Chinese Journal of Tissue Engineering Research ›› 2026, Vol. 30 ›› Issue (3): 570-576.doi: 10.12307/2025.909
Previous Articles Next Articles
High tibial osteotomy on a single plane: femorofibular angle as a reference marker for mechanical axis correction
Li Xiaomin1, Tian Xiangdong2, Wang Chaolu1
- 1Wangjing Hospital, China Academy of Chinese Medical Sciences, Beijing 100102, China; 2Third Affiliated Hospital of Beijing University of Chinese Medicine, Beijing 100029, China
-
Received:2024-09-04Accepted:2024-11-19Online:2026-01-28Published:2025-07-03 -
Contact:Corresponding author: Tian Xiangdong, Chief physician, Doctoral supervisor, Third Affiliated Hospital of Beijing University of Chinese Medicine, Beijing 100029, China Corresponding author: Wang Chaolu, Chief physician, Doctoral supervisor, Wangjing Hospital, China Academy of Chinese Medical Sciences, Beijing 100102, China -
About author:Li Xiaomin, Doctoral candidate, Wangjing Hospital, China Academy of Chinese Medical Sciences, Beijing 100102, China -
Supported by:Basic Research Business Expenses Project of Beijing University of Chinese Medicine, No. 2023-JYB-JBZD-026 (to TXD); Chinese Society of Traditional Chinese Medicine Information Research Project, No. CACMS-KY-2023008 (to WCL)
CLC Number:
Cite this article
Li Xiaomin, Tian Xiangdong, Wang Chaolu. High tibial osteotomy on a single plane: femorofibular angle as a reference marker for mechanical axis correction[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(3): 570-576.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
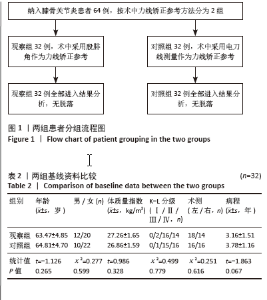
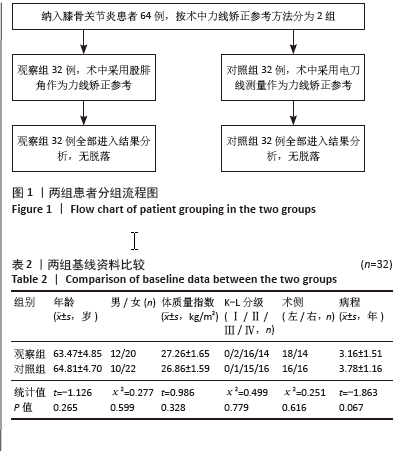
2.1 参与者数量分析 共纳入64例患者,均接受了单平面胫骨高位截骨术,观察组32例术中采用股腓角作为力线矫正参考,对照组32例术中采用电刀线测量作为力线矫正参考。两组均无脱落病例,在治疗期间均未发生严重不良反应。 2.2 试验流程图 见图1。 2.3 基线资料比较 两组患者基线资料比较,差异无显著性意义(P > 0.05),具有可比性,见表2。"
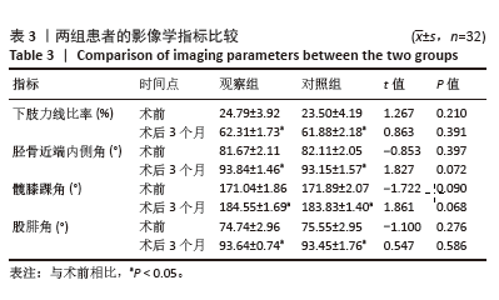
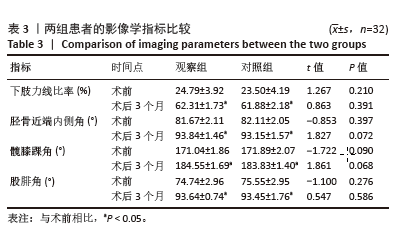
2.4 影像学指标结果 术前两组患者的下肢力线比率、胫骨近端内侧角、髋膝踝角及股腓角比较差异均无显著性意义(P > 0.05);术后3个月,两组患者的下肢力线比率、胫骨近端内侧角、髋膝踝角及股腓角均较术前显著改善,差异有显著性意义(P < 0.05),两组之间上述指标比较差异均无显著性意义(P > 0.05),见表3。"
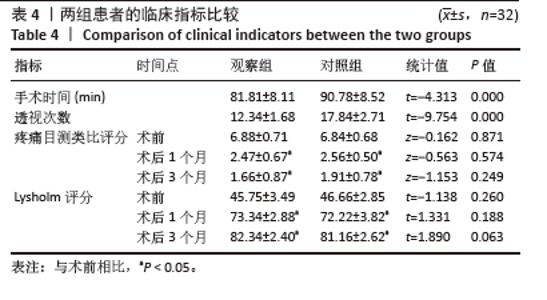
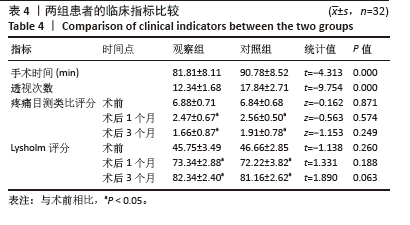
2.5 临床指标结果 术中观察组的手术时间和透视次数均少于对照组,差异有显著性意义(P < 0.05);术前及术后各随访节点,两组患者的疼痛目测类比评分及Lysholm评分比较差异均无显著性意义(P > 0.05);术后随时间的改变,两组患者的疼痛目测类比评分及Lysholm评分均较术前显著改善,差异有显著性意义(P < 0.05),见表4。"
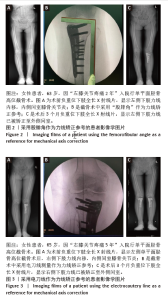
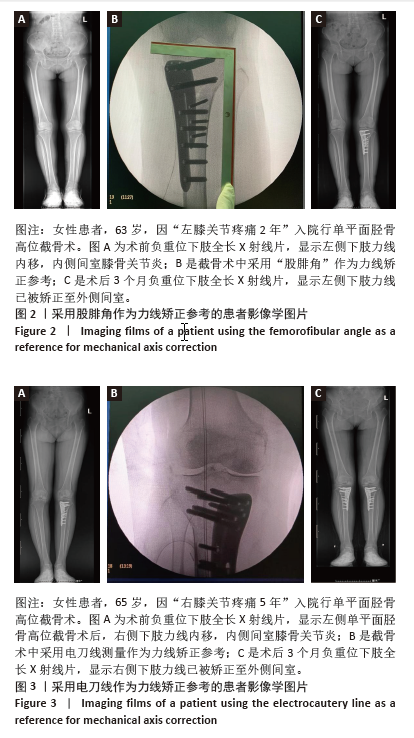
2.6 植入物与宿主的生物相容性 两组患者内固定材料生物相容性良好,在治疗期间均未发生内植物感染、过敏反应以及免疫排斥反应等。 2.7 典型病例 见图2,3。"
| [1] HUANG Y, LOBENHOFFER P, JIANG XY. Development of knee-preserving osteotomy in China. Sci Bull (Beijing). 2023;68(2):125-128. [2] 白浩, 孙海飚, 韩晓强, 等. 胫骨高位截骨与单髁置换治疗膝关节内侧间室骨关节炎的Meta分析[J]. 中国组织工程研究,2020,24(30): 4905-4913. [3] WU ZX, REN WX, WANG ZQ. Proximal fibular osteotomy versus high tibial osteotomy for treating knee osteoarthritis: a systematic review and meta-analysis. J Orthop Surg Res. 2022;17(1):470. [4] KIM MS, KOH IJ, SOHN S, et al. Unicompartmental knee arthroplasty is superior to high tibial osteotomy in post-operative recovery and participation in recreational and sports activities. Int Orthop. 2019; 43(11):2493-2501. [5] 韩昶晓, 田向东, 王剑, 等. 胫骨结节远端单平面截骨术对髌骨高度的影响[J]. 中华关节外科杂志(电子版),2020,14(5):559-564. [6] LONGINO PD, BIRMINGHAM TB, SCHULTZ WJ, et al. Combined tibial tubercle osteotomy with medial opening wedge high tibial osteotomy minimizes changes in patellar height: a prospective cohort study with historical controls. Am J Sports Med. 2013; 41(12):2849-2857. [7] HAN C, LI X, TIAN X, et al. The effect of distal tibial tuberosity high tibial osteotomy on postoperative patellar height and patellofemoral joint degeneration. J Orthop Surg Res. 2020;15(1):466. [8] 丁铭阳, 钟齐刚, 郑刘杰, 等. 胫骨高位截骨术中传统下肢力线测量法的指导意义[J]. 中华骨与关节外科杂志,2024,17(2):132-136. [9] 丁天送, 田向东, 谭冶彤, 等. 胫骨结节远端高位截骨术中MPTA与WBLR的相关性分析[J]. 实用骨科杂志,2023,29(5):405-410. [10] 石少辉, 刘路辉, 娄罡, 等. 改良胫骨结节下单平面胫骨高位截骨术治疗膝骨关节炎的疗效[J]. 临床骨科杂志,2022,25(5):644-647. [11] 许康永, 童也, 赵鹏, 等. 两种截骨术式治疗膝关节内侧间室骨关节炎的疗效比较[J]. 中国修复重建外科杂志,2021,35(11): 1440-1448. [12] LI K, GUO H, SUN F, et al. Less risk of patellofemoral degeneration without significant clinical and survivorship difference for distal tibial tuberosity high tibial osteotomy compared to biplanar high tibial osteotomy over a mid-term follow-up. J Orthop Surg (Hong Kong). 2024;32(2):793545797. [13] CHUNG K, JUNG M, JANG KM, et al. Acellular Particulated Costal Allocartilage Improves Cartilage Regeneration in High Tibial Osteotomy: Data From a Randomized Controlled Trial. Cartilage. 2024: 19476035241292321. doi: 10.1177/19476035241292321. [14] MICHAEL JW, SCHLUTER-BRUST KU, EYSEL P. The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee. Dtsch Arztebl Int. 2010;107(9):152-162. [15] FISCHER MA. From Morphology to Biomarker: Quantitative Texture Analysis of the Infrapatellar Fat Pad Reliably Predicts Knee Osteoarthritis. Radiology. 2022;304(3):622-623. [16] OLLIVIER B, BERGER P, DEPUYDT C, et al. Good long-term survival and patient-reported outcomes after high tibial osteotomy for medial compartment osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2021;29(11):3569-3584. [17] TAKAHARA Y, NAKASHIMA H, ITANI S, et al. Mid-term results of medial open-wedge high tibial osteotomy based on radiological grading of osteoarthritis. Arch Orthop Trauma Surg. 2023;143(1):149-158. [18] SCHUSTER P, GESSLEIN M, SCHLUMBERGER M, et al. Ten-Year Results of Medial Open-Wedge High Tibial Osteotomy and Chondral Resurfacing in Severe Medial Osteoarthritis and Varus Malalignment. Am J Sports Med. 2018;46(6):1362-1370. [19] GIMM G, JI H, RO DH, et al. Medial Joint Opening in the Operated Knee After Unilateral High Tibial Osteotomy: Risk of Osteoarthritis and Future Surgery in the Operated and Nonoperated Knee. Am J Sports Med. 2024;52(13):3266-3276. [20] 刘宇哲, 阿里木江·玉素甫, 覃祺, 等. 术前膝关节周围角度对胫骨高位截骨术下肢力线准确性矫正的研究进展[J]. 实用骨科杂志, 2023,29(10):933-938. [21] KARHU J, NYMAN M, SIITARI-KAUPPI M, et al. Cantilever-enhanced photoacoustic measurement of HTO in water vapor. Photoacoustics. 2023;29:100443. [22] 仲鹤鹤, 金瑛, 刘修齐, 等. 胫骨高位截骨钢板置入联合关节镜治疗伴下肢力线不良的内侧半月板后角退变性损伤[J]. 中国组织工程研究,2023,27(22):3531-3536. [23] KOSHINO T, YOSHIDA T, ARA Y, et al. Fifteen to twenty-eight years’ follow-up results of high tibial valgus osteotomy for osteoarthritic knee. Knee. 2004;11(6):439-444. [24] YOO JD, HUH MH, SHIN YS. Risk of revision in UKA versus HTO: a nationwide propensity score-matched study. Arch Orthop Trauma Surg. 2023;143(6):3457-3469. [25] HOHMANN E. Editorial Commentary: High Tibial Osteotomy May Not Be Required With Medial Meniscus Root Repair. Arthroscopy. 2023,39(3):647-649. [26] BENZAKOUR T, HEFTI A, LEMSEFFER M, et al. High tibial osteotomy for medial osteoarthritis of the knee: 15 years follow-up. Int Orthop. 2010;34(2):209-215. [27] MAEDA S, CHIBA D, SASAKI E, et al. The difficulty of continuing sports activities after open-wedge high tibial osteotomy in patient with medial knee osteoarthritis: a retrospective case series at 2-year-minimum follow-up. J Exp Orthop. 2021;8(1):68. [28] MARTAY JL, PALMER AJ, BANGERTER NK, et al. A preliminary modeling investigation into the safe correction zone for high tibial osteotomy. Knee. 2018;25(2):286-295. [29] LI OL, PRITCHETT S, GIFFIN JR, et al. High Tibial Osteotomy: An Update for Radiologists. AJR Am J Roentgenol. 2022;218(4):701-712. [30] JUNG WH, SAHU V, SEO M, et al. Cartilage regeneration and long term survival in medial OA knee patients treated with HTO and OATS. J Orthop. 2024;57:120-126. [31] FEUCHT MJ, MINZLAFF P, SAIER T, et al. Degree of axis correction in valgus high tibial osteotomy: proposal of an individualised approach. Int Orthop. 2014;38(11):2273-2280. [32] 金宇杰, 徐人杰, 周晓强, 等. AI术前规划+3D打印导板行胫骨高位截骨术治疗膝骨关节炎的临床疗效[J]. 生物骨科材料与临床研究,2024,21(3):21-26. [33] 李一凡, 孙广峰, 付廷, 等. 3D打印个体化导板辅助下胫骨高位截骨的精准度及临床疗效分析[J]. 解放军医学杂志,2024,49(12): 1366-1371. [34] 刘源, 柳剑, 黄野, 等. 导板辅助胫骨高位截骨术与经典截骨方式的临床对照研究[J]. 实用骨科杂志,2023,29(11):980-984. [35] 周观明,刘效仿,管明强,等.改良内侧开放式胫骨高位截骨术治疗膝内侧间室骨性关节炎[J].组织工程与重建外科,2021, 17(1):54-56. [36] HUANG Y, TAN Y, TIAN X, et al. Three-dimensional surgical planning and clinical evaluation of the efficacy of distal tibial tuberosity high tibial osteotomy in obese patients with varus knee osteoarthritis. Comput Methods Programs Biomed. 2022;213:106502. [37] 李珂, 孙凤龙, 王宏庆, 等. 改良单平面胫骨高位截骨术治疗膝关节骨关节炎的早期临床研究[J]. 中华骨与关节外科杂志,2020, 13(9):729-735. [38] 王宏庆,董婕,梁庆晨,等.开放楔形胫骨高位截骨术与膝单髁置换术治疗K-L Ⅲ级膝内侧间室骨关节炎的术后运动功能比较[J].中华骨与关节外科杂志,2024,17(5):423-430. [39] 程加峰,赵平,耿家金,等.计算机导航辅助与传统内侧开放胫骨高位截骨术治疗膝内侧骨关节炎的早期疗效比较[J].实用骨科杂志,2023,29(11):1032-1036. [40] 李瑶,梁文卫,李梦溪,等.髋-膝-踝角矫正率在胫骨高位截骨术中的应用[J].实用骨科杂志,2023,29(10):950-953. |
| [1] | Gu Fucheng, Yang Meixin, Wu Weixin, Cai Weijun, Qin Yangyi, Sun Mingyi, Sun Jian, Geng Qiudong, Li Nan. Effects of Guilu Erxian Glue on gut microbiota in rats with knee osteoarthritis: machine learning and 16S rDNA analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(4): 1058-1072. |
| [2] | Jia Yingao, Gao Shitao, Wang Fei. Application of 3D printed titanium cage cutting model in anterior cervical vertebrae subtotal decompression and bone graft fusion [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(3): 604-611. |
| [3] | Wang Jiangjing, Zhao Na, Hu Xiaona, Zhao Na . Safety of 3D printed titanium alloy bone trabecular cup prosthesis combined with modified Kidney Tonifying and Blood Activating Decoction for elderly hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(3): 612-619. |
| [4] | Guo Jingwen, Wang Qingwei, He Zijun, Hu Zihang, Chen Zhi, Zhu Rong, Wang Yuming, Liu Wenfei, Luo Qinglu. Intra-articular injection of different concentrations of silicon-based bioceramics in treatment of knee osteoarthritis in rats [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(2): 288-295. |
| [5] | Ma Chi, Wang Ning, Chen Yong, Wei Zhihan, Liu Fengji, Piao Chengzhe. Application of 3D-printing patient-specific instruments combined with customized locking plate in opening wedge high tibial osteotomy [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(9): 1863-1869. |
| [6] | Sun Yundi, Cheng Lulu, Wan Haili, Chang Ying, Xiong Wenjuan, Xia Yuan. Effect of neuromuscular exercise for knee osteoarthritis pain and function: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(9): 1945-1952. |
| [7] | Wang Peiguang, Zhang Xiaowen, Mai Meisi, Li Luqian, Huang Hao. Generalized equation estimation of the therapeutic effect of floating needle therapy combined with acupoint embedding on different stages of human knee osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(8): 1565-1571. |
| [8] | He Guanghui, Yuan Jie, Ke Yanqin, Qiu Xiaoting, Zhang Xiaoling. Hemin regulates mitochondrial pathway of oxidative stress in mouse chondrocytes [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(6): 1183-1191. |
| [9] | Ma Haoyu, Qiao Hongchao, Hao Qianqian, Shi Dongbo. Causal effects of different exercise intensities on the risk of osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(6): 1305-1311. |
| [10] | Wu Guangtao, Qin Gang, He Kaiyi, Fan Yidong, Li Weicai, Zhu Baogang, Cao Ying . Causal relationship between immune cells and knee osteoarthritis: a two-sample bi-directional Mendelian randomization analysis [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(5): 1081-1090. |
| [11] | Fang Ying, Zhang Yanwei, Li Xi, Yan Peidong, Bi Miao. Improvements in automatic diagnosis methods for knee osteoarthritis based on deep learning [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(35): 7511-7518. |
| [12] | Wang Lei, Li Chengsong, Zhang Shenshen, Wang Qing. Finite element analysis of biomechanical characteristics of three internal fixation methods in treatment of inferior patellar fracture [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(33): 7048-7054. |
| [13] | Liu Ning, Sun Yingjin, Huang Long, Feng Shuo, Chen Xiangyang. Optimal rotational alignment of the tibial component during Oxford unicompartmental knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(33): 7158-7164. |
| [14] | Yang Wanzhong, Ma Rong, Guo Wei, Wang Zhiqiang, Yang Wei, Chen Zhen, Wang Zemin, Zhang Honglai, Ge Zhaohui. One-stage posterior hemivertebra resection and pedicle screw fixation in treatment of congenital scoliosis: a 2-year follow-up of correction effect [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(33): 7173-7180. |
| [15] | Yan Jinlian, Xu Zhengquan, Wei Renjie, Wang Yehua. Hip joint function recovery and prediction model construction after proximal femoral nail antirotation for intertrochanteric fractures [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(33): 7189-7195. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||