中国组织工程研究 ›› 2013, Vol. 17 ›› Issue (48): 8429-8436.doi: 10.3969/j.issn.2095-4344.2013.48.021
• 骨与关节临床实践 clinical practice of the bone and joint • 上一篇 下一篇
老年骨质疏松性髋部骨折的优化治疗方案
陈 鹏1,刘文和2,颜林淋3,郭志文1,唐新文1,胡伟文1,曹锡文1,王福剑1,李 杨1,陈家玉4
- 湘南学院附属医院,1骨科,3超声诊断室,湖南省郴州市 423000;2暨南大学医学院附属清远人民医院骨科二区,广东省清远市 511518;4湘南学院临床医学系,湖南省郴州市 423000
-
出版日期:2013-11-26发布日期:2013-11-26 -
通讯作者:陈家玉,主任医师,教授,硕士生导师,湘南学院临床医学系, 湖南省郴州市 423000 -
作者简介:陈鹏★,男,1981年生,湖南省耒阳市人,汉族,2009年南华大学毕业,硕士,主治医师,主要从事骨与关节损伤的基础与临床研究。 -
基金资助:湖南省科技厅立项支助项目(2012TP4021-4)*;郴州市科技局立项支助项目(2012CT116)*
Optimized surgical treatment for osteoporotic hip fractures in the elderly
Chen Peng1, Liu Wen-he2, Yan Lin-lin3, Guo Zhi-wen1, Tang Xin-wen1, Hu Wei-wen1, Cao Xi-wen1, Wang Fu-jian1, Li Yang1, Chen Jia-yu4
- 1 Department of Orthopedics, Affiliated Hospital of Xiangnan University, Chenzhou 423000, Hunan Province, China
2 Department of Orthopedics, People’s Hospital of Qingyuan, Medical College of Jinan University, Qingyuan 511518, Guangdong Province, China
3 Department of Ultrasonography Diagnosis, Affiliated Hospital of Xiangnan University, Chenzhou 423000, Hunan Province, China
4 Department of Clinical Medicine, Xiangnan University, Chenzhou 423000, Hunan Province, China
-
Online:2013-11-26Published:2013-11-26 -
Contact:Chen Jia-yu, Chief physician, Professor, Master’s supervisor, Department of Clinical Medicine, Xiangnan University, Chenzhou 423000, Hunan Province, China iudoct@126.com -
About author:Chen Peng★, Master, Attending physician, Department of Orthopedics, Affiliated Hospital of Xiangnan University, Chenzhou 423000, Hunan Province, China 198122741@163.com -
Supported by:the Supportive Program of Hunan Provincial Science and Technology Bureau, No. 2012TP4021-4*; the grant from the Science and Technology Department of Chenzhou City, No. 2012CT116*
摘要:
背景:目前国内外学者对于老年性髋部骨折越来趋向于积极的手术治疗。手术治疗首先要根据不同骨折部位、骨折类型、不同年龄和是否合并有内科基础疾病从而选择不同的固定方式,对于老年性髋部骨折治疗的成败起到非常重要的作用。 目的:探讨老年骨质疏松性髋部骨折的优化治疗方案。 方法:2000年1月至2012年1月根据具体情况采用不同方法治疗老年骨质疏松性髋部骨折176例,年龄(76.7±6.3)岁。股骨转子间骨折84例,其中保守治疗7例,动力髋螺钉内固定34例,空心加压螺钉固定18例,解剖钢板内固定7例,人工股骨头置换12例,人工全髋关节置换6例。股骨颈骨折92例,其中双极人工股骨头置换40例,人工全髋关节置换37例,空心加压螺钉固定15例。不同治疗方法的治疗效果按Harris髋关节功能评分标准评定,并观察患者并发症发生情况。 结果与结论:股骨转子间骨折76例,股骨颈骨折85例获随访,随访时间8-26个月。内固定治疗的平均愈合时间为(5.7±1.3)个月。3例发生治疗后感染,1例治疗后10 d并发心肺功能衰竭死亡。不同治疗方法的并发症包括股骨头切割、围术期骨折,内固定或假体松动、术后骨折、股骨头缺血坏死、髋内翻、下肢短缩、骨折延期愈合及对髋再骨折等。双极人工股骨头置换与人工全髋关节置换患者的并发症发生率显著低于保守治疗、空心加压螺钉、解剖钢板及动力髋螺钉置入内固定患者(P < 0.05)。双极人工股骨头置换与人工全髋关节置换患者的Harris评分优良率显著高于保守治疗、空心加压螺钉、解剖钢板及动力髋螺钉置入内固定患者(P < 0.05)。而保守治疗、空心加压螺钉、解剖钢板及动力髋螺钉置入内固定患者相互之间的并发症发生率、Harris评分优良率比较,双极人工股骨头置换与人工全髋关节置换患者的并发症发生率、Harris评分优良率比较,差异无显著性意义(P > 0.05),提示老年骨质疏松性髋部骨折需要积极的综合治疗,对于高龄股骨颈骨折患者最好采用双极人工股骨头置换或人工全髋关节置换治疗为宜。
中图分类号:
引用本文
陈 鹏,刘文和,颜林淋,郭志文,唐新文,胡伟文,曹锡文,王福剑,李 杨,陈家玉. 老年骨质疏松性髋部骨折的优化治疗方案[J]. 中国组织工程研究, 2013, 17(48): 8429-8436.
Chen Peng, Liu Wen-he, Yan Lin-lin, Guo Zhi-wen, Tang Xin-wen, Hu Wei-wen, Cao Xi-wen, Wang Fu-jian, Li Yang, Chen Jia-yu. Optimized surgical treatment for osteoporotic hip fractures in the elderly[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(48): 8429-8436.
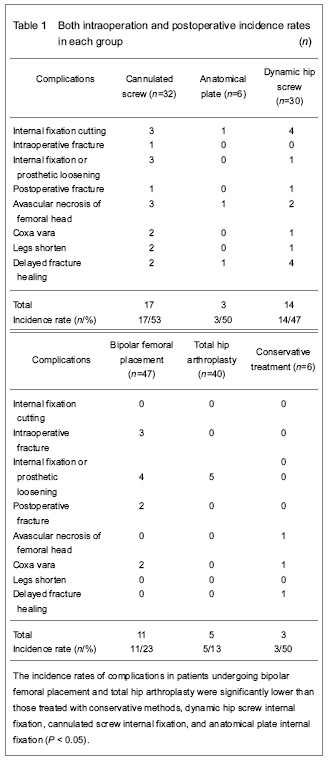
Both intraoperation and postoperative complications included femoral head cutting, intraoperative fracture, internal fixation and prosthetic loosening, postoperative fracture, avascular necrosis of femoral head, coxa vara, legs shorten, delayed fracture healing, contralateral hip re-fracture. The incidence rates of complications in patients undergoing bipolar femoral placement and total hip arthroplasty were significantly lower than those treated with conservative methods, dynamic hip screw internal fixation, cannulated screw internal fixation, and anatomical plate internal fixation (P < 0.05). No significant differences were found in the incidence rate of complications among patients treated with conservative methods, dynamic hip screw internal fixation, cannulated screw internal fixation, and anatomical plate internal fixation (P > 0.05). There was also no significant difference in the incidence rate of complications between patients treated with bipolar femoral placement and total hip arthroplasty (P > 0.05; Table 1).
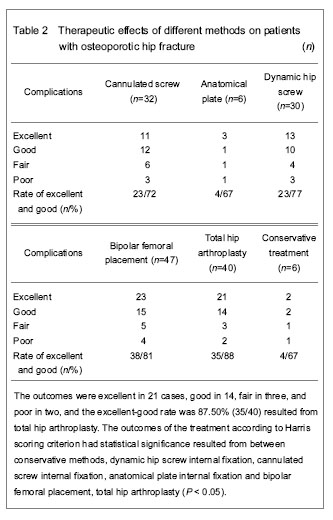
The data are detailed in Table 2.
| [1] Liu J. The comparison of different treatment method of internal fixation on inertrochanter fracture of femur. Zhongguo Xiandai Yixue Zazhi. 2011;21(19):2283-2285. [2] Liu ZH. Bone Mineral and Clinical M. Beijing: China Science and Technology Press, 2006:446-460. [3] Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51(4):737-755. [4] Napoli N, Schwartz AV, Palermo L, et al. Risk factors for subtrochanteric and diaphyseal fractures: the study of osteoporotic fractures. J Clin Endocrinol Metab. 2013; 98(2):659-667. [5] Kung AW, Fan T, Xu L, et al. Factors influencing diagnosis and treatment of osteoporosis after a fragility fracture among postmenopausal women in Asian countries: a retrospective study. BMC Womens Health. 2013;13(1):7-15. [6] Briongos L, Sañudo S, García-Alonso M, et al. Treatment of osteoporosis and hip fractures in a Spanish health area. Eur Rev Med Pharmacol Sci. 2013;17(2):266-268. [7] Chen P, Liu WH, Yan LL, et al. Treatment of osteoporotic hip fracture in the elder. Zhongguo Linchuang Xinyixue. 2012;5(5):410-412. [8] Said GZ, Farouk O, El-Sayed A, et al. Salvage of failed dynamic hip screw fixation of intertrochanteric fractures. Injury. 2006;37(2):194-202. [9] Zhang C, Wang PJ, Ruan DK, et al. Complications of surgical treatment for femoral intertrochanteric fractures using dynamic hip screw. Zhongguo Gushang. 2009;22(8): 624-626. [10] Huo JJ, Zhao Y, Tian H, et al. Systematic review on gamma nails versus dynamic hip screws and plate for intertrochanteric fractures of femur in elder. Zhongguo Xiandai Yixue Zazhi. 2011;21(7):773-778. [11] Jewell DP, Gheduzzi S, Mitchell MS, et al. Locking plates increase the strength of dynamic hip screws. Injury. 2008; 39(2):209-212. [12] Zheng HG, Tang H, Zhang QL. A comparative study of dynamic hip screw and proximal femoral nail an tirotation in treatment of femoral in tertrochan tericfractures. Zhongguo Jiaoxing Waike Zazhi. 2009;17(6):407-408. [13] Al-Ani AN, Samuelsson B, Tidermark J, et al. Early operation on patients with a hip fracture improved the ability to return to independent living: A prospective study of 850 patients. J Bone Joint Surg Am. 2008;90(7):1436-1442. [14] Efstathopoulos NE, Nikolaou VS, Lazarettos JT. Intramedullary fixation of intertrochanteric hip fractures: a comparison of two implant designs. Int Orthop. 2007;1: 71-76. [15] Parker MJ, White A, Boyle A. Fixation versus hemiarthroplasty for undisplaced intracapsular hip fractures. Injury. 2008;39(7):791-795. [16] Cui FG, Cong J, Li GS. Treatment of unstable femoral intertrochanteric fracture with dynamic hip screw. Zhongguo Jiaoxing Waike Zazhi. 2008;16(6):471-472. [17] Leonardsson O, Sernbo I, Carlsson A, et al. Long-term follow-up of replacement compared with internal fixation for displaced femoral neck fractures: results at ten years in a randomised study of 450 patients. J Bone Joint Surg Br. 2010;92(3):406-412. [18] Li SF. The comparison between different treatment on femoral intertrochanteric fractures by dynamic condylus screw and dynamic hip screw. Zhongyiyao Daobao. 2008; 14(5):63-65. [19] Gao H. Clinical outcome of femoral head replacement for femoral intertrochanteric fractures or femoral neck fractures in patients over 70 years old. Zhongguo Zuzhi Gongcheng Yanjiu yu Linchuang Kangfu. 2008;12(35):6879-6882. [20] Frihagen F, Nordsletten L, Madsen JE. Hemiarthroplasty or internal fixation for intracapsular displaced femoral neck fractures: randomised controlled trial. BMJ. 2007;335 (7632):1251-1254. [21] Guan CY, Chang Q, Ma YZ, et al. Treatment of senile patients with unstable femoral intertrochanteric fracture:comparison between hemiprosthesis arthoplasty and internal fixation. Zhongguo Gu yu Guanjie Sunshang Zazhi. 2008;23(12):975. [22] Faldini G, Grandi G, Romagnoli M, et al. Surgical treatment of unstable intertrochanteric fractures by bipolar hip replacement or total hip replacement in elderly osteoporotic patients. J Orthop Trauma. 2006;7(3):117-121. [23] Gu GS, Wang G, Sun DH, et al. Cemented bipolar hemiarthroplasty with a novel cerclage cable technique for unstable intertrochanteric hip fractures in senile patients. Chin J Traumatol. 2008;11(1):13-17. [24] Hsu CJ, Chou WY, Chiou CP, et al. Hemi-arthroplasty with supplemental fixation of greater trochanter to treat failed hip screws of femoral intertrochanteric fracture. Arch Orthop Trauma Surg. 2008;128(8):841-845. [25] Ho M, Garau G, Walley G, et al. Minimally invasive dynamic hip screw for fixation of hip fractures. Int Orthop. 2009;33(2): 555-560. [26] Zhang S, Kong CG, Chen WY, et al. Osteoporotic hip fracture: Comparison on various treatments of metal implants. Zhongguo Zuzhi Gongcheng Yanjiu yu Linchuang Kangfu. 2010;14(22):4176-4180. [27] Chen JS, Zheng Q, Li H. Comparison of dynamic hip screw and proximal femoral nail for treating intertrochanteric fractures in elderly patients. Zhejiang Yixue. 2008;30(1): 49-51. [28] Hammad A, Abdel-Aal A, Said HG, et al. Total hip arthroplasty following failure of dynamic hip screw fixation of fractures of the proximal femur. Acta Orthop Belg. 2008; 74(6):788-792. [29] Hsu CJ, Chou WY, Chiou CP, et al. Hemi-arthroplasty with supplemental fixation of greater trochanter to treat failed hip screws of femoral intertrochanteric fracture. Arch Orthop Trauma Surg. 2008;128(8):841-845. [30] Faldini G, Grandi G, Romagnoli M, et al. Surgical treatment of unstable intertrochanteric fractures by bipolar hip replacement or total hip replacement in elderly osteoporotic patients. J Orthop Trauma. 2006;7(3):117-121. [31] Wang CH, Ma ZX, Bi LF. Analysis on osteoporosis diagnosis and treatment of 986 elderly inpatients with hip fracture. Zhongguo Guzhi Shusong Zazhi. 2010;16(5): 353-355. |
| [1] | 李啸群, 徐凯航, 纪 方. 补骨脂异黄酮抑制破骨细胞分化缓解小鼠去卵巢骨质疏松[J]. 中国组织工程研究, 2020, 24(在线): 4-. |
| [2] | 赵维彪, 何子微, 李 季, 李 毅. 3D打印导板在以SuperPATH技术行老年髋关节置换中的应用价值:回顾性研究和文献检索证据分析[J]. 中国组织工程研究, 2020, 24(9): 1324-1330. |
| [3] | 周 祺, 高 益, 魏 康, 黎 俊, 徐建达, 蒋 阳, 瞿玉兴. 全膝关节置换治疗类风湿关节炎:关节功能及相关生化指标的变化[J]. 中国组织工程研究, 2020, 24(9): 1337-1341. |
| [4] | 余 彬, 彭银虓, 薛 力, 秦 辉, 梁益建. 零切迹椎间融合固定器与传统颈前路钢板Cage融合内固定治疗双节段颈椎病的比较[J]. 中国组织工程研究, 2020, 24(9): 1342-1347. |
| [5] | 葛 苏, 邹小宝, 马向阳, 王宾宾, 杨浩志, 张 双, 倪 菱, 陈育岳, 夏 虹, 吴增晖. 枢椎支点螺钉设计与其在寰枢椎脱位修复中的应用[J]. 中国组织工程研究, 2020, 24(9): 1348-1352. |
| [6] | 刘 炎, 葛鸿庆, 管 华, 陈文治. 内侧柱缺失型肱骨近端骨折不同固定方式的有限元分析[J]. 中国组织工程研究, 2020, 24(9): 1384-1389. |
| [7] | 林 旺, 王盈盈, 林伟民, 许胜贵, 黄其龙, 郭卫中, 林成寿. 新型胸锁关节钩状板的研发与生物力学测定[J]. 中国组织工程研究, 2020, 24(9): 1395-1399. |
| [8] | 钟远鸣, 罗 满, 唐福波, 唐 成. 骨质疏松性胸腰椎骨折MRI STIR黑色线性信号与外力程度的关系[J]. 中国组织工程研究, 2020, 24(9): 1400-1404. |
| [9] | 曹旭含, 白子兴, 孙承颐, 李晏乐, 孙卫东. 机器人在骨科手术中应用的可靠性与提升空间[J]. 中国组织工程研究, 2020, 24(9): 1416-1421. |
| [10] | 程才统, 韩鹏飞, 武太勇, 李 健, 付海军, 王羽姗, 冯 毅. 关节置换与切开复位内固定治疗桡骨头骨折的Meta分析[J]. 中国组织工程研究, 2020, 24(9): 1457-1463. |
| [11] | 邓锦满, 方冠军, 汪 宇, 丁少波 . 系统评价帕瑞昔布和塞来昔布治疗骨科手术后疼痛的效果及特点[J]. 中国组织工程研究, 2020, 24(9): 1471-1476. |
| [12] | 申洪全, 陆 慧, 张孝华, 郭金伟, 杨博文, 余路鑫, 朱 明. 计算机辅助2枚空心钉置入内固定治疗股骨颈骨折的生物力学分析[J]. 中国组织工程研究, 2020, 24(6): 882-887. |
| [13] | 汪 亮, 黄朝朝, 于娇娜, 顾卫东, 王 忍, 钱志艺. 桥接系统混棒与双棒结构治疗股骨及胫骨骨折的生物力学特点[J]. 中国组织工程研究, 2020, 24(6): 888-892. |
| [14] | 郭天庆, 薛 飞, 冯 卫. 股骨转子间骨折不同外侧壁分型的内固定治疗策略[J]. 中国组织工程研究, 2020, 24(6): 917-923. |
| [15] | 陈锦涛, 韩树峰.
髓内钉与锁定钢板固定治疗肱骨近端骨折的Meta分析 |
1 老年性髋部骨折主要是指股骨转子间骨折和股骨颈骨折,骨折后丧失站立行走动能力,容易影响老年人的生活质量甚至缩短生存期。同时老年患者多存在不同程度的骨质疏松,骨折后卧床容易出现静脉血栓、肺部感染、压疮、尿路感染、不全性肠梗阻等严重并发症。 2 老年骨质疏松性髋部骨折治疗不当可引起畸形愈合或骨折不愈合等并发症,影响患肢功能,所以治疗方法不同对临床疗效有很大的影响。文章特点在于老年骨质疏松性髋部骨折的优化治疗方案。 3 结果显示,对于老年骨质疏松性髋部骨折治疗必须个体化,但总的治疗原则和目的是一致的,即在积极控制基础疾病的同时,选择合理的治疗手段,防止并发症的发生,恢复原有功能,提高生活质量。对于高龄股骨颈骨折患者采用双极人工股骨头置换或人工全髋关节置换治疗为宜。 基金资助: 湖南省科技厅立项支助项目(2012TP4021-4)*;郴州市科技局立项支助项目(2012CT116)*
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||