Chinese Journal of Tissue Engineering Research ›› 2013, Vol. 17 ›› Issue (13): 2431-2438.doi: 10.3969/j.issn.2095-4344.2013.13.021
Previous Articles Next Articles
Three-dimensional image reconstruction for elbow fractures
Lu Hao-ning, Pan Shi-nong
- Shengjing Hospital of China Medical University, Shenyang 110004, Liaoning Province, China
-
Received:2012-10-15Revised:2013-01-26Online:2013-03-26Published:2013-03-26 -
Contact:Pan Shi-nong, Doctor, Professor, Master’s supervisor, Shengjing Hospital of China Medical University, Shenyang 110004, Liaoning Province, China panshinong@vip.163.com -
About author:Lu Hao-ning★, Studying for master’s degree, Shengjing Hospital of China Medical University, Shenyang 110004, Liaoning Province, China luhaoning1985@126.com
CLC Number:
Cite this article
Lu Hao-ning, Pan Shi-nong. Three-dimensional image reconstruction for elbow fractures[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(13): 2431-2438.
share this article

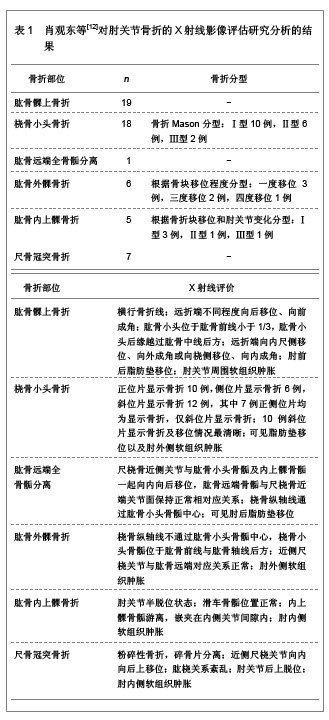
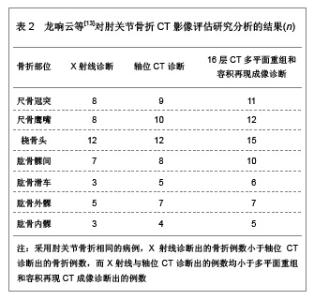
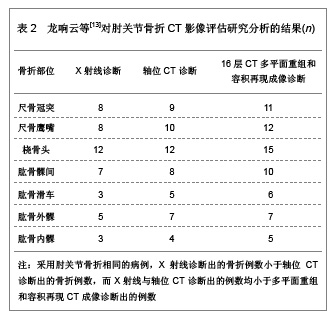
2.1 X射线在肘关节骨折评估中的应用 X射线是由德国物理学家伦琴首先发现,随后被广泛应用于医学各个领域,随着人们认识的深入以及医学技术的不断发展,X射线目前已经成为骨关节创伤最常用的检查诊断方法。X射线摄片简单、方便,是骨关节创伤首选的检查诊断方法。X射线可以显示肘关节创伤尤其是肘关节骨折中的病变,肖观东等[12]对肘关节骨折时各种类型骨折的X射线影像评价进行了研究分析,具体结果见表1。 2.2 CT在肘关节骨折评估中的应用 CT扫面成像快速、清晰,能够发现微小的骨质变化或X射线平片互相重叠而遮盖的骨折线。此外,CT扫描能够更立体直观的显示肘关节各骨骨折线的走形、移位情况、碎骨片的数量、来源、关节受累情况等,在肘关节骨折的影像学诊断中具有不可替代的作用。龙响云等[13]对CT影像评价肘关节骨折的准确性进行了分析,以X射线平片诊断为对照参考,对轴位CT影像与16层CT多平面重组和容积再现成像诊断的准确性进行了评估,结果显示16层CT多平面重组和容积再现成像对肘关节骨折诊断的例数多于轴位CT诊断例数,并且明显多于X射线诊断的肘关节骨折例数,具体结果见表2。"
"
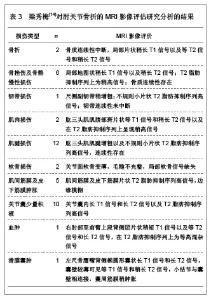
2.3 MRI在肘关节骨折评估中的应用 梁秀梅[14]对肘关节骨折以及周围软组织损伤的MRI影像评价进行了研究分析,具体结果见表3。"
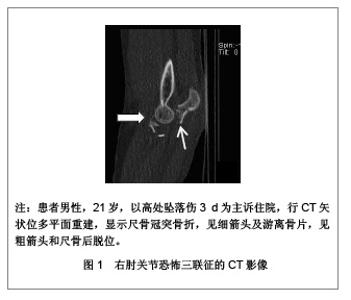
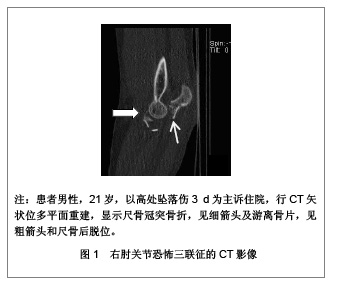
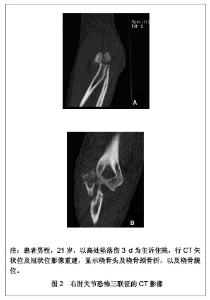
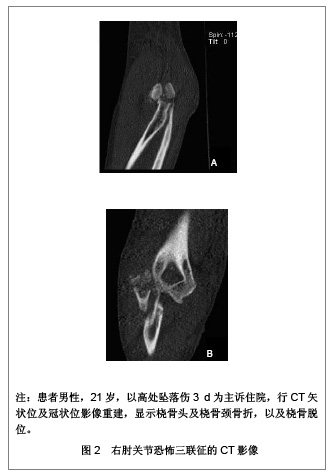
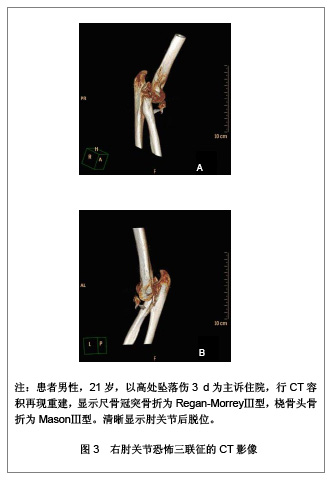
MRI影像对于肘关节的轻微创伤如骨挫伤以及周围软组织损伤具有良好的评估价值,能够明确显示肘关节周围韧带、肌肉以及肌腱组织等的损伤情况,是一种无创伤且有效的检查方法。肘关节内外侧副韧带是维持肘关节内侧和外侧稳固性的主要因素,其中外侧尺副韧带和内侧前束更为重要,在冠状位MRI图像中,正常内外侧副韧带均表现为薄的跨关节条状低信号影像,分别位于屈肌腱和伸肌腱的下方。由此可见MRI在肘关节创伤的影像诊断中发挥重要的作用。 2.4 肘关节“恐怖三联征”的影像学研究 病例:患者男性,21岁,以高处坠落伤3 d为主诉住院。 患者3 d前因意外从3楼(约9 m)高处坠落,自觉右肘疼痛,腰疼,骨盆疼,双髋疼。查体:右肘关节肿胀畸形,压痛阳性,轴向叩击痛阳性,可闻及骨擦音,触及骨擦感,有反常活动。右肘关节盂空虚,尺骨鹰嘴向后突出,肘后三角位置改变,肘外翻挤压实验阳性。 病例应用Philips Brilliance 64层CT检查。设置扫描参数120 kV,118 mA。层厚1 mm,螺距0.5。采用Philips Brilliance Workspace Portal工作站进行图像后处理,重建参数,层厚1 mm,层间隔1 mm。 右肘关节平扫及三维重建影像显示:右肘关节变形,右尺、桡骨向后上方移位。右尺骨冠突多发骨质断裂,断端分离,游离冠突碎骨片大于50%冠突高度,符合Regan-MorreyⅢ型骨折。右桡骨头及桡骨颈骨质断裂,桡骨头游离,其内见多发透亮线影,右桡骨头、干分离,且桡骨头粉碎性骨折,符合MasonⅢ型骨折。右肘关节软组织肿胀。X射线及CT影像显示见图1-5。"
"

"

影像学诊断:右肘关节恐怖三联征,右肘关节后脱位合并右桡骨小头粉碎性骨折(MasonⅢ型)以及右尺骨冠突粉碎性骨折(Regan-MorreyⅢ型)。 行“右肘关节骨折切开复位内固定”,内固定操作中发现桡骨小头粉碎骨折,桡骨颈处骨质压缩,冠状突粉碎骨折。复位冠状突,复位桡骨小头,修复肘关节外侧韧带。 肘关节“恐怖三联征”是Hotchkiss[15]于1996年首次命名,即肘关节后脱位同时伴有尺骨冠突骨折和挠骨头骨折。由于肘关节“恐怖三联征”属于复杂不稳定、高能量的肘部创伤,临床治疗较为困难,由此引起的关节不稳定、创伤性关节炎及关节僵硬、异位骨化等并发症常导致患者预后不良。 Ring等[16]和Pugh等[17]进一步对此类损伤进行了研究与报道。“恐怖三联征”多见于坠落伤及车祸,是肘部严重的高能量创伤。最常见的损伤机制为肘关节在伸直位,遭受纵轴方向的高能量压缩剪切暴力造成[18]。主要损伤包括肘关节后脱位,桡骨头骨折,冠突骨折,双侧副韧带撕裂,前关节囊撕裂等。目前认为尺骨冠突和内外侧副韧带是肘关节稳定的第一列因素,桡骨头、关节囊和屈肌、伸肌起点是第二列因素[19]。因此,肘关节“恐怖三联征”的尺骨冠突及桡骨头骨折以及侧副韧带损伤能够导致肘关节极度不稳定。 临床常用Regan-Morrey分类法评价冠突骨折:冠突尖部骨折为Ⅰ型,冠突骨折块高度小于冠突高度的50%为Ⅱ型,冠突骨折块高度大于或等于冠突高度的50%为Ⅲ型[20]。其中冠突高度指尺骨冠突尖至滑车最低点的垂直距离,即经鹰嘴尖作一与尺骨干平行的直线,该直线即为冠突高度50%的分界线。用Mason[21]分类法评价桡骨头骨折:桡骨头无移位性骨折为Ⅰ型,桡骨头骨折伴分离移位,但仍有部分桡骨头与骨干相连为Ⅱ型,桡骨头粉碎性骨折,头与骨干分离为Ⅲ型。之后Johnston将Mason法改良,把桡骨头骨折伴肘关节后脱位增加为第Ⅳ型,因此对于肘关节“恐怖三联征”,所有桡骨头骨折均为Johnston改良后的第Ⅳ型。文章病例右尺骨冠突骨折属于Regan-Morrey分类Ⅲ型,右桡骨头骨折属于Mason分类Ⅲ型,属于Johnston改良后的第Ⅳ型。"

| [1] 王云钊.中华影像医学:骨肌系统卷[M].北京:人民卫生出版社, 2002:128.[2] 陈明祥,邰学祥,陈娟,等.螺旋CT多平面和三维重建在肘关节骨折中的诊断价值[J].实用放射学杂志,2007,23(5):656-657.[3] 李德龙,刘斯平,王振波.16层MSCT不同重建方法在骨与关节疾病诊断中的应用价值研究[J].中国中西医结合影像学杂志,2007, 5(2):106-109.[4] Mulkens TH, Bellinck P, Baeyaert M, et al. Use of an automatic exposure control mechanism for dose optimization in multi-detector row CT examinations: clinical evaluation. Radiology. 2005;237(1):213-223.[5] van Riet RP, Bain GI, Baird R, et al. Simultaneous reconstruction of medial and lateral elbow ligaments for instability using a circumferential graft. Tech Hand Up Extrem Surg. 2006;10(4):239-244.[6] Haapamäki VV, Kiuru MJ, Mustonen AO, et al. Multidetector computed tomography in acute joint fractures. Acta Radiol. 2005;46(6):587-598.[7] Wodecki P, Maiza D, Rozenblum B. Elbow dislocation in children associated with proximal radioulnar translocation. Rev Chir Orthop Reparatrice Appar Mot. 2007;93(2):190-194.[8] 扈延龄,裴国献,李旭,等.三维CT重建对关节内骨折分型术前评价的影响[J].中国矫形外科杂志,2008,16(8):568-570.[9] 何强.MSCT重建技术在肘关节创伤性骨折中的应用[J].实用临床医药杂志,2012,16(13):65-66.[10] 栗占国.类风湿关节炎[M].北京:人民卫生出版社,2009:149.[11] 中国知网.中国学术期刊总库[DB/OL].2013-1-10. https://www.cnki.net[12] 肖观东,周长元,郑超,等.肘关节骨折56例数字化X线摄影分析[J].广东医学,2011,32(6):780-782.[13] 龙响云,方向军,罗祖孝,等.16层螺旋CT多平面重组和容积再现对肘关节损伤的诊断价值[J].重庆医科大学学报,2011,36(8): 985-987.[14] 梁秀梅.MRI对22例肘关节病变的诊断价值[J].重庆医学,2012, 41(10):993-996.[15] Hotchkiss RN. Fractures and dislocations of the elbow. In: Rockwood CA, Green DP, Bucholz RW, et al. Rockwood and Green's fractures in adults. 4th ed.Volume 1. Philadelphia: Lippincott-Raven,1996:929-1024.[16] Ring D, Jupiter JB, Zilberfarb J. Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am. 2002;84-A(4):547-551.[17] Pugh DM, McKee MD. The "terrible triad" of the elbow. Tech Hand Up Extrem Surg. 2002;6(1):21-29.[18] Amis AA, Miller JH. The mechanisms of elbow fractures: an investigation using impact tests in vitro. Injury. 1995;26(3): 163-168.[19] 张世民.肘关节恐怖三联征的诊治进展[J].同济大学学报(医学版),2010,31(1):5-11.[20] Regan W, Morrey B. Fractures of the coronoid process of the ulna. J Bone Joint Surg Am. 1989;71(9):1348-1354.[21] Mason ML. Some observations on fractures of the head of the radius with a review of one hundred cases. Br J Surg. 1954; 42(172):123-132.[22] Durakbasa MO, Gumussuyu G, Gungor M, et al. Distal humeral coronal plane fractures: management, complications and outcome. J Shoulder Elbow Surg. 2013;22(4):560-566.[23] Riseborough EJ, Radin EL. Intercondylar T fractures of the humerus in the adult. A comparison of operative and non-operative treatment in twenty-nine cases. J Bone Joint Surg Am. 1969;51(1):130-141.[24] Wong AS, Baratz ME. Elbow fractures: distal humerus. J Hand Surg Am. 2009;34(1):176-190.[25] Lumsdaine W, Enninghorst N, Hardy BM, et al. Patterns of CT use and surgical intervention in upper limb periarticular fractures at a level-1 trauma centre. Injury. 2013;44(4): 471-474.[26] McCollough CH, Primak AN, Saba O, et al. Dose performance of a 64-channel dual-source CT scanner. Radiology. 2007;243(3):775-784.[27] Cody DD, Stevens DM, Ginsberg LE. Multi-detector row CT artifacts that mimic disease. Radiology. 2005;236(3):756-761.[28] 王土兴,王立章,俞方荣.多层螺旋CT在骨创伤诊断中的临床价值[J].中国医学影像技术,2003,19(1):118-119.[29] Jelly LM, Evans DR, Easty MJ, et al. Radiography versus spiral CT in the evaluation of cervicothoracic junction injuries in polytrauma patients who have undergone intubation. Radiographics. 2000;20 Spec No:S251-9; discussion S260-262.[30] Klingebiel R, Kentenich M, Bauknecht HC, et al. Comparative evaluation of 64-slice CT angiography and digital subtraction angiography in assessing the cervicocranial vasculature. Vasc Health Risk Manag. 2008;4(4):901-907.[31] Guitton TG, Ring D; Science of Variation Group. Interobserver reliability of radial head fracture classification: two-dimensional compared with three-dimensionalCT. J Bone Joint Surg Am. 2011;93(21):2015-2021.[32] Adams JE, Sanchez-Sotelo J, Kallina CF 4th, et al. Fractures of the coronoid: morphology based upon computer tomography scanning. J Shoulder Elbow Surg. 2012;21(6): 782-788.[33] Kotsianos D, Rock C, Euler E, et al. 3-D imaging with a mobile surgical image enhancement equipment (ISO-C-3D). Initial examples of fracturediagnosis of peripheral joints in comparison with spiral CT and conventional radiography. Unfallchirurg. 2001;104(9):834-838.[34] Rieker O, Mildenberger P, Rudig L, et al. 3D CT of fractures: comparison of volume and surface reconstruction. Rofo. 1998;169(5):490-494.[35] Dewailly M, Rémy-Jardin M, Duhamel A, et al. Computer- aided detection of acute pulmonary embolism with 64-slice multi-detector row computed tomography: impact of the scanning conditions and overall image quality in the detection of peripheral clots. J Comput Assist Tomogr. 2010;34(1): 23-30.[36] Mowatt G, Cummins E, Waugh N, et al. Systematic review of the clinical effectiveness and cost-effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of coronary artery disease. Health Technol Assess. 2008; 12(17): Iii-iv, ix-143.[37] Gufler H, Schulze CG, Wagner S, et al. MRI for occult physeal fracture detection in children and adolescents. Acta Radiol. 2013.[38] Rhyou IH, Kim KC, Kim KW, et al. Collateral ligament injury in the displaced radial head and neck fracture: correlation with fracture morphology and management strategy to the torn ulnar collateral ligament. J Shoulder Elbow Surg. 2013;22(2): 261-267.[39] Timmerman LA, Schwartz ML, Andrews JR. Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography. Evaluation in 25 baseball players with surgical confirmation. Am J Sports Med. 1994;22(1):26-31; discussion 32.[40] Fritz RC, Steinbach LS, Tirman PF, et al. MR imaging of the elbow. An update. Radiol Clin North Am. 1997;35(1):117-144. |
| [1] | Xu Feng, Kang Hui, Wei Tanjun, Xi Jintao. Biomechanical analysis of different fixation methods of pedicle screws for thoracolumbar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1313-1317. |
| [2] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [3] | Chen Xinmin, Li Wenbiao, Xiong Kaikai, Xiong Xiaoyan, Zheng Liqin, Li Musheng, Zheng Yongze, Lin Ziling. Type A3.3 femoral intertrochanteric fracture with augmented proximal femoral nail anti-rotation in the elderly: finite element analysis of the optimal amount of bone cement [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1404-1409. |
| [4] | Du Xiupeng, Yang Zhaohui. Effect of degree of initial deformity of impacted femoral neck fractures under 65 years of age on femoral neck shortening [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1410-1416. |
| [5] | Zhang Shangpu, Ju Xiaodong, Song Hengyi, Dong Zhi, Wang Chen, Sun Guodong. Arthroscopic suture bridge technique with suture anchor in the treatment of acromioclavicular dislocation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1417-1422. |
| [6] | Zhang Chao, Lü Xin. Heterotopic ossification after acetabular fracture fixation: risk factors, prevention and treatment progress [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1434-1439. |
| [7] | Zhou Jihui, Li Xinzhi, Zhou You, Huang Wei, Chen Wenyao. Multiple problems in the selection of implants for patellar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1440-1445. |
| [8] | Wang Debin, Bi Zhenggang. Related problems in anatomy mechanics, injury characteristics, fixed repair and three-dimensional technology application for olecranon fracture-dislocations [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1446-1451. |
| [9] | Hu Kai, Qiao Xiaohong, Zhang Yonghong, Wang Dong, Qin Sihe. Treatment of displaced intra-articular calcaneal fractures with cannulated screws and plates: a meta-analysis of 15 randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1465-1470. |
| [10] | Liu Yafei, Wang Yalin, Zuo Yanping, Sun Qi, Wei Jing, Zhao Lixia. Structural changes of the temporomandibular joint in adolescents with skeletal Class III malocclusions after maxillary protraction: an X-ray measurement analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1154-1159. |
| [11] | Shen Jinbo, Zhang Lin. Micro-injury of the Achilles tendon caused by acute exhaustive exercise in rats: ultrastructural changes and mechanism [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1190-1195. |
| [12] | Zou Gang, Xu Zhi, Liu Ziming, Li Yuwan, Yang Jibin, Jin Ying, Zhang Jun, Ge Zhen, Liu Yi. Human acellular amniotic membrane scaffold promotes ligament differentiation of human amniotic mesenchymal stem cells modified by Scleraxis in vitro [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1037-1044. |
| [13] | He Li, Tian Wei, Xu Song, Zhao Xiaoyu, Miao Jun, Jia Jian. Factors influencing the efficacy of lumbopelvic internal fixation in the treatment of traumatic spinopelvic dissociation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 884-889. |
| [14] | Yang Weiqiang, Ding Tong, Yang Weike, Jiang Zhengang. Combined variable stress plate internal fixation affects changes of bone histiocyte function and bone mineral density at the fractured end of goat femur [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 890-894. |
| [15] | Zhang Lei, Ma Li, Fu Shijie, Zhou Xin, Yu Lin, Guo Xiaoguang. Arthroscopic treatment of greater tuberosity avulsion fractures with anterior shoulder dislocation using the double-row suture anchor technique [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 895-900. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||