骨筋膜瓣移植治疗陈旧性舟状骨骨折[J].解放军医学杂志,1987(3):225. [36] 田光磊. 用于舟骨骨折的桡骨瓣及其血管[J]. 中华手外科杂志,2007,23(6):321-326. [37] ZAIDEMBERG C, SIEBERT JW, ANGRIGIANI C. A new vascularized bone graft for scaphoid nonunion. J Hand Surg. 1991;16(3):474-478. [38] SHEETZ KK, BISHOP AT, BERGER RA. The arterial blood supply of the distal radius and ulna and its potential use in vascularized pedicled bone grafts. J Hand Surg. 1995; 20(6):902-914. [39] ÇOLAK I, AKGÜN E, KILIÇ Z, et al. Vascularized Bone Grafting in the Treatment of Scaphoid Nonunion: A Clinical and Functional Outcome Study. J Wrist Surg. 2022;11(4):288-294. [40] 邢志利, 孙捷, 诸葛天瑜, 等. 桡动脉茎突返支骨瓣移位治疗舟状骨不连[J]. 中国骨伤,2010,23(2):147-149. [41] 李宏维, 吴卓, 王栓科. 手术治疗腕舟状骨骨折不愈合的研究进展[J]. 中国矫形外科杂志,2014,22(24):2261-2263. [42] BRAUN RJOT. Pronator pedicle bone grafting n the forearm and proximal carpal row. 1983;7:35. [43] KAPOOR S, PAWAR I, KAPOOR S. Posttraumatic osteonecrosis and nonunion of distal pole of scaphoid. Indian J Orthop. 2013;47(4):425-428. [44] LEE SK, PARK JS, CHOY WS. Scaphoid fracture nonunion treated with pronator quadratus pedicled vascularized bone graft and headless compression screw. Annals of plastic surgery. 2015;74(6):665-671. [45] ÖZDEMIR MA, BAYRAM S, AYIK Ö, et al. Comparison of clinical outcomes of autologous bone graft versus pronator quadratus pedicled vascularized bone graft in the treatment of scaphoid nonunion. Acta orthopaedica Belgica. 2022;88(3): 447-455. [46] 马玉林, 夏宁晓, 郭建斌,等. 带血管蒂第二、三掌骨骨瓣转移治疗腕舟骨陈旧性骨折[J]. 中华手外科杂志,1996(S1): 22-23. [47] SAWAIZUMI T, NANNO M, NANBU A, et al. Vascularised bone graft from the base of the second metacarpal for refractory nonunion of the scaphoid. J Bone Joint Surg Br. 2004;86(7):1007-1012. [48] 周家顺. 股骨内髁游离骨瓣治疗腕舟骨近侧骨折块坏死[J].实用手外科杂志, 2023,37(4):475-478+490. [49] KORIEM I, AGINA AA, EL GHAZAWY AK. Treatment of failed scaphoid nonunion fixation using free medial femoral condyle vascularized bone grafting. SICOT J. 2023; 9:7. [50] ZHOU KJ, GRAHAM DJ, STEWART D, et al. Free Medial Femoral Condyle Flap for Reconstruction of Scaphoid Nonunion: A Systematic Review. J Reconstr Microsurg. 2022;38(8):593-603. [51] HARPF C, GABL M, REINHART C, et al. Small free vascularized iliac crest bone grafts in reconstruction of the scaphoid bone: a retrospective study in 60 cases. Plast Reconstr Surg. 2001;108(3): 664-674. [52] 邹阳平, 张树新, 张小平, 等. 吻合血管游离髂骨瓣治疗陈旧性舟骨骨折[J].深圳中西医结合杂志, 2019,29(23): 128-129. [53] 彭亚静,张奕华,高婷婷. 疲劳和营养不良对腕舟状骨骨折不愈合术后恢复的影响[J]. 局解手术学杂志,2024,33(4): 330-334. [54] 何智灵,王超,何斌,等. 高压氧联合桡骨瓣治疗腕舟状骨骨折不愈合的临床疗效[J]. 中国骨与关节损伤杂志,2024, 39(3):315-317. |
| [1] | Liu Jinlong, Abuduwupuer·Haibier, Bai Zhen, Su Danyang, Miao Xin, Li Fei, Yang Xiaopeng. Efficacy of different nonsurgical treatments for adolescent idiopathic scoliosis: a systematic review and network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2370-2379. |
| [2] | Xinjiang Branch of China Trauma Rescue & Treatment Association. Expert consensus on diagnosis and treatment of brucellar osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2403-2412. |
| [3] | Li Qingbin, Lin Jianhui, Huang Wenjie, Wang Mingshuang, Du Jiankai, Lao Yongqiang. Bone cement filling after enlarged curettage of giant cell tumor around the knee joint: a comparison of subchondral bone grafting and non-grafting [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 1896-1902. |
| [4] | Xu Shencong, Fang Zifei, Ji Mingyi, Xu Chengrui, Li Binhong, Cao Jiayu, Xu Junfeng. Application of Onlay bone grafts from mandibular lateral oblique line in implant restoration of bone defects in upper anterior teeth [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(4): 841-848. |
| [5] | Jia Yingao, Gao Shitao, Wang Fei. Application of 3D printed titanium cage cutting model in anterior cervical vertebrae subtotal decompression and bone graft fusion [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(3): 604-611. |
| [6] | Guan Mingqiang, Wei Jinqiang, Chen Weijian, Zhou Guanming. Reconstruction of bone defect at the top of acetabulum during revision total hip arthroplasty with cup blocking screws and impaction bone grafting [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(15): 3878-3884. |
| [7] | Wang Jingyi, An Shuai, Li Daoqin, He Tao, Feng Mingli, La Gaoyan, Li Zheng, Cheng Jingbo. Stepwise surgical treatment of knee osteoarthritis and the application trends of three surgical procedures: a bibliometric analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(15): 4010-4020. |
| [8] | Cai Yaohao, Lang Lyu, Li Hong. Assessing the bone mass of the residual alveolar ridge in the first molar for implant placement by cone-beam computed tomography [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(8): 1572-1577. |
| [9] | Liu Haoyang, Xie Qiang, Shen Mengran, Ren Yansong, Ma Jinhui, Wang Bailiang, Yue Debo, Wang Weiguo . Application, research hotspots, and shortcomings of degradable zinc-based alloys in bone defect repair and reconstruction [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(4): 839-845. |
| [10] | Akliya·Anwar, Nafisa·Gupur, Baibugafu·Yelisi, Zilalai·Gulaiti, Guzalnur·Emrayim, Nijat·Tursun. Dynamic stress analysis of maxillary sinus lifting without bone grafting and with immediate loading after bone grafting [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(30): 6416-6425. |
| [11] | Lu Yuzheng, Xiong Yingjie, Shan Yanbo, Ye Jianting, Wu Yanbin, Song Jipeng, Zhang Yao, Lin Wancheng, Weng Qirui, Cheng Xuan, Meng Haoye, Xu Wenjing, Peng Jiang, Ding Lixiang. Effect of silicate bioactive glass fiber on properties of calcium phosphate bone cement [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(28): 5994-6002. |
| [12] | Liu Zilue, Wang Zhi, Song Wenshang, Li Suna, Cai Shixin. Autogenous bone and platelet-rich fibrin in repair of severe alveolar bone defects [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(10): 2044-2051. |
| [13] | Chen Kaijia, Liu Jingyun, Cao Ning, Sun Jianbo, Zhou Yan, Mei Jianguo, Ren Qiang. Application and prospect of tissue engineering in treatment of osteonecrosis of the femoral head [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(9): 1450-1456. |
| [14] | Zhong Jun, Wang Wen. Network meta-analysis of different anatomical repair strategies to improve chronic lateral ankle instability [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(9): 1470-1476. |
| [15] | Sun Houjie, Han Jianhua, Cai Xiaojun, Li Daijun, Fan Rui. Subcutaneous endplate bone graft reduction combined with percutaneous pedicle screw fixation for A3+B2 thoracolumbar burst fractures [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(33): 5357-5363. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||