Chinese Journal of Tissue Engineering Research ›› 2023, Vol. 27 ›› Issue (4): 539-546.doi: 10.12307/2023.251
Previous Articles Next Articles
Measuring the position relation between nerve tissue and bony structure in lumbar spinal canal decompression area by constructing a three-dimensional model of the lumbar spine
Wang Jianye, Liu Xin, Tian Lin, Sun Ning, Li Yuefei, Bi Jingwei, Liu Changzhen, Sun Zhaozhong
- Department of Spine Surgery, Affiliated Hospital of Binzhou Medical College, Binzhou 256603, Shandong Province, China
-
Received:2022-02-19Accepted:2022-04-18Online:2023-02-08Published:2022-06-22 -
Contact:Sun Zhaozhong, Chief physician, Department of Spine Surgery, Affiliated Hospital of Binzhou Medical College, Binzhou 256603, Shandong Province, China -
About author:Wang Jianye, Master candidate, Department of Spine Surgery, Affiliated Hospital of Binzhou Medical College, Binzhou 256603, Shandong Province, China -
Supported by:the National Key Research and Development Program, No. 2017YFC0114002 (to SZZ); Shandong Natural Science Foundation of China, No. 2R2017LH021 (to SZZ); Binzhou Medical College “Clinical + X” Project, No. BY2021LCX17 (to SZZ); Science and Technology Project of Binzhou Medical College, No. BY2018KJ03 (to LX)
CLC Number:
Cite this article
Wang Jianye, Liu Xin, Tian Lin, Sun Ning, Li Yuefei, Bi Jingwei, Liu Changzhen, Sun Zhaozhong . Measuring the position relation between nerve tissue and bony structure in lumbar spinal canal decompression area by constructing a three-dimensional model of the lumbar spine[J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 539-546.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
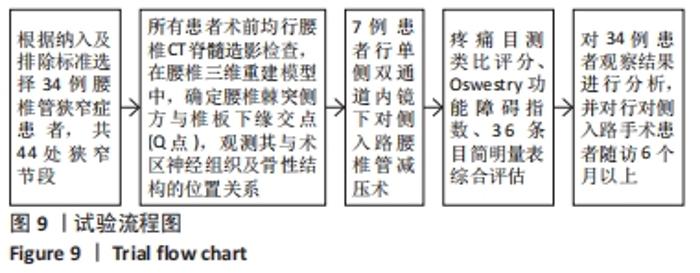
2.1 参与者数量分析 纳入34例患者,均进入结果分析。 2.2 试验流程图 见图9。"
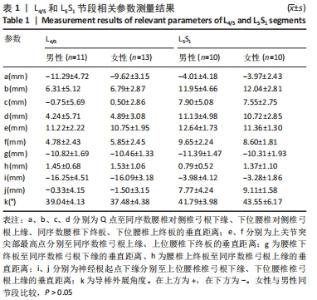
2.3 观测结果 2.3.1 研究组腰椎测量参数 L4/5和L5S1节段男性与女性之间各相关测量参数相比差异无显著性意义(P > 0.05),见表1。"

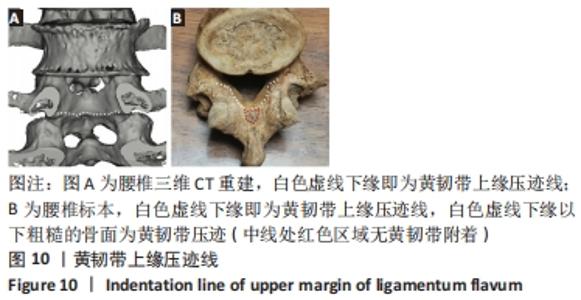
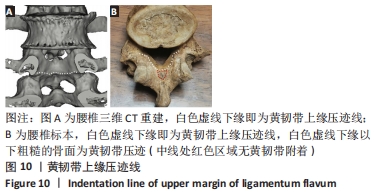
2.3.2 黄韧带压迹、腰椎峡部与周围骨性结构的关系 在三维CT中,清晰可见黄韧带附着的骨性结构处形成明显压迹,骨面粗糙,见图10。黄韧带除附着于上位腰椎板腹侧外,还向外、向下附着于腰椎峡部及下关节突腹侧,向下与关节突关节囊融合。黄韧带上缘压迹的连线近乎水平方向、向外延续至椎弓根下缘水平,称之为黄韧带上缘压迹线,该线对应黄韧带上缘,见图10。腰椎峡部位于下关节突基底部水平以上,峡部腹侧面骨质呈拱形向上、向前与椎弓根内下缘相连接,构成椎间孔后壁的上份,椎弓根下缘水平(即黄韧带上缘压迹线水平)以上仍有部分峡部、以下是大部分峡部,整个峡部腹侧向内与椎板腹侧相延续。从椎管内面观,黄韧带上缘压迹线的外侧部水平以下是峡部和下关节突。"
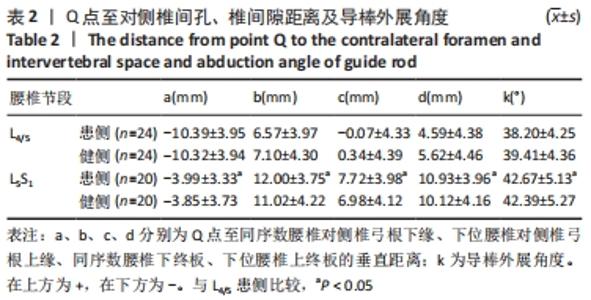
2.3.3 Q点与对侧椎间孔、椎间隙位置关系 同节段患侧与健侧相比,Q点分别至同序数腰椎对侧椎弓根下缘、下位腰椎对侧椎弓根上缘、同序数腰椎下终板、下位腰椎上终板垂直距离以及导棒外展角度差异无显著性意义(P > 0.05);L4/5患侧和L5S1患侧相比,Q点至同序数腰椎对侧椎弓根下缘、下位腰椎对侧椎弓根上缘、同序数腰椎下终板、下位腰椎上终板垂直距离以及导棒外展角度差异有显著性意义(P < 0.05),见表2。"
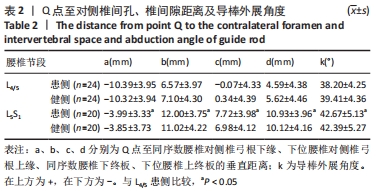
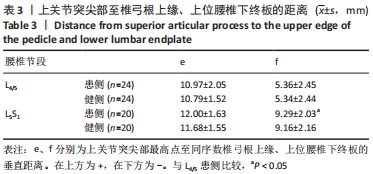
2.3.4 上关节突尖部与椎间孔、椎间隙位置关系 同节段患侧与健侧相比,上关节突尖部最高点至同序数椎弓根上缘、上位腰椎下终板垂直距离差异无显著性意义(P > 0.05);L4/5患侧和L5S1患侧相比,上关节突尖部最高点至同序数椎弓根上缘垂直距离差异无显著性意义(P > 0.05),上关节突尖部最高点至上位腰椎下终板垂直距离差异有显著性意义(P < 0.05),见表3。"
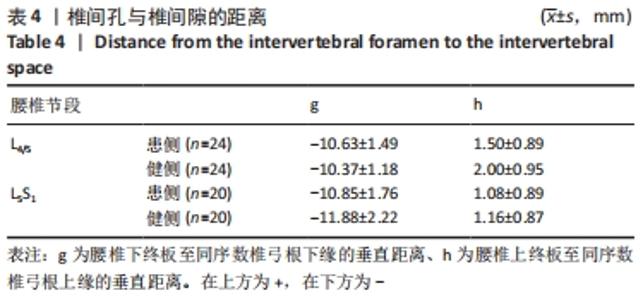
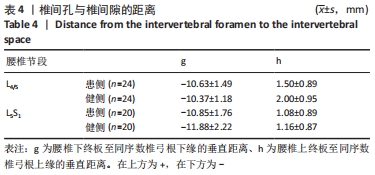
2.3.5 椎间孔与椎间隙位置关系 同节段患侧与健侧相比,腰椎下终板至同序数椎弓根下缘、腰椎上终板至同序数椎弓根上缘垂直距离差异无显著性意义(P > 0.05);L4/5患侧和L5S1患侧相比,腰椎下终板至同序数椎弓根下缘、腰椎上终板至同序数椎弓根上缘垂直距离差异无显著性意义(P > 0.05),见表4。"
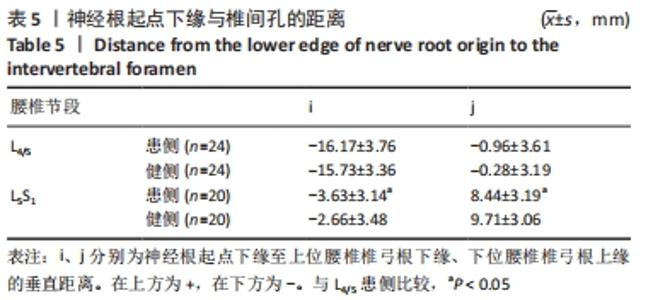
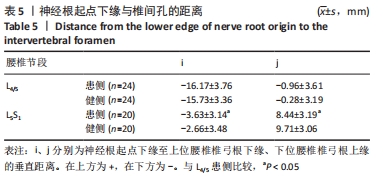
2.3.6 神经根起点下缘与椎间孔位置关系 同节段患侧与健侧相比,神经根起点下缘至上位腰椎椎弓根下缘、下位腰椎椎弓根上缘垂直距离差异无显著性意义(P > 0.05);L4/5患侧和L5S1患侧相比,神经根起点下缘至上位腰椎椎弓根下缘、下位腰椎椎弓根上缘垂直距离差异有显著性意义(P < 0.05),见表5。"
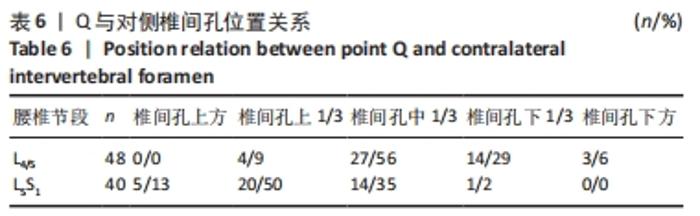
2.3.7 Q、神经根起点下缘与对侧椎间孔位置关系 Q点投影至对侧椎间孔位置:在L4/5节段,Q点大多投影于对侧椎间孔中1/3水平,占比56%(27/48),其次投影于对侧椎间孔下1/3水平,占比29%(14/48);L5S1节段,Q点大多数投影于椎间孔上1/3水平,占比50%(20/40),见表6。"

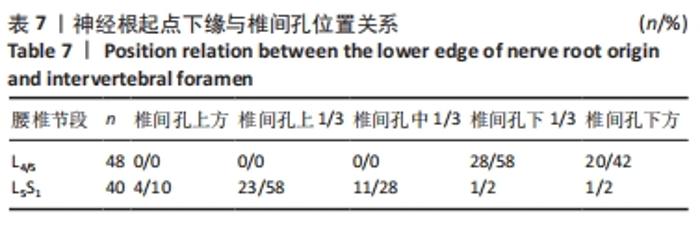
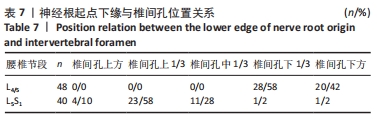
在L4/5节段,L5神经根起点下缘大多投影于椎间孔下1/3水平,占比58%(28/48),其次均位于椎间孔水平下方,距离L5椎弓根上缘(-0.96±3.61) mm。而在L5S1节段,S1神经根起点下缘大多数投于影椎间孔上1/3水平,占比58%(23/40),见表7。在L4/5和L5S1节段,其椎间隙位置均投影于同节段椎间孔下1/3水平附近。 "
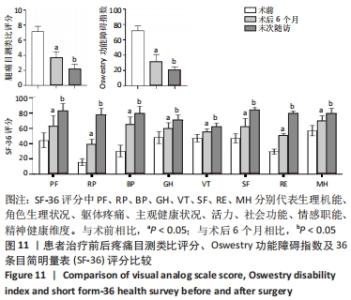
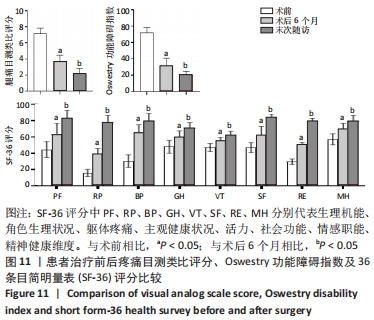
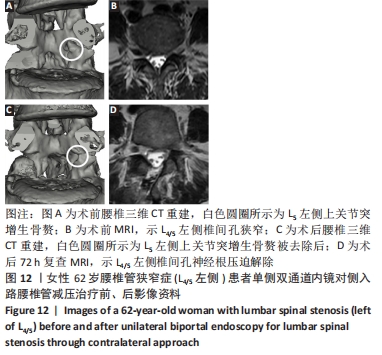
2.4 疗效评价 7例对侧入路手术患者均顺利完成手术,术中均未转为开放手术,术后未出现硬脊膜血肿及神经组织损伤。随访以疼痛目测类比评分、Oswestry功能障碍指数、SF-36评分综合评估,所有患者均得到有效随访,随访时间6-12个月。随着术后康复时间延长,目测类比评分、Oswestry功能障碍指数较术前显著降低,SF-36评分较术前显著改善,不同随访时间点间差异均有显著性意义(P < 0.05),见图11。典型病例资料见图12。"

"
| [1] 林博颖,沈茂.内镜下腰椎椎间融合:单侧椎弓根螺钉联合对侧椎板关节突螺钉固定的生物力学稳定性[J].中国组织工程研究,2022, 26(3):329-333. [2] ARABMOTLAGH M, SELLEI RM, VINAS-RIOS JM, et al. Classification and diagnosis of lumbar spinal stenosis. Orthopade. 2019;48(10):816-823. [3] LAI MKL, CHEUNG PWH, CHEUNG JPY. A systematic review of developmental lumbar spinal stenosis. Eur Spine J. 2020;29(9):2173-2187. [4] LU HG, PAN XK, HU MJ, et al. Percutaneous Transforaminal Endoscopic Decompression for Lumbar Lateral Recess Stenosis. Front Surg. 2021;8: 631419. [5] BURKHARDT BW, OERTEL JM. Is Decompression and Partial Discectomy Advantageous Over Decompression Alone in Microendoscopic Decompression Of Monosegmental Unilateral Lumbar Recess Stenosis? Int J Spine Surg. 2021;15(1):94-104. [6] WANG Y, DENG M, WU H, et al. Short-term effectiveness of precise safety decompression via double percutaneous lumbar foraminoplasty and percutaneous endoscopic lumbar decompression for lateral lumbar spinal canal stenosis: a prospective cohort study. BMC Musculoskelet Disord. 2021;22(1):80. [7] WILTSE LL, SPENCER CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988;13(6):696-706. [8] YANG CC, YEH KT, LIU KC, et al. Ameliorated Full-Endoscopic Transforaminal Decompression for L5-S1 Foraminal and Extraforaminal Stenosis. Clin Spine Surg. 2021;34(6):197-205. [9] 毕经纬,李瑞,孙宁,等.单侧双通道内镜与椎间孔镜治疗腰椎管狭窄症的比较[J].中国微创外科杂志,2022,22(2):102-107. [10] 田大胜,刘建军,朱斌,等.单边双通道内镜技术治疗腰椎间盘突出症和腰椎椎管狭窄症[J].中华骨科杂志,2020,40(17):1155-1164. [11] LEE HG, KANG MS, KIM SY, et al. Dural Injury in Unilateral Biportal Endoscopic Spinal Surgery. Global Spine J. 2021;11(6):845-851. [12] GATAM AR, GATAM L, MAHADHIPTA H, et al. Unilateral Biportal Endoscopic Lumbar Interbody Fusion: A Technical Note and an Outcome Comparison with the Conventional Minimally Invasive Fusion. Orthop Res Rev. 2021;13:229-239. [13] JIANG HW, CHEN CD, ZHAN BS, et al. Unilateral biportal endoscopic discectomy versus percutaneous endoscopic lumbar discectomy in the treatment of lumbar disc herniation: a retrospective study. J Orthop Surg Res. 2022;17(1):30. [14] KIM JY, KIM HS, JEON JB, et al. The Novel Technique of Uniportal Endoscopic Interlaminar Contralateral Approach for Coexisting L5-S1 Lateral Recess, Foraminal, and Extraforaminal Stenosis and Its Clinical Outcomes. J Clin Med. 2021;10(7):1364. [15] JHA RT, SYED HR, CATALINO M, et al. Contralateral Approach for Minimally Invasive Treatment of Upper Lumbar Intervertebral Disc Herniation: Technical Note and Case Series. World Neurosurg. 2017; 100:583-589. [16] HWANG JH, PARK WM, PARK CW. Contralateral Interlaminar Keyhole Percutaneous Endoscopic Lumbar Surgery in Patients with Unilateral Radiculopathy. World Neurosurg. 2017;101:33-41. [17] HUA W, WANG B, KE W, et al. Comparison of lumbar endoscopic unilateral laminotomy bilateral decompression and minimally invasive surgery transforaminal lumbar interbody fusion for one-level lumbar spinal stenosis. BMC Musculoskelet Disord. 2020;21(1):785. [18] HUA W, WANG B, KE W, et al. Comparison of Clinical Outcomes Following Lumbar Endoscopic Unilateral Laminotomy Bilateral Decompression and Minimally Invasive Transforaminal Lumbar Interbody Fusion for One-Level Lumbar Spinal Stenosis With Degenerative Spondylolisthesis. Front Surg. 2021;7:596327. [19] AKBARY K, KIM JS, PARK CW, et al. Biportal Endoscopic Decompression of Exiting and Traversing Nerve Roots Through a Single Interlaminar Window Using a Contralateral Approach: Technical Feasibilities and Morphometric Changes of the Lumbar Canal and Foramen. World Neurosurg. 2018;117:153-161. [20] ALIMI M, NJOKU IJR, CONG GT, et al. Minimally invasive foraminotomy through tubular retractors via a contralateral approach in patients with unilateral radiculopathy. Neurosurgery. 2014;10 Suppl 3:436-447. [21] KHALSA SS, KIM HS, SINGH R, et al. Radiographic outcomes of endoscopic decompression for lumbar spinal stenosis. Neurosurg Focus. 2019;46(5):E10. [22] 刘金玉,丁宇,蒋强,等. 全内镜下腰椎板开窗减压有限元模拟建模及生物力学变化[J]. 中国组织工程研究,2020,24(27): 4291-4296. [23] KIM J, HEO DH, LEE DC, et al. Biportal endoscopic unilateral laminotomy with bilateral decompression for the treatment of cervical spondylotic myelopathy. Acta Neurochir (Wien). 2021;163(9):2537-2543. [24] KIM JS, PARK CW, YEUNG YK, et al. Unilateral Bi-portal Endoscopic Decompression via the Contralateral Approach in Asymmetric Spinal Stenosis: A Technical Note. Asian Spine J. 2021;15(5):688-700. [25] AKBARY K, KIM JS, PARK CW, et al. Biportal Endoscopic Decompression of Exiting and Traversing Nerve Roots Through a Single Interlaminar Window Using a Contralateral Approach: Technical Feasibilities and Morphometric Changes of the Lumbar Canal and Foramen. World Neurosurg. 2018;117:153-161. [26] KIM HS, PATEL R, PAUDEL B, et al. Early Outcomes of Endoscopic Contralateral Foraminal and Lateral Recess Decompression via an Interlaminar Approach in Patients with Unilateral Radiculopathy from Unilateral Foraminal Stenosis. World Neurosurg. 2017;108: 763-773. [27] HEO DH, KIM JS, PARK CW, et al. Contralateral Sublaminar Endoscopic Approach for Removal of Lumbar Juxtafacet Cysts Using Percutaneous Biportal Endoscopic Surgery: Technical Report and Preliminary Results. World Neurosurg. 2019;122:474-479. [28] KIM JY, HEO DH. Contralateral sublaminar approach for decompression of the combined lateral recess, foraminal, and extraforaminal lesions using biportal endoscopy: a technical report. Acta Neurochir (Wien). 2021;163(10):2783-2787. [29] CHOI CM, CHUNG JT, LEE SJ, et al. How I do it? Biportal endoscopic spinal surgery (BESS) for treatment of lumbar spinal stenosis. Acta Neurochir (Wien). 2016;158(3):459-463. [30] RHEE J, ANAIZI AN, SANDHU FA, et al. Minimally invasive resection of lumbar synovial cysts from a contralateral approach. J Neurosurg Spine. 2012;17(5):453-458. [31] HWANG JH, PARK WM, PARK CW. Contralateral Interlaminar Keyhole Percutaneous Endoscopic Lumbar Surgery in Patients with Unilateral Radiculopathy. World Neurosurg. 2017;101:33-41. [32] KIM HS, SINGH R, ADSUL NM, et al. Management of Root-Level Double Crush: Case Report with Technical Notes on Contralateral Interlaminar Foraminotomy with Full Endoscopic Uniportal Approach. World Neurosurg. 2019;122:505-507. [33] CHAU AM, PELZER NR, HAMPTON J, et al. Lateral extent and ventral laminar attachments of the lumbar ligamentum flavum: cadaveric study. Spine J. 2014;14(10):2467-2471. [34] PENG YX, ZHENG ZY, WANG MD WG, et al. Relationship between the location of ligamentum flavum hypertrophy and its stress in finite element analysis. Orthop Surg. 2020;12(3):974-982. |
| [1] | Li Jinglian, Zhang Hongfei, Yan Jiapeng, Zhou Jiabin, Yu Hao. Lag screw path for fixation of sacroiliac joint dislocation through S1 pedicle [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(15): 2337-2341. |
| [2] | Gu Yueguang, Shen Jianhuan, Ni Jieli, Guo Shuyu, Yan Zhongyi, Zhang Yang. Effect of osteogenesis in patients with alveolar cleft after bone grafting investigated by volume analysis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(10): 1501-1504. |
| [3] | Yao Rubin, Wang Shiyong, Yang Kaishun. Minimally invasive transforaminal lumbar interbody fusion for treatment of single-segment lumbar spinal stenosis improves lumbar-pelvic balance [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1387-1392. |
| [4] | Tian Yang, Tang Chao, Liao Yehui, Tang Qiang, Ma Fei, Zhong Dejun. Consistency and repeatability of CT and MRI in measurement of spinal canal area in patients with lumbar spinal stenosis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3882-3887. |
| [5] | Lin Tianye, Yang Peng, Xiong Binglang, He Xiaoming, Yan Xinhao, Zhang Jin, He Wei, Wei Qiushi . Comparison of preoperative three-dimensional reconstruction simulation and intraoperative drawing of femoral osteotomy to measure rotation angle in vitro [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(21): 3349-3353. |
| [6] | Li Yuefei, Li Rui, Ren Jiabin, Liu Xin, Sun Ning, Liu Weike, Bi Jingwei, Sun Zhaozhong. Three-dimensional CT analysis of the treatment of thoracic disc herniation by percutaneous endoscopic posterolateral approach: establishment of a good osseous channel [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(21): 3354-3359. |
| [7] | Wang Jing, Xu Shuai, Liu Haiying. Hidden blood loss during posterior lumbar interbody fusion in lumbar spinal stenosis patients with and without rheumatoid arthritis [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(33): 5307-5314. |
| [8] | Li Xuxiang, Zhang Huikang, Wei Bo, Yao Qingqiang, Xu Yan, Tang Cheng, Wang Liming. Application of personalized osteotomy guide plate in medial pivot knee prosthesis replacement based on MRI and three-dimensional CT [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(30): 4835-4840. |
| [9] | Zhang Chunlin, Shang Lijie, Yan Xu, Cao Zhengming, Shao Chenglong, Feng Yang. Mid-long-term effect of only placed expandable interbody fusion cage in the treatment of lumbar spinal stenosis with vertebral instability using micro-endoscopic discectomy system [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(3): 335-341. |
| [10] | Liu Jinyu, Ding Yu, Jiang Qiang, Cui Hongpeng, Lu Zhengcao. A finite element model of full endoscope lumbar fenestration and biomechanical characteristics [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(27): 4291-4296. |
| [11] | Zhang Junwei, Cui Yutao, Li Zuhao, Wang Zhonghan, Liu He, Luo Wenbin. Application of bioprinting in reconstruction of musculoskeletal interface [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(16): 2585-2591. |
| [12] | Zhang Shuai, Wang Gaoju, Wang Qing. Relationship between thoracic and lumbar vertebral posterior wall morphology and bone cement leakage into the spinal canal during the percutaneous kyphoplasty [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(10): 1477-1483. |
| [13] | He Da, Zhao Jingwei, Liu Bo, Tian Wei. Comparison of limited fusion and full curve fusion for mild lumbar degenerative scoliosis with stenosis [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(36): 5811-5817. |
| [14] |
Rong Feilong, Yin Ruofeng, Feng Mengmeng, Zhang Boyin, Liu Yi, Zhao Baolin.
Correlation between degenerative lumbar spondylolisthesis and spinal stenosis and muscle volume around the vertebral body: CT and MRI data analysis
[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(24): 3840-3845.
|
| [15] |
Huang Guangxi, Liu Yan, Chen Wenzhi.
Degenerative changes of lumbar facet joint in patients with lumbar spinal stenosis by MRI
[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(24): 3852-3856.
|
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||