Chinese Journal of Tissue Engineering Research ›› 2026, Vol. 30 ›› Issue (27): 6969-6977.doi: 10.12307/2026.446
Finite element analysis of effects of opening wedge high tibial osteotomy on knee joint and internal fixation stress
Chen Ping, Lu Hongxu, Xilinbaoleri
- Department of Orthopedics, Inner Mongolia International Mongolian Medicine Hospital, Hohhot 010000, Inner Mongolia Autonomous Region, China
-
Received:2025-10-29Accepted:2026-01-23Online:2026-09-28Published:2026-04-16 -
Contact:Xilinbaoleri, MD, Chief physician, Department of Orthopedics, Inner Mongolia International Mongolian Medicine Hospital, Hohhot 010000, Inner Mongolia Autonomous Region, China -
About author:Chen Ping, MS, Associate chief physician, Department of Orthopedics, Inner Mongolia International Mongolian Medicine Hospital, Hohhot 010000, Inner Mongolia Autonomous Region, China -
Supported by:Inner Mongolia Autonomous Region Science and Technology Plan Project, No. 2022YFSH0127 (to CP)
CLC Number:
Cite this article
Chen Ping, Lu Hongxu, Xilinbaoleri. Finite element analysis of effects of opening wedge high tibial osteotomy on knee joint and internal fixation stress[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(27): 6969-6977.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
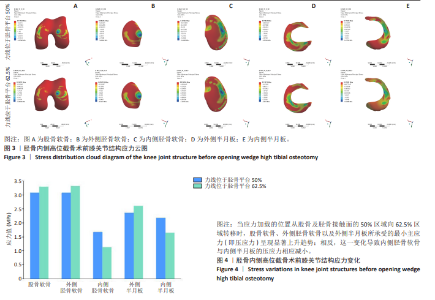
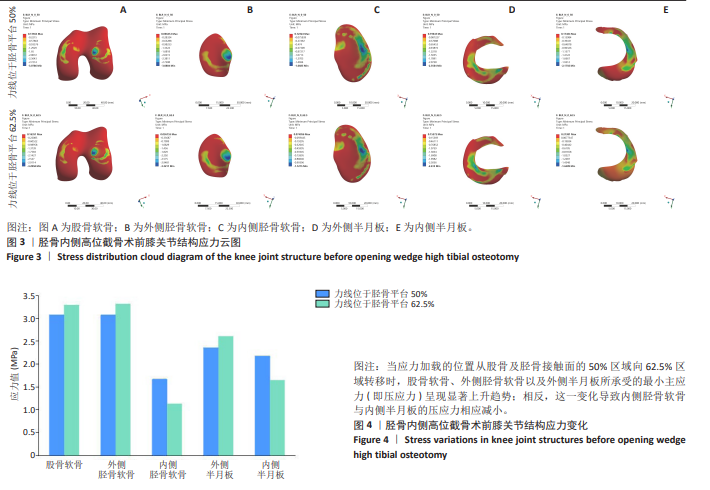
2.1 胫骨内侧高位截骨术前膝关节模型应力变化 软骨应力集中于股骨外侧髁的内上角处、胫骨平台前内侧,即软骨最易磨损部位。半月板应力集中于内侧半月板体部、外侧半月板前角及前角移行处,即半月板最易撕裂部位。当应力加载的位置从股骨及胫骨接触面的50%区域向62.5%区域转移时,股骨软骨、外侧胫骨软骨以及外侧半月板所承受的最小主应力(即压应力)呈现显著上升趋势;相反,这一变化导致内侧胫骨软骨与内侧半月板的压应力相应减小(图3,4)。"
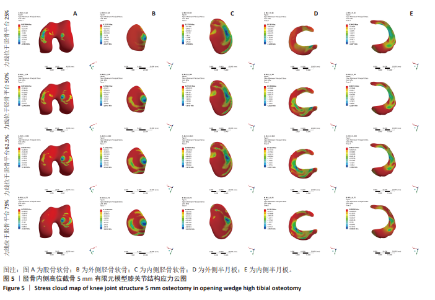
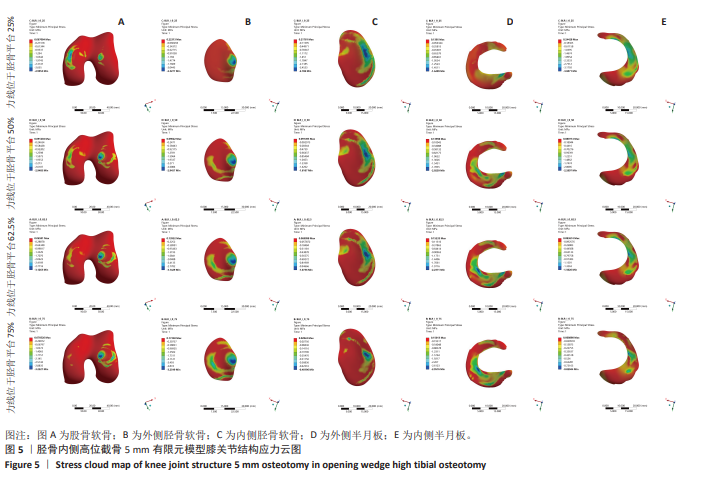
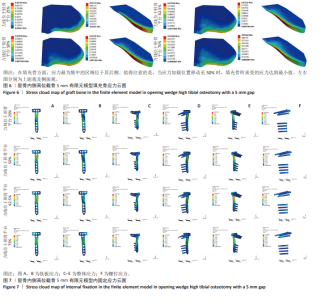
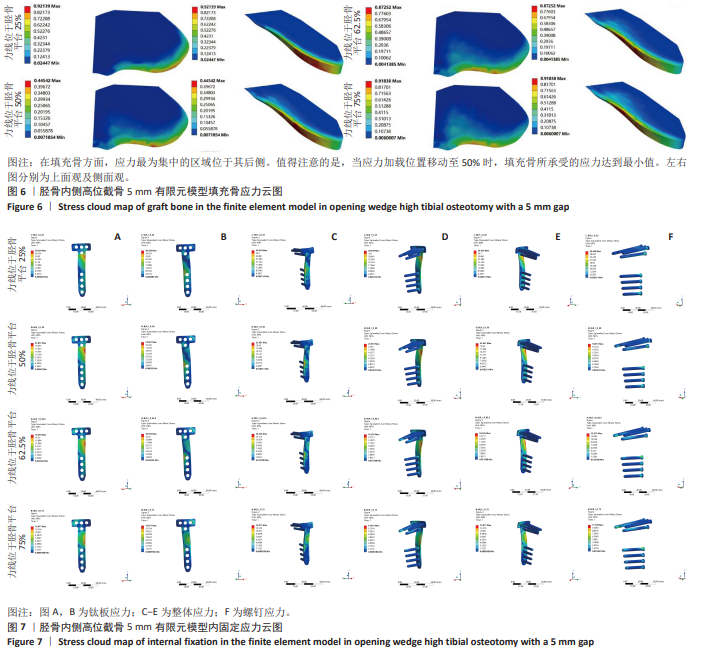
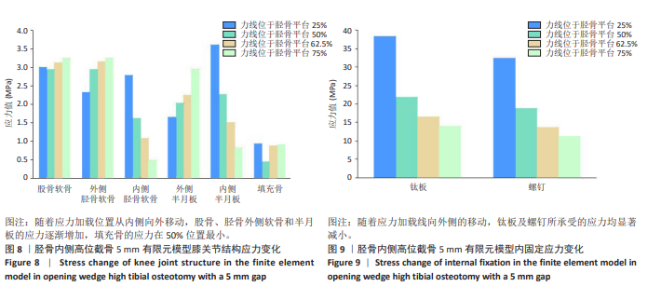
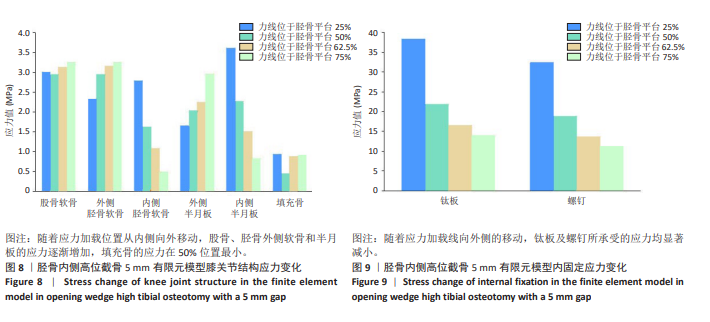
2.2 胫骨内侧高位截骨5 mm时不同力线位置的应力变化 胫骨内侧高位截骨5 mm模型中,于胫骨平台25%,50%,62.5%,75%处加载应力并对胫骨内侧高位截骨术后膝关节各结构及填充骨和内固定装置进行应力分析(图5-9)。25%应力加载模型中,股骨软骨表面高应力区域位于股骨内侧髁的内侧,随着应力加载位置向外侧移动,逐渐转移至股骨外侧髁的内上角。同时,外侧胫骨平台软骨的高应力值集中于胫骨外侧髁,而内侧胫骨平台的高应力值则位于胫骨内侧区域,且内侧胫骨软骨所承受的应力显著高于外侧胫骨髁。随着加载位置向外侧偏移,应力逐渐转移至胫骨外侧髁软骨表面。外侧半月板上表面的高应力区域主要集中在前角及前角移行区,而内侧半月板上表面的高应力区域则主要集中于后角及体部。随着应力加载位置外移,外侧半月板的应力逐渐增大,并愈发集中于外侧半月板前角处;相反,内侧半月板的应力则呈现减小趋势。在填充骨方面,应力最为集中的区域位于其后侧。值得注意的是,当应力加载位置移动至50%时,填充骨所承受的应力达到最小值。钛板的应力主要集中于其中间后内侧区域,而螺钉的应力则主要集中于D孔及1孔螺钉[28-30](D孔及1孔于图1中予以标注)。随着应力加载线向外侧的移动,钛板及螺钉所承受的应力均显著减小。 "
"
"

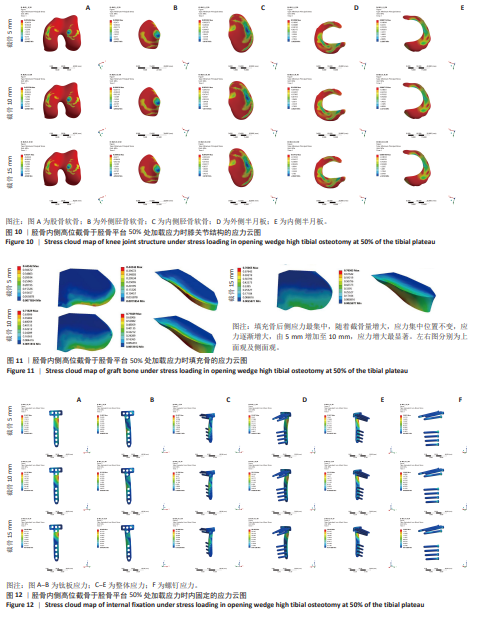
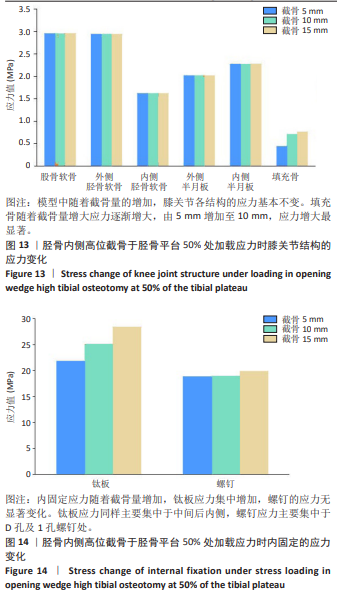
2.3 胫骨内侧高位截骨力线在胫骨平台50%时不同截骨高度的应力变化 在胫骨内侧高位截骨术后模型中,分析力线位于胫骨平台50%及5,10,15 mm截骨量时术后膝关节各结构及内固定的应力变化云图,见图10-14。模型中随着截骨量的增加,膝关节各结构及内固定位置的应力基本不变。股骨软骨表面高应力值位于股骨外侧髁的内侧,外侧胫骨软骨表面高应力值位于胫骨外髁,内侧胫骨软骨表面高应力值位于胫骨内侧,其中胫骨外髁应力大于内侧胫骨软骨应力。外侧半月板上表面高应力值集中于前角及前角移行处,内侧半月板上表面高应力值集中于后角及体部。填充骨后侧应力最集中,随着截骨量增大,应力集中位置不变,应力逐渐增大,由5 mm增加至10 mm,应力增大最显著。内固定应力随着截骨量增加,钛板应力集中增加,螺钉的应力无显著变化。钛板应力同样主要集中于中间后内侧,螺钉应力主要集中于D孔及1孔螺钉处。"

"
| [1] 廖德发. 我国骨性关节炎流行病学调查现状[J]. 微创医学,2017,12(4): 521-524. [2] PENG H, OU A, HUANG X, et al. Osteotomy Around the Knee: The Surgical Treatment of Osteoarthritis. Orthop Surg. 2021;13(5):1465-1473. [3] LEE SS, OH J, LEE DH. Change in Cartilage Status of Medial Compartment after Open-Wedge High Tibial Osteotomy without Cartilage Regeneration Procedure: Second Look Arthroscopic Assessment. Biomedicines. 2023;11(6):1639. [4] FUJISAWA Y, MASUHARA K, SHIOMI S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop Clin North Am. 1979;10(3):585-608. [5] TRIPON M, SAUTET P, ARGENSON JN, et al. Is the lateral tibial spine a reliable landmark for planning tibial or femoral valgus osteotomies? Orthop Traumatol Surg Res. 2022;108(3):103253. [6] 张子峥, 罗旺, 刘长路. 膝内侧间室骨关节炎单髁置换中有限元分析的应用价值[J]. 中国组织工程研究,2026,30(9):2313-2322. [7] 李清瀚, 王大麟. 有限元分析技术在内侧开放性楔形胫骨高位截骨术研究中的应用进展[J]. 吉林医学,2022,43(6):1683-1685. [8] 熊华章, 斯海波, 吴元刚, 等. 有限元分析在胫骨高位截骨治疗膝内侧间室骨关节炎的研究进展[J]. 中国矫形外科杂志,2022,30(15):1377-1380. [9] 范建波, 崔胜宇, 逸弘, 等. TomoFix钢板固定胫骨高位截骨术治疗膝关节骨性关节炎的疗效[J]. 中国老年学杂志,2021,41(16):3432-3436. [10] KANG KT, KOH YG, LEE JA, et al. The influence of the number of holes in the open wedge high tibial osteotomy on knee biomechanics using finite element analysis. Orthop Traumatol Surg Res. 2021;107(4):102884. [11] RAJA IZAHAM RM, ABDUL KADIR MR, ABDUL RASHID AH, et al. Finite element analysis of Puddu and Tomofix plate fixation for open wedge high tibial osteotomy. Injury. 2012;43(6):898-902. [12] AHMED AM, ADDOSOOKI A, SALEH SLEEM A, et al. Superior survivorship and plate-related results of TomoFix compared to Puddu plate fixation for opening-wedge high tibial osteotomy: A systematic review of the literature. Knee. 2023;42: 1-18. [13] YABUUCHI K, KONDO E, ONODERA J, et al. Clinical Outcomes and Complications During and After Medial Open-Wedge High Tibial Osteotomy Using a Locking Plate: A 3- to 7-Year Follow-up Study. Orthop J Sports Medicine. 2020;8(6): 2325967120922535. [14] NELISSEN EM, VAN LANGELAAN EJ, NELISSEN RG. Stability of medial opening wedge high tibial osteotomy: a failure analysis. Int Orthop. 2010;34(2):217-223. [15] LUO CA, LIN SC, HWA SY, et al. Biomechanical effects of plate area and locking screw on medial open tibial osteotomy. Comput Methods Biomech Biomed Engin. 2015;18(12):1263-1271. [16] CHEN YN, CHANG CW, LI CT, et al. Biomechanical investigation of the type and configuration of screws used in high tibial osteotomy with titanium locking plate and screw fixation. J Orthop Surg Res. 2019;14(1):35. [17] RÖDERER G, GEBHARD F, DUERSELEN L, et al. Delayed bone healing following high tibial osteotomy related to increased implant stiffness in locked plating. Injury. 2014;45(10):1648-1652. [18] 刘蒙飞, 陈刚, 史易晗, 等. 骨质疏松患者单髁置换过程中股骨假体置入位置优化的有限元分析[J]. 中国组织工程研究,2025,29(3):464-470. [19] JIANG D, ZHAN S, WANG Q, et al. Biomechanical Comparison of Locking Plate and Cancellous Screw Techniques in Medial Malleolar Fractures: A Finite Element Analysis. J Foot Ankle Surg. 2019;58(6):1138-1144. [20] NI M, ZHANG F, MEI J, et al. Biomechanical analysis of four augmented fixations of plate osteosynthesis for comminuted mid-shaft clavicle fracture: A finite element approach. Exp Ther Med. 2020;20(3):2106-2112. [21] PEÑA E, CALVO B, MARTÍNEZ MA, et al. A three-dimensional finite element analysis of the combined behavior of ligaments and menisci in the healthy human knee joint. J Biomech. 2006;39(9):1686-1701. [22] HOPKINS AR, NEW AM, RODRIGUEZ-Y-BAENA F, et al. Finite element analysis of unicompartmental knee arthroplasty. Med Eng Phys. 2010;32(1):14-21. [23] TUNCER M, COBB JP, HANSEN UN, et al. Validation of multiple subject-specific finite element models of unicompartmental knee replacement. Med Eng Phys. 2013;35(10):1457-1464. [24] PEÑA E, CALVO B, MARTÍNEZ MA, et al. Finite element analysis of the effect of meniscal tears and meniscectomies on human knee biomechanics. Clin Biomech (Bristol). 2005;20(5):498-507. [25] KANG KT, SON J, KWON SK, et al. Preservation of femoral and tibial coronal alignment to improve biomechanical effects of medial unicompartment knee arthroplasty: Computational study. Biomed Mater Eng. 2018;29(5):651-664. [26] 张吉超, 董万鹏, 董跃福, 等. 膝关节有限元模型参数设置[J]. 中国组织工程研究,2021,25(30):4781-4786. [27] JI W, LUO C, ZHAN S, et al. Combined proximal tibial osteotomy for varus osteoarthritis of the knee: Biomechanical tests and finite-element analyses. Knee. 2020;27(3):863-870. [28] CHEN YN, CHUANG CH, YANG TH, et al. Computational comparison of different plating strategies in medial open-wedge high tibial osteotomy with lateral hinge fractures. J Orthop Surg Res. 2020;15(1):409. [29] NHA KW, JUNG WH, KOH YG, et al. D-hole breakage of 2 angular stable locking plates for medial opening-wedge high tibial osteotomy: Analysis of results from 12 cases. Medicine. 2019;98(2):e14138. [30] KANG KT, KOH YG, LEE JA, et al. Biomechanical effect of a lateral hinge fracture for a medial opening wedge high tibial osteotomy: finite element study. J Orthop Surg Res. 2020;15(1):63. [31] XU H, TU H, ZHAO T, et al. Comparison of the clinical effects for different positions of the weight-bearing axis after high tibial osteotomy. J Orthop Surg Res. 2023; 18(1):423. [32] JIANG X, LI B, XIE K, et al. Lateral tibial intercondylar eminence is a reliable reference for alignment correction in high tibial osteotomy. Knee Surg Sports Traumatol Arthroscopy. 2023;31(4):1515-1523. [33] MARTINEZ DE ALBORNOZ P, LEYES M, FORRIOL F, et al. Opening wedge high tibial osteotomy: plate position and biomechanics of the medial tibial plateau. Knee Surg Sports Traumatol Arthroscopy. 2014;22(11):2641-2647. [34] MARTAY JL, PALMER AJ, BANGERTER NK, et al. A preliminary modeling investigation into the safe correction zone for high tibial osteotomy. Knee. 2018; 25(2):286-295. [35] 梁秋娟, 刘潇, 古丽奴儿·沙吾提,等. 持续静压力通过TRPV4信号通路调控大鼠软骨细胞凋亡[J]. 中国骨质疏松杂志,2025,31(4):507-511+517. [36] 吴斌, 刘兆祥, 张月红, 等. 过度机械应力调控Piezo1介导成软骨细胞铁死亡的机制探讨[J]. 天津医药,2025,53(1):14-18. [37] 白玉明, 张海森, 刘畅, 等. 胫骨高位截骨术治疗单纯内侧间室膝骨关节炎术后炎性细胞因子水平变化研究[J]. 中国修复重建外科杂志,2017,31(4): 422-426. [38] GUILAK F, FERMOR B, KEEFE FJ, et al. The role of biomechanics and inflammation in cartilage injury and repair. Clin Orthop Relat Res. 2004;(423):17-26. [39] PAN CS, WANG X, DING LZ, et al. The best position of bone grafts in the medial open-wedge high tibial osteotomy: A finite element analysis. Comput Methods Programs Biomed. 2023;228:107253. [40] 于成双, 马剑雄, 卢斌, 等. 不同填充块对内侧开放楔形胫骨高位截骨应力分布的影响[J]. 医用生物力学,2023,38(1):84-89. [41] ZHAO XW, FAN ZR, MA JX, et al. Reinforcement strategy for medial open-wedge high tibial osteotomy: a finite element evaluation of the additional opposite screw technique and bone grafts. Comput Methods Programs Biomed. 2022;213: 106523. [42] GANESH VK, RAMAKRISHNA K, GHISTA DN. Biomechanics of bone-fracture fixation by stiffness-graded plates in comparison with stainless-steel plates. Biomed Eng Online. 2005;4:46. [43] MEHMOOD S, ALI MN, ANSARI U, et al. Auxetic polymeric bone plate as internal fixator for long bone fractures: Design, fabrication and structural analysis. Technol Health Care. 2015;23(6):819-833. [44] JAEBLON T. Biomechanics of far cortical locking. J Orthop Trauma. 2011;25(6): e60. |
| [1] | Chen Qiuhan, Yang Long, Yuan Daizhu, Wu Zhanyu, Zou Zihao, Ye Chuan. Peri-knee osteotomy for treatment of knee osteoarthritis: optimization of treatment strategies [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2303-2312. |
| [2] | Zhang Zizheng, Luo Wang, Liu Changlu. Application value of finite element analysis on unicompartmental knee arthroplasty for medial knee compartmental osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2313-2322. |
| [3] | Zhao Feifan, Cao Yujing. Risk factors and coping strategies of internal fixation failure in treatment of intertrochanteric fracture with proximal femoral nail antirotation [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2323-2333. |
| [4] | Chen Huiting, Zeng Weiquan, Zhou Jianhong, Wang Jie, Zhuang Congying, Chen Peiyou, Liang Zeqian, Deng Weiming. Tail anchoring technique of vertebroplasty in treatment of osteoporotic vertebral compression fractures with intravertebral cleft: a finite element analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2145-2152. |
| [5] | Cheng Qisheng, Julaiti·Maitirouzi, Xiao Yang, Zhang Chenwei, Paerhati·Rexiti. Finite element analysis of novel variable-diameter screws in modified cortical bone trajectory of lumbar vertebrae [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2162-2171. |
| [6] | Liu Jiafu, Ren Ruxia, Liao Zhouwei, Zhou Xiali, Wu Yihong, Zhang Shaoqun. Three-dimensional finite element analysis of cervical spine biomechanical characteristics in a rat model of cervical vertigo [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2182-2190. |
| [7] | Liu Wenlong, Dong Lei, Xiao Zhengzheng, Nie Yu. Finite element analysis of tibial prosthesis loosening after fixed-bearing unicompartmental knee arthroplasty for osteoporosis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2191-2198. |
| [8] | Zheng Wangyang, Fei Ji, Yang Di, Zhao Lang, Wang Lingli, Liu Peng, Li Haiyang. Finite element analysis of the force changes of the supraspinatus tendon and glenohumeral joint during the abduction and flexion of the humerus [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2199-2207. |
| [9] | Cai Qirui, Dai Xiaowei, Zheng Xiaobin, Jian Sili, Lu Shaoping, Liu Texi, Liu Guoke, Lin Yuanfang. Mechanical effects of Long’s traction orthopedic method on cervical functional units: quantitative analysis of biomechanical model of head and neck [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2208-2216. |
| [10] | Rao Jingcheng, Li Yuwan, Zheng Hongbing, Xu Zhi, Zhu Aixiang, Shi Ce, Wang Bing, Yang Chun, Kong Xiangru, Zhu Dawei. Biomechanical differences between the new proximal femoral stable intramedullary nail and traditional intramedullary nail#br# [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2217-2225. |
| [11] | Chen Long, Wang Xiaozhen, Xi Jintao, Lu Qilin. Biomechanical performance of short-segment screw fixation combined with expandable polyetheretherketone vertebral body replacement in osteoporotic vertebrae [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2226-2235. |
| [12] | He Yixiang, Qiao Wanjia, Wang Wenji. Effectiveness and safety of tranexamic acid versus epsilon-aminocaproic acid in total hip and knee arthroplasties: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2361-2369. |
| [13] | Zheng Xuying, Hu Hongcheng, Xu Libing, Han Jianmin, Di Ping. Stress magnitude and distribution in two-piece cement-retained zirconia implants under different loading conditions and with varying internal connection shapes [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 1979-1987. |
| [14] | Zhong Caihong, Xiao Xiaoge, Li Ming, Lin Jianhong, Hong Jing. Biomechanical mechanism of sports-related patellar tendinitis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(6): 1417-1423. |
| [15] | Li Linzhen, Jiao Hongzhuo, Chen Weinan, Zhang Mingzhe, Wang Jianlong, Zhang Juntao. Effect of icariin-containing serum on lipopolysaccharide-induced inflammatory damage in human chondrocytes [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(6): 1368-1374. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||