Chinese Journal of Tissue Engineering Research ›› 2019, Vol. 23 ›› Issue (36): 5861-5867.doi: 10.3969/j.issn.2095-4344.1978
Previous Articles Next Articles
Rotational positioning of femoral prosthesis in total knee arthroplasty
- 1Department of Orthopedic Surgery, Affiliated Ruikang Hospital of Guangxi University of Chinese Medicine, Nanning 530001, Guangxi Zhuang Autonomous Region, China; 2Department of Orthopedic Surgery, The People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning 530021, Guangxi Zhuang Autonomous Region, China
-
Online:2019-12-28Published:2019-12-28 -
Contact:Li Shuzhen, Master, Associate chief physician, Department of Orthopedic Surgery, Affiliated Ruikang Hospital of Guangxi University of Chinese Medicine, Nanning 530001, Guangxi Zhuang Autonomous Region, China; Department of Orthopedic Surgery, The People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning 530021, Guangxi Zhuang Autonomous Region, China -
About author:Zeng Feng, Master candidate, Physician, Department of Orthopedic Surgery, Affiliated Ruikang Hospital of Guangxi University of Chinese Medicine, Nanning 530001, Guangxi Zhuang Autonomous Region, China -
Supported by:the Self-Funded Research Projects in Guangxi Zhuang Autonomous Region, No. Z20180878 (to LSZ)
CLC Number:
Cite this article
Zeng Feng, Li Shuzhen. Rotational positioning of femoral prosthesis in total knee arthroplasty[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(36): 5861-5867.
share this article

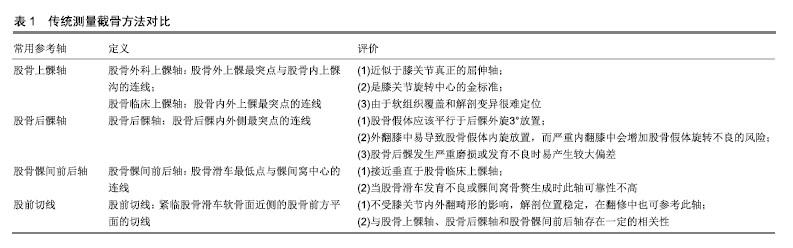
2.1 股骨假体旋转定位方法 全膝关节置换重建下肢正 常力线并使膝关节获得矩形屈曲间隙是手术关键一步,而其中又包括两方面内容:一是膝关节内外侧软组织的松解;二则是术中截骨的精确性。目前临床医生在术中判断股骨假体旋转定位常用的方法有:测量截骨法、间隙平衡法和计算机辅助导航技术[3,9-10]。 2.1.1 测量截骨技术 测量截骨技术通过股骨远端解剖标志进行定位[11-12],临床常以股骨后髁轴、上髁轴和Whiteside’s线作为参考轴,有研究指出该技术操作简单、学习曲线短,并可以维持置换后关节的稳定[13-14]。但该技术也有一定的局限性,如不同程度骨性关节炎患者之间骨性标志具有个体化差异,而临床医生通过术中肉眼观察及判断也受个人临床经验的影响[15]。 2.1.2 股骨上髁轴 股骨上髁轴由2条参考轴线组成:外科上髁轴和临床上髁轴。股骨外科上髁轴定义为股骨外上髁最突点与股骨内上髁沟的连线,而股骨临床上髁轴定义为股骨内外上髁最突点的连线。股骨上髁轴与膝关节的功能轴处于平行位置,当膝关节进行屈伸活动时,此轴线最为接近,Czurda等[16]和Vanin等[17]的研究中指出参照股骨上髁轴进行截骨可以保证良好的髌股运动轨迹,并改善胫股关节,从而获得矩形屈曲关节间隙。Franceschini等[18]的研究中得出类似结论。股骨外科上髁轴平行于膝关节,并且不受膝关节内外翻畸形的影响[19-20],参照股骨外科上髁轴截骨可以获得良好的旋转对线,在股骨髁发育不良或股骨后髁发生磨损时可选用此参考轴线,并且在翻修手术中也能参照此轴。Kobayashi等[21]的一项研究中纳入了70例骨性关节炎患者,分析患者膝关节在屈曲0°,30°,60°,90°和120°时股骨外科上髁轴与其他股骨远端参考轴线角度间的关系,发现股骨外科上髁轴作为膝关节的主轴,其角度在膝关节屈曲0°-60°之间保持不变,从而认为股骨外科上髁轴作为膝关节旋转中心,对股骨假体的旋转定位具有指导意义。而作者认为该研究中仅从CT图像来分析股骨外科上髁轴与其他股骨远端参考轴线间的关系具有一定局限性,CT图像不能对软骨进行显影,影响股骨远端内外上髁骨性标志的定位。并且该研究中纳入人群仅为骨关节炎患者,缺少正常组的对照,所以作者认为对于股骨外科上髁轴是否能作为膝关节旋转中心仍然需要大量样本及研究的支持。但股骨内上髁切迹显露困难,并且不同术者或同一术者在不同时间定位不一样,只有44%-75%的准确率[22-23]。 骨关节炎患者膝关节骨赘形成及软组织的覆盖导致术中定位困难,对膝关节严重外翻畸形或股骨后髁磨损较重的患者,术者选择股骨临床上髁轴较为可靠[15,24-25]。临床医生在术中应根据患者股骨远端内外侧髁或后髁骨质磨损程度及软组织覆盖情况灵活选用参考轴进行手术。 2.1.3 股骨后髁轴 股骨后髁轴是指股骨后髁内外侧最凸出点的连线。当膝关节处于屈曲位置时,外侧韧带结构处于松弛状态,而胫骨平台在冠状面上并不平行于地面,存在一个平均3°的生理内翻角度[26],因此,当术中不需要松解内侧软组织时,将股骨假体置于一定的外旋角度,才能弥补胫骨平台的生理内翻,从而获得矩形的屈曲间隙。van der Linden-van der Zwaag等[27]指出,股骨假体平均2.5°外旋放置才能保证下肢力线对齐,从而获得良好的屈曲关节间隙。该研究结论与膝关节正常生理内翻角度相契合,对临床上股骨假体外旋放置提供了依据。在正常或内翻、轻度畸形的膝关节截骨中可参照此轴线进行截骨。但Konigsberg等[6]和Yip等[23]的研究表明,在外翻膝外侧后髁发育不良,内翻膝内侧后髁骨软骨磨损状态下进行的截骨,会使得股骨假体过度内旋或外旋放置,并且在翻修中,此参考轴线不存在。该研究还指出股骨上髁轴与后髁轴的夹角在性别之间差异有显著性意义,若膝外翻畸形并伴有后髁骨质严重破坏的患者,特别是股骨后髁存在过度退变或者股骨后髁发育较小的患者,股骨上髁轴与后髁轴之间的夹角度数较大,从而加大股骨内外侧髁畸形程度,此时若参考股骨后髁外旋3°进行截骨会发生较大的误差。 2.1.4 股骨髁间前后轴 Whiteside等[11,28]将“股骨髁间前后轴”定义为:股骨滑车最低点与股骨髁间窝中心的连线。此线是髌骨活动的最佳路线,在初次全膝关节置换中较容易标记并且重复性高,对周围软组织损伤 小[29]。当股骨后髁发育不良或存在骨缺损时参考此线较可靠,它不受膝关节内外翻畸形的影响。但在严重骨关节炎或股骨远端髁发育不良患者中,参照此轴线进行截骨将产生一定的误差,并且在翻修中,此线不存在,而在健康人群中变异度较大。Amaranath等[19]对256例骨性关节炎患者的MRI图像进行对比测量,发现Whiteside’s线与股骨上髁轴的角度平均为(92.6±2.3)°,而Park等[20]的研究发现Whiteside’s线与股骨上髁轴之间的角度平均为(92.4±3.5)°,二者之间的角度在年龄、性别及内外翻畸形之间无明显相关性,但仅参照Whiteside’s线进行截骨,有约1/3股骨假体会发生内旋放置,因此认为术中结合Whiteside’s线与股骨上髁轴进行截骨将减少股骨假体发生内旋的概率。 作者认为在股骨滑车发育不良或髌股关节发生严重磨损时参照股骨髁间前后轴会产生一定误差,由于解剖标志难以定位,通过肉眼观察将发生标记线偏移,所以术中可结合股骨上髁轴或后髁轴进行定位,来获得准确的力线及旋转。 2.1.5 股前切线 股前切线又称作股骨前轴,是由Talbot等[30]在2008年最早提出的。股骨前轴指紧临股骨滑车软骨面近侧的股骨前方平面的切线。Whiteside’s线前后轴的垂线外旋3°(-2.9°±-1.7°)与股前切线平行,二者之间差异无显著性意义。所以认为可以参考股前切线对股骨假体进行旋转定位,在膝关节翻修中,若其他参考轴线难以定位,也可参照此轴进行定位。Won等[31]在研究中对骨性关节炎患者的CT进行测量,得出相似结论:股骨外科上髁轴与股前切线、股骨后髁轴、Whiteside’s线之间的角度在不同患者之间变化范围较大,而股前切线与股骨后髁轴和Whiteside’s线的角度在不同患者中变化范围较小,角度恒定。Watanabe等[32]对150例骨性关节炎患者置换前股前切线与股骨上髁轴之间的角度进行测量,发现股前切线相比临床上髁轴平均有(12.2±3.9)°的内旋,而相对于外科上髁轴平均有(7.3±4.0)°的内旋,这说明了股前切线与股骨上髁轴的角度是密切相关的,无论在置换前还是手术当中对股前切线与股骨上髁轴夹角的测量在全膝关节置换中具有一定参考价值。这些测量结果与先前的研究结果相似,从这些研究结果来看,股前切线可作为股骨假体旋转对线上一个有用的参考指标[13,33]。但目前为止,临床上对股前切线的研究数据较少,其精确性及可靠性尚需进一步研究证实。上述传统测量截骨方法常用参考轴线对比见表1。"

2.2 间隙平衡技术 间隙平衡技术最早是由Insall等[14]提出,即韧带松解后膝关节维持在软组织平衡状态,使股骨与胫骨间的间隙成矩形,然后进行股骨远端和胫骨平台面的截骨,使膝关节在屈伸间隙上达到平衡状态,从而恢复膝关节的稳定性。而Samuelson等[13]在1970年提出屈膝间隙优先的原则,Insall等[14,34-35]在此基础上进行了改进并提出了在使用活动衬垫型假体中采取伸膝间隙优先的原则。采用间隙平衡法进行截骨时,膝关节活动度较大,对软组织干扰少,患者恢复好,疗效满意。对于正常膝或内翻膝,使用间隙平衡技术可使假体放置准确,但对于膝外翻角度较大的患者(膝外翻>10°),使用该技术将加大股骨外旋角度,导致术后膝关节不稳。有研究表明:使用间隙平衡技术可提高膝关节屈曲稳定性并增加假体的使用寿命,因为间隙平衡技术不依赖股骨远端解剖学标志,在重建下肢正常力线方面具有优势,但患者置换后临床疗效却没有明显变化[36-38]。Kim等[39]的一项前瞻性随机对照试验,对150例使用间隙平衡法的患者CT图像进行了测量,发现术中将张力装置设置为30 N,将导致股骨假体产生更大的外旋,所以建议临床医生在术中可将张力装置设置为20 N,可以获得更好的股骨假体旋转。Fehring等[36]对100例用测量截骨法和间隙平衡法行全膝关节置换的患者进行了比较,发现采用测量截骨法行全膝关节置换的患者中有45%的股骨假体旋转角度偏差小于3°,因此认为间隙平衡法可以减小股骨假体内外旋的角度。Itokazu等[40]对48例行全膝关节置换的患者进行研究,分别用后髁轴外旋3°、平行于股骨临床上髁轴和平行于股骨外科上髁轴的截骨方式对屈曲关节间隙进行评估,发现不同参考轴线进行截骨后出现的离群值分别为25%、27%和31%。所以股骨远端髁的解剖标志并不总是平行于屈曲的胫骨截骨面,要建立一个矩形的屈曲关节间隙,不仅要依靠解剖标志,也要考虑韧带平衡,将二者结合起来,才能正确放置股骨假体,使下肢获得正常力线。 2.3 计算机辅助导航技术(Computer aided navigation technology) 全膝关节置换中,应用测量截骨技术和间隙平衡法容易受到患者膝关节骨质条件、畸形程度及临床医生经验判断等因素的影响。近年来,计算机辅助导航技术开始被引入手术当中,该技术在降低出血量、避免破坏髓腔及降低脂肪栓塞方面优势较大,但目前为止,由于应用该技术耗时较长,技术难掌握且费用较高,所以临床未得到普及。Choong等[3]的临床随机对照试验中分别比较了传统手术方法和计算机辅助导航技术对于股骨假体旋转在全膝关节置换中的精确性,发现计算机辅助导航技术下定位股骨假体旋转的精确性要高于传统手术,并且置换后膝关节稳定性和临床效果要好。Joseph等[41]进行的一项前瞻性临床随机对照研究中也发现计算机辅助导航技术在重建内外侧伸直间隙上优势明显,但在屈曲间隙方面差异无显著性意义。该作者对其研究的患者进行5年随访后,发现计算机辅助导航技术组置换后的患者膝关节活动度及评分指标高于传统手术组,但后期临床效果有待进一步随访研究[35,42]。Lützner等[43]对80例患者置换后X射线片及CT图像进行分析,发现应用计算机辅助导航技术行全膝关节置换患者股骨假体旋转角度恒定,并且假体位置能够放置准确,但胫骨假体旋转角度变化较大。因此认为计算机辅助导航技术在确定股骨假体旋转对线上是更为可靠以及可重复的方法。但也有很多学者不赞同上述观点。Amanatullah等[44]研究了股骨远端假体旋转定位的安全范围,发现股骨远端上髁轴的个体化差异较大,且安全范围少于2 mm,所以认为计算机辅助导航技术并不能够获得满意的置换后疗效。Benjamin等[45]对50例应用计算机辅助导航技术下行全膝关节置换的患者进行研究,评估术中选用股骨假体的大小,结果发现52%的患者术中选用的股骨假体比置换前要小。因此认为应用计算机辅助导航技术进行关节置换时应该注意个体化差异。Kendoff等[46]应用8合1截骨板结合计算机辅助导航技术对成人尸体膝关节进行截骨,判断股骨假体是否能够准确的放置及产生的偏差范围,结果显示在冠状面上,股骨假体平均有(0.9±1.7)°的内旋,(0.8±2.3) mm的前移,(0.3±1) mm的后移;在矢状面和轴位面上平均有(2.8±2.5)°的屈曲,(3.4±1.3) mm的前移,(0.7±2.7)°的外旋。因此得出,在计算机辅助导航技术下用八合一截骨板进行截骨,对膝关节轴位旋转、截骨高度和膝关节内外精确度较高,但在矢状面和轴位面上却存在一定的偏差。 2.4 3D打印技术 3D打印技术作为一项新技术,近年逐渐被引入了医学领域,并应用于骨科临床当中。Won等[47]在全髋关节置换中运用3D打印技术打印出髋臼模型,在术中确定假体的类型、大小和位置从而保证假体能够精确植入。Qiao等[48]运用3D打印技术设计出个性化的外固定支架,减少手术创伤并且能够对骨折断端进行精准复位,使得创伤骨科手术中的操作更简便。Lu等[49]运用3D打印技术研制出了用于颈椎椎弓根内固定的新型钻孔模板行颈椎椎弓根内固定,并且实现了更为安全的螺钉定位。Sun等[50]运用3D打印技术专门为盆腔肿瘤切除患者设计出一种半骨盆假体,从而快速有效弥补了置换后骨缺损。 3D打印技术辅助全膝关节置换则是通过计算机软件对患者置换前的CT图像进行三维重建并测量计算出最佳截骨量及截骨角度,然后模拟整个虚拟手术过程,设计并打印出个性化的截骨模板和膝关节模型以备术中使用。对比传统全膝关节置换,利用3D打印技术设计出个性化的截骨模板辅助进行手术可缩短手术时间并减少围术期出血量[51]。孙振国等[52]的一项临床研究中对32例骨关节炎外翻畸形患者分别采用传统全膝关节置换和3D打印技术辅助全膝关节置换进行比较,发现采用3D打印技术辅助全膝关节置换要比传统全膝关节置换手术时间短、失血量少、并且能够恢复下肢力线。传统全膝关节置换中由于入髓杆插入股骨髓腔位置较深导致手术创伤较大、失血量增多,而3D打印技术辅助下的全膝关节置换,可以准确定位股骨入髓的位置,缩短入髓深度,从而提高了准确性并减少了手术创伤。使用3D打印技术辅助全膝关节置换可以精确截骨,使得假体能够放置准确,而传统方式全膝关节置换中对于截骨量和力线的判断多数依赖临床医生个人的经验和肉眼观察,存在一定的误差[53]。有部分研究中表明3D打印技术辅助全膝关节置换临床疗效满意,值得推广[54-55]。而Cucchi等[56]的一项前瞻性随机对照试验中分别用传统全膝关节置换和个性化截骨模板对24例骨关节炎患者进行手术,并记录手术时间,截骨量及使用的假体大小,发现二者间差异无显著性意义,但运用传统全膝关节置换方式进行截骨的患者股骨假体产生了更大的外旋角度。发现运用个性化截骨模板进行截骨后,58%的患者仍然需要在术中更换假体尺寸。所以笔者认为临床医生在运用3D打印技术辅助全膝关节置换仍然需要在置换前仔细进行评估,用计算机软件进行建模,并反复计算出最佳截骨量及截骨方向,针对患者的个体化差异设计出个性化截骨模板和膝关节模型,从而保证截骨精准化。但由于3D打印技术辅助全膝关节置换属于新生事物且个性化截骨模板设计较复杂,临床上未能够得到普及,目前临床上关于3D打印技术辅助全膝关节置换的研究较少,样本量不足且临床医生学习该技术的学习曲线较长,仍需要广大学者进一步研究。但该技术符合现代微创理念的时代要求,具有创新性,值得推广,相信随着科学技术和临床医生水平的不断提高,3D打印技术辅助全膝关节置换将会迎来更广阔的发展前景。 2.5 机器人辅助全膝关节置换技术 随着科学技术的不断进步,机器人辅助外科手术开始出现,机器人辅助外科手术系统可以分为3类[57-58]。①主动型:完全由机器人根据置换前计划自主切割工具进行手术;②半主动型:由医师参与指挥并控制机器人的机械手臂在规划路径上进行操作;③被动型:机器人完全按照医师的指挥控制,放置截骨模板等工具,机器人机械臂动作完全由医师进行操控,而临床考虑到手术的安全性和可靠性,目前应用最多的是被动型机器人。机器人辅助全膝关节置换技术即置换前将患者CT图像导入机器人工作站,并在冠状面、矢状面各个方向及距离进行调整,保证良好的对线,通过识别一些解剖标志定位解剖轴和机械轴,然后进行虚拟手术确定植入假体型号大小。术中将机械手臂摆在合适位置,对相应骨性标志进行注册并标记,根据图像反馈信息进行相应调整,最后确认整个手术计划,在计算机辅助导航监测系统下用机械臂进行切割,最后清理骨赘及软组织后安装试模,位置合适后即取出试模放入假体。但目前临床上对机器人辅助直接应用于全膝关节置换的报道较少,而应用机器人辅助行单髁置换的报道较多。有相关文献报道机器人辅助单髁置换的精准度较高,并能够降低假体位置放置不良和误差的发生率[59-61]。Cobb等[62]的一项随机对照试验中对28例行机器人辅助单髁置换和传统单髁置换的临床疗效进行了比较,发现机器人辅助单髁置换组置换后力线偏差均在2°范围内,而传统单髁置换组仅有40%置换后力线偏差在2°范围之内,并且发现机器人辅助单髁置换组置换后膝关节功能评分也要高于传统组。Suero等[63]对12例尸体进行研究,对比机器人辅助单髁置换和传统单髁置换中假体放置的准确性,发现机器人辅助技术组股骨假体误差为1.9 mm和3.7°,而传统单髁置换组误差为5.4 mm和10.2°,从而得出机器人辅助单髁置换股骨假体精确性要高。虽然机器人辅助技术下行单髁置换提高了术中截骨的精确度及假体植入准确率,但由于缺乏大量样本及及对照试验,临床疗效仍有待进一步观察。有许多医院已经开展了机器人辅助膝关节置换,但由于购买整套设备价格昂贵,并且对于机器人及其相关设备的安装与调试都比较复杂,手术的安全性及可靠性难以得到保证,临床上还未能够得到普及。作者认为今后研发的重点应该放在提升机器人控制系统的安全性及可靠性上,研发专门针对手术的医用型机器人,结合微创时代理念,加快机器人辅助全膝关节置换领域的发展。"

| [1]Johnson DR, Dennis DA, Kindsfater KA, et al. Evaluation of total knee arthroplasty performed with and without computer navigation: a bilateral total knee arthroplasty study. J Arthroplasty. 2013;28(3):455-458. [2]Patel AR, Talati RK, Yaffe MA, et al. Femoral component rotation in total knee arthroplasty: an MRI-based evaluation of our options. J Arthroplasty. 2014;29(8):1666-1670.[3]Choong PF, Dowsey MM, Stoney JD. Does accurate anatomical alignment result in better function and quality of life? Comparing conventional and computer-assisted total knee arthroplasty. J Arthroplasty. 2009;24(4):560-569. [4]Seo JG, Moon YW, Kim SM, et al. Easy identification of mechanical axis during total knee arthroplasty. Yonsei Med J. 2013;54(6):1505-1510. [5]Vanin N, Panzica M, Dikos G, et al. Rotational alignment in total knee arthroplasty: intraoperative inter- and intraobserver reliability of Whiteside's line. Arch Orthop Trauma Surg. 2011;131(11): 1477-1480. [6]Konigsberg B, Hess R, Hartman C, et al. Inter- and intraobserver reliability of two-dimensional CT scan for total knee arthroplasty component malrotation. Clin Orthop Relat Res.2014;472(1): 212-217.[7]Pietsch M, Hofmann S. Early revision for isolated internal malrotation of the femoral component in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2012;20(6):1057-1063. [8]Cinotti G, Ripani FR, Sessa P, et al. Combining different rotational alignment axes with navigation may reduce the need for lateral retinacular release in total knee arthroplasty. Int Orthop. 2012; 36(8):1595-1600.[9]Walde TA, Bussert J, Sehmisch S, et al. Optimized functional femoral rotation in navigated total knee arthroplasty considering ligament tension. Knee. 2010;17(6):381-386. [10]Moon YW, Seo JG, Lim SJ, et al. Variability in femoral component rotation reference axes measured during navigation-assisted total knee arthroplasty using gap technique. J Arthroplasty. 2010;25(2): 238-243.[11]Whiteside LA, Arima J. The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty. Clin Orthop Relat Res.1995;(321):168-172.[12]Laskin RS. Flexion space configuration in total knee arthroplasty. J Arthroplasty. 1995;10(5):657-660.[13]Samuelson KM, Freeman MA, Levack B, et al. Homograft bone in revision acetabular arthroplasty. A clinical and radiographic study. J Bone Joint Surg Br. 1988;70(3):367-372.[14]Insall J, Ranawat CS, Scott WN, et al. Total condylar knee replacment: preliminary report. Clin Orthop Relat Res. 1976;(120): 149-154.[15]Siston RA, Patel JJ, Goodman SB, et al. The variability of femoral rotational alignment in total knee arthroplasty. J Bone Joint Surg Am. 2005t;87(10):2276-2280.[16]Czurda T, Fennema P, Baumgartner M, et al. The association between component malalignment and post-operative pain following navigation-assisted total knee arthroplasty: results of a cohort/nested case-control study. Knee Surg Sports Traumatol Arthrosc. 2010;18(7):863-869.[17]Vanin N, Panzica M, Dikos G, et al. Rotational alignment in total knee arthroplasty: intraoperative inter- and intraobserver reliability of Whiteside's line. Arch Orthop Trauma Surg. 2011;131(11): 1477-1480.[18]Franceschini V, Nodzo SR, Gonzalez Della Valle A. Femoral Component Rotation in Total Knee Arthroplasty: A Comparison Between Transepicondylar Axis and Posterior Condylar Line Referencing. J Arthroplasty. 2016;31(12):2917-2921. [19]Amaranath JE, Moopanar TR, Sorial RM. Defining distal femoral anatomy for rotational alignment in total knee arthroplasty: a magnetic resonance imaging-based study. ANZ J Surg. 2014; 84(11):852-855. [20]Park A, Duncan ST, Nunley RM, et al. Relationship of the posterior femoral axis of the "kinematically aligned" total knee arthroplasty to the posterior condylar, transepicondylar, and anteroposterior femoral axes. Knee. 2014;21(6):1120-1123. [21]Kobayashi H, Akamatsu Y, Kumagai K, et al. Is the surgical epicondylar axis the center of rotation in the osteoarthritic knee? J Arthroplasty. 2015;30(3):479-483.[22]Tang WM, Zhu YH, Chiu KY. Axial alignment of the lower extremity in Chinese adults. J Bone Joint Surg Am. 2000;82(11): 1603-1608.[23]Yip DK, Zhu YH, Chiu KY, et al. Distal rotational alignment of the Chinese femur and its relevance in total knee arthroplasty. J Arthroplasty. 2004;19(5):613-619.[24]Akagi M, Yamashita E, Nakagawa T, et al. Relationship between frontal knee alignment and reference axes in the distal femur. Clin Orthop Relat Res. 2001;(388):147-156.[25]Yoshino N, Takai S, Ohtsuki Y, et al. Computed tomography measurement of the surgical and clinical transepicondylar axis of the distal femur in osteoarthritic knees. J Arthroplasty. 2001;16(4): 493-497.[26]Lee CM, Dhillon MK1, Sulaiman MA. A computer-assisted, tibia-first technique for improved femoral component rotation in total knee arthroplasty. Arthroplast Today. 2017;4(1):78-84.[27]van der Linden-van der Zwaag HM, Valstar ER, van der Molen AJ, et al. Transepicondylar axis accuracy in computer assisted knee surgery: a comparison of the CT-based measured axis versus the CAS-determined axis. Comput Aided Surg. 2008;13(4):200-206.[28]Arima J, Whiteside LA, McCarthy DS, et al. Femoral rotational alignment, based on the anteroposterior axis, in total knee arthroplasty in a valgus knee. A technical note. J Bone Joint Surg Am. 1995;77(9):1331-1334.[29]Manili M, Muratori F, Fredella N. Whiteside line as the reliable surgical landmark for femoral rotation in total knee arthroplasty. Radiological validation. Eur J Orthop Surg Traumatol. 2007; 17(6):599-602.[30]Talbot S, Bartlett J. The anterior surface of the femur as a new landmark for femoral component rotation in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2008;16(3):258-262.[31]Won YY, Cui WQ, Baek MH, et al. An additional reference axis for determining rotational alignment of the femoral component in total knee arthroplasty. J Arthroplasty. 2007;22(7):1049-1053.[32]Watanabe H, Gejo R, Matsuda Y, et al. Femoral anterior tangent line of the osteoarthritic knee for determining rotational alignment of the femoral component in total knee arthroplasty. J Arthroplasty. 2011;26(2):268-273.[33]Watanabe H, Gejo R, Tokunaga A, et al. Intraoperative measurements of femoral anterior tangent (FAT) line for determining the rotational alignment of femoral component of total knee arthroplasty. J Arthroplasty. 2013;28(10):1757-1759.[34]Insall JN, Binazzi R, Soudry M, et al. Total knee arthroplasty. Clin Orthop Relat Res. 1985;(192):13-22.[35]Scott RD. Femoral and tibial component rotation in total knee arthroplasty: methods and consequences. Bone Joint J. 2013; 95-B(11 Suppl A):140-143.[36]Fehring TK. Rotational malalignment of the femoral component in total knee arthroplasty. Clin Orthop Relat Res. 2000(380):72-79.[37]Katz MA, Beck TD, Silber JS, et al. Determining femoral rotational alignment in total knee arthroplasty: reliability of techniques. J Arthroplasty. 2001;16(3):301-305.[38]Dennis DA, Komistek RD, Kim RH, et al. Gap balancing versus measured resection technique for total knee arthroplasty. Clin Orthop Relat Res. 2010;468(1):102-107.[39]Kim JI, Chun SH, Han HS, et al. Femoral component rotations in different gap tensions in total knee arthroplasty: A prospective randomized controlled trial. Knee. 2017;24(2):439-446.[40]Itokazu M, Minoda Y, Ikebuchi M, et al. Anatomical landmarks of the distal femoral condyles are not always parallel to the tibial bone cut surface in flexion during total knee arthroplasty. Knee. 2016;23(4):725-729.[41]Joseph J, Simpson PM, Whitehouse SL, et al. The use of navigation to achieve soft tissue balance in total knee arthroplasty - a randomised clinical study. Knee. 2013;20(6):401-406.[42]Ishida K, Matsumoto T, Tsumura N, et al. Mid-term outcomes of computer-assisted total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2011;19(7):1107-1112.[43]Lützner J, Krummenauer F, Wolf C, et al. Computer-assisted and conventional total knee replacement: a comparative, prospective, randomised study with radiological and CT evaluation. J Bone Joint Surg Br. 2008;90(8):1039-1044.[44]Amanatullah DF, Di Cesare PE, Meere PA, et al. Identification of the landmark registration safe zones during total knee arthroplasty using an imageless navigation system. J Arthroplasty. 2013;28(6):938-942.[45]Benjamin J. Determining femoral component position using CAS and measured resection. Clin Orthop Relat Res. 2008;466(11): 2745-2750.[46]Kendoff DO, Moreau-Gaudry A, Plaskos C, et al. A navigated 8-in-1 femoral cutting guide for total knee arthroplasty technical development and cadaveric evaluation. J Arthroplasty. 2010;25(1):138-145.[47]Won SH, Lee YK, Ha YC, et al. Improving pre-operative planning for complex total hip replacement with a Rapid Prototype model enabling surgical simulation. Bone Joint J. 2013;95-B(11): 1458-1463.[48]Qiao F, Li D, Jin Z, et al. Application of 3D printed customized external fixator in fracture reduction. Injury. 2015;46(6):1150-1155.[49]Lu S, Xu YQ, Chen GP, et al. Efficacy and accuracy of a novel rapid prototyping drill template for cervical pedicle screw placement. Comput Aided Surg. 2011;16(5):240-248.[50]Sun W, Li J, Li Q, et al. Clinical effectiveness of hemipelvic reconstruction using computer-aided custom-made prostheses after resection of malignant pelvic tumors. J Arthroplasty. 2011; 26(8):1508-1513.[51]Boonen B, Schotanus MG, Kerens B, et al. Intra-operative results and radiological outcome of conventional and patient-specific surgery in total knee arthroplasty: a multicentre, randomised controlled trial. Knee Surg Sports Traumatol Arthrosc. 2013; 21(10):2206-2212.[52]孙振国,翁伟,李恒,等.3D打印技术辅助全膝关节置换术治疗骨关节炎膝外翻畸形的临床研究[J].中医正骨,2018,30(6):36-41,45.[53]MacDessi SJ, Jang B, Harris IA, et al. A comparison of alignment using patient specific guides, computer navigation and conventional instrumentation in total knee arthroplasty. Knee. 2014;21(2):406-409.[54]Ng VY, DeClaire JH, Berend KR, et al. Improved accuracy of alignment with patient-specific positioning guides compared with manual instrumentation in TKA. Clin Orthop Relat Res. 2012; 470(1):99-107.[55]孙茂淋,何锐,陈光兴,等.3D打印导航模板在全膝关节置换术中的应用[J].中华骨与关节外科杂志,2019,12(3):195-200.[56]Cucchi D, Menon A, Aliprandi A, et al. Patient-specific Instrumentation Affects Rotational Alignment of the Femoral Component in Total Knee Arthroplasty: A Prospective Randomized Controlled Trial. Orthop Surg. 2019;11(1):75-81.[57]Netravali NA, Shen F, Park Y, et al. A perspective on robotic assistance for knee arthroplasty. Adv Orthop. 2013;2013:970703.[58]Medical Advisory Secretariat. Computer-assisted hip and knee arthroplasty. Navigation and active robotic systems: an evidence-based analysis. Ont Health Technol Assess Ser. 2004;4(2):1-39.[59]Mofidi A, Plate JF, Lu B, et al. Assessment of accuracy of robotically assisted unicompartmental arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014;22(8):1918-1925.[60]Plate JF, Mofidi A, Mannava S, et al. Achieving accurate ligament balancing using robotic-assisted unicompartmental knee arthroplasty. Adv Orthop. 2013;2013:837167.[61]Lonner JH, Smith JR, Picard F, et al. High degree of accuracy of a novel image-free handheld robot for unicondylar knee arthroplasty in a cadaveric study. Clin Orthop Relat Res. 2015;473(1):206-212.[62]Cobb J, Henckel J, Gomes P, et al. Hands-on robotic unicompartmental knee replacement: a prospective, randomised controlled study of the acrobot system. J Bone Joint Surg Br. 2006;88(2):188-197.[63]Suero EM, Citak M, Kraneburg UM, et al. Robotic-assisted unicompartmental knee arthroplasty in a patient with combined medial compartment arthritis and subchondral defect of the medial femoral condyle. Knee. 2012;19(5):724-727. |
| [1] | Lu Dezhi, Mei Zhao, Li Xianglei, Wang Caiping, Sun Xin, Wang Xiaowen, Wang Jinwu. Digital design and effect evaluation of three-dimensional printing scoliosis orthosis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1329-1334. |
| [2] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [3] | Li Dadi, Zhu Liang, Zheng Li, Zhao Fengchao. Correlation of total knee arthroplasty efficacy with satisfaction and personality characteristics [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1346-1350. |
| [4] | Wei Wei, Li Jian, Huang Linhai, Lan Mindong, Lu Xianwei, Huang Shaodong. Factors affecting fall fear in the first movement of elderly patients after total knee or hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1351-1355. |
| [5] | Wang Jinjun, Deng Zengfa, Liu Kang, He Zhiyong, Yu Xinping, Liang Jianji, Li Chen, Guo Zhouyang. Hemostatic effect and safety of intravenous drip of tranexamic acid combined with topical application of cocktail containing tranexamic acid in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1356-1361. |
| [6] | Xiao Guoqing, Liu Xuanze, Yan Yuhao, Zhong Xihong. Influencing factors of knee flexion limitation after total knee arthroplasty with posterior stabilized prostheses [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1362-1367. |
| [7] | Huang Zexiao, Yang Mei, Lin Shiwei, He Heyu. Correlation between the level of serum n-3 polyunsaturated fatty acids and quadriceps weakness in the early stage after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1375-1380. |
| [8] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [9] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [10] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Comparison of the short-term efficacy of extracorporeal shock wave therapy for middle-aged and elderly knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1471-1476. |
| [11] | Zhong Hehe, Sun Pengpeng, Sang Peng, Wu Shuhong, Liu Yi. Evaluation of knee stability after simulated reconstruction of the core ligament of the posterolateral complex [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 821-825. |
| [12] | Liu Zhengpeng, Wang Yahui, Zhang Yilong, Ming Ying, Sun Zhijie, Sun He. Application of 3D printed interbody fusion cage for cervical spondylosis of spinal cord type: half-year follow-up of recovery of cervical curvature and intervertebral height [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 849-853. |
| [13] | Zhao Zhongyi, Li Yongzhen, Chen Feng, Ji Aiyu. Comparison of total knee arthroplasty and unicompartmental knee arthroplasty in treatment of traumatic osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 854-859. |
| [14] | Liu Shaohua, Zhou Guanming, Chen Xicong, Xiao Keming, Cai Jian, Liu Xiaofang. Influence of anterior cruciate ligament defect on the mid-term outcome of fixed-bearing unicompartmental knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 860-865. |
| [15] | Zhang Nianjun, Chen Ru. Analgesic effect of cocktail therapy combined with femoral nerve block on total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 866-872. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||