Chinese Journal of Tissue Engineering Research ›› 2021, Vol. 25 ›› Issue (21): 3354-3359.doi: 10.3969/j.issn.2095-4344.3855
Previous Articles Next Articles
Three-dimensional CT analysis of the treatment of thoracic disc herniation by percutaneous endoscopic posterolateral approach: establishment of a good osseous channel
Li Yuefei1, Li Rui1, Ren Jiabin1, Liu Xin1, Sun Ning1, Liu Weike2, Bi Jingwei1, Sun Zhaozhong1
- 1Department of Spinal Surgery, Binzhou Medical University Hospital, Binzhou 256603, Shandong Province, China; 2Department of Orthopedics, Binzhou Hospital of Traditional Chinese Medicine, Binzhou 256600, Shandong Province, China
-
Received:2020-08-25Revised:2020-08-28Accepted:2020-10-09Online:2021-07-28Published:2021-01-23 -
Contact:Sun Zhaozhong, Chief physician, Professor, Department of Spinal Surgery, Binzhou Medical University Hospital, Binzhou 256603, Shandong Province, China -
About author:Li Yuefei, Master candidate, Department of Spinal Surgery, Binzhou Medical University Hospital, Binzhou 256603, Shandong Province, China
CLC Number:
Cite this article
Li Yuefei, Li Rui, Ren Jiabin, Liu Xin, Sun Ning, Liu Weike, Bi Jingwei, Sun Zhaozhong. Three-dimensional CT analysis of the treatment of thoracic disc herniation by percutaneous endoscopic posterolateral approach: establishment of a good osseous channel[J]. Chinese Journal of Tissue Engineering Research, 2021, 25(21): 3354-3359.
share this article
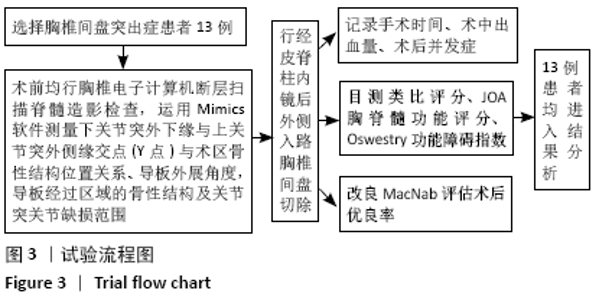
2.1 参与者数量分析 13例患者均进入结果分析。 2.2 试验流程 见图3。"

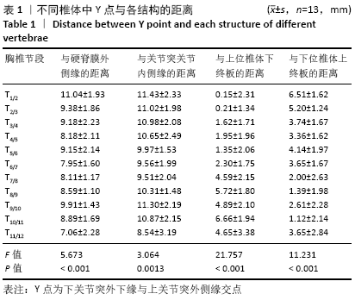
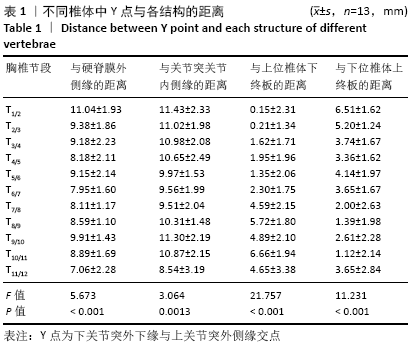
2.3 胸椎3D-CT测量结果 T1/2椎体Y点与上位椎体下终板的距离为(0.15±2.31) mm,T1/2椎体Y点与下位椎体上终板的距离为(6.51±1.62) mm,在矢状面上Y点投影在椎间隙上方;其余节段Y点与上位椎体下终板的距离为(0.21±1.34)-(6.66±1.94) mm,Y点与下位椎体上终板的距离为(1.12±2.14)-(5.20±1.24) mm,在矢状面上Y点投影在椎间隙水平(表1)。"
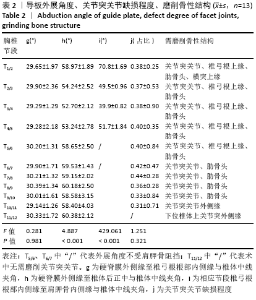
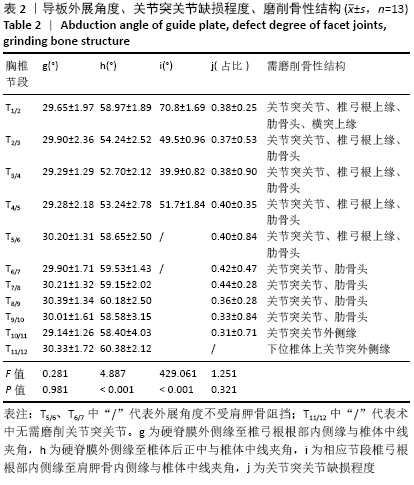
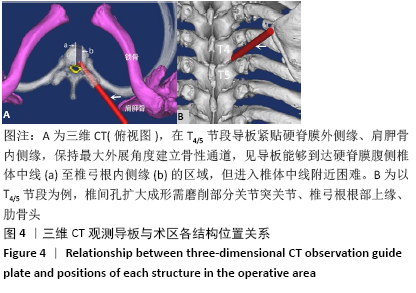
T1/2椎体h<i,导板外展时无肩胛骨阻挡;T2/3-T4/5椎体h>i,导板外展时被肩胛骨阻挡(表2)。在软件三维视图中,T1/2-T11/12节段导板通过部分关节突关节、椎弓根、肋骨头等骨性结构(表2、图4)。"

"
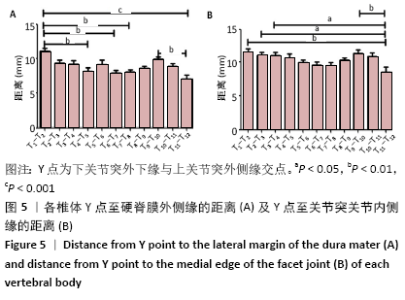
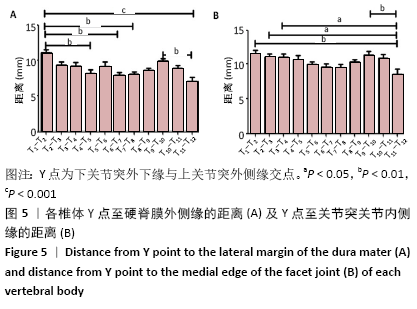
2.4 胸椎3D-CT测量结果 采用Graphpad prism 5统计各数据后只有a,b有规律性,可用于指导临床研究,其余数据没有明显规律性,对于指导临床十分有限,没有纳入结果分析。T2/3-T10/11椎体间Y点至硬脊膜外侧缘的距离比较差异无显著性意义(P > 0.05),T1/2与T4/5、T1/2与T6/7、T1/2与T7/8、T1/2与T11/12、T9/10与T11/12椎体间Y点至硬脊膜外侧缘的距离比较差异均无显著性意义(P > 0.05),T1/2-T10/11椎体间Y点至关节突 关节内侧缘的距离比较差异均无显著性意义(P > 0.05),T11/12与T1/2-T3/4、T9/10椎体间Y点至关节突关节内侧缘的距离比较差异有显著性意义(P < 0.05),见图5。 "

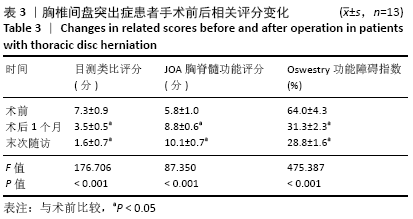
2.5 术中与术后随访相关指标 13例患者均顺利完成手术,未发生硬脊膜撕裂及胸髓、胸神经、大血管、胸膜腔损伤,术后未发生切口感染、脑脊液漏、双下肢深静脉血栓及二次翻修手术。手术时间35-130 min,平均(66.2±33.1) min。术中出血量10-40 mL。术后1例患者出现右下肢无力症状加重,术前双下肢肌力Ⅳ级,术后即出现左下肢肌力Ⅴ级、右下肢肌力Ⅲ级,术后1个月右下肢肌力恢复至Ⅴ级。随访时间6-27个月,平均17.0个月,随访期间所有患者均无疼痛、麻木、无力等症状加重情况。术后1个月、末次随访的目测类比评分、JOA胸脊髓功能评分、Oswestry功能障碍指数评分均较术前差明显改善(P < 0.05),见表3。末次随访时运用改良MacNab疗效评定疗效,优8例,良4例,可1例,无疗效“差”患者,优良率为92%。 "

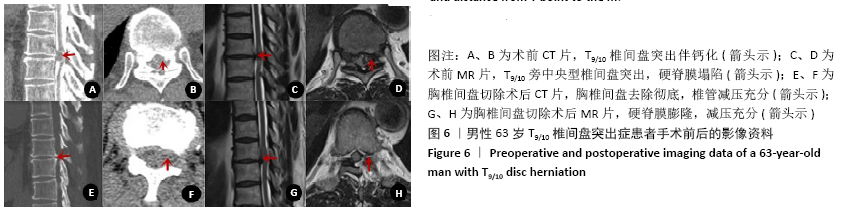
2.6 典型病例 63岁男性患者,双下肢无力4年加重6个月,诊断为T9/10椎间盘突出症,行经皮脊柱内镜后外侧入路胸椎间盘切除手术前后的影像资料,见图6。"
| [1] OLTULU I, CIL H, ULU MO, et al. Clinical outcomes of symptomatic thoracic disk herniations treated surgically through minimally invasive lateral transthoracic approach. Neurosurg Rev. 2019;42(4):885-894. [2] WOOD KB, GARVEY TA, GUNDRY C, et al. Magnetic resonance imaging of the thoracic spine. Evaluation of asymptomatic individuals. J Bone Joint Surg Am. 1995;77:1631-1638. [3] ROELZ R, SCHOLZ C, KLINGLER JH, et al. Giant central thoracic disc herniations: surgical outcome in 17 consecutive patients treated by mini-thoracotomy. Eur Spine J. 2016;25:1443-1451. [4] DALBAYRAK S, YAMAN O, OZTÜRK K, et al. Transforaminal approach in thoracal disc pathologies: transforaminal microdiscectomy technique. Minim Invasive Surg. 2014;2014:301945. [5] STILLERMAN CB, CHEN TC, COULDWELL WT, et al. Experience in the surgical management of 82 symptomatic herniated thoracic discs and review of the literature. J Neurosurg. 1998;88(4):623-633. [6] XIAOBING Z, XINGCHEN L, HONGGANG Z, et al. “U” route transforaminal percutaneous endoscopic thoracic discectomy as a new treatment for thoracic spinal stenosis. Int Orthop. 2019;43(4):825-832. [7] ROSS JS, PEREZ-REYES N, MASARYK TJ, et al. Thoracic disk herniation: MR imaging. Radiology. 1987;165(2):511-515. [8] Rogers MA, Crockard HA. Surgical treatment of the symptomatic herniated thoracic disk. Clin Orthop Relat Res. 1994;300:70-78. [9] WAGNER R, TELFEIAN AE, IPRENBURG M, et al. Transforaminal Endoscopic Foraminoplasty and Discectomy for the Treatment of a Thoracic Disc Herniation. World Neurosurg. 2016;90:194-198. [10] OPPENLANDER ME, CLARK JC, KALYVAS J, et al. Surgical management and clinical outcomes of multiple- level symptomatic herniated thoracic discs. J Neurosurg Spine. 2013;19(6):774-783. [11] LUBELSKI D, ABDULLAH KG, STEINMETZ MP, et al. Lateral extracavitary, costotransversectomy,and transthoracic thoracotomy approaches to the thoracic spine:review of techniques and complications. J Spinal Disord Tech. 2013;26(4):222-232. [12] ZHAO Y, WANG Y, XIAO S, et al. Transthoracic approach for the treatment of calcified giant herniated thoracic discs. Eur Spine J. 2013;22(11):2466-2473. [13] HUR JW, KIM JS, SEUNG JH. Full-endoscopic interlaminar discectomy for the treatment of a dorsal migrated thoracic disc herniation: Case report. Medicine (Baltimore). 2019;98(22):e15541. [14] DEVIREN V, KUELLING FA, POULTER G, et al. Minimal invasive anterolateral transthoracic transpleural approach:a novel technique for thoracic disc herniation. A review of the literature,description of a new surgical technique and experience with first 12 consecutive patients. J Spinal Disord Tech. 2011;24(5):E40-E48. [15] ROSENTHAL D. Endoscopic approaches to the thoracic spine. Eur Spine J. 2000;9 (Suppl 1):S8-S16. [16] WAIT SD, FOX DJ JR, KENNY KJ, et al. Thoracoscopic resection of symptomatic herniated thoracic discs: clinical results in 121 patients. Spine (Phila Pa 1976). 2012;37:35-40. [17] 杨俊松,楚磊,王永峰,等.经皮脊柱内镜在治疗胸椎管狭窄症中的应用研究[J].中国骨与关节杂志,2019,8(2):98-104. [18] 刘越,徐宝山,吉宁,等.经皮椎间孔镜技术治疗胸椎间盘突出症的初步体会[J].天津医药,2017,45(2):121-124. [19] BARTELS RH, PEUL WC. Mini-thoracotomy or thoracoscopic treatment for medially located thoracic herniated disc? Spine (Phila Pa 1976). 2007; 32:E581-E584. [20] BILSKY MH. Transpedicular approach for thoracic disc herniations. Neurosurg Focus. 2000;9(4):e3. [21] FESSLER RG, STURGILL M. Review: complications of surgery for thoracic disc disease. Surg Neurol. 1998;49:609-618. [22] YOSHIHARA H, YONEOKA D. Comparison of in-hospital morbidity and mortality rates between anterior and nonanterior approach procedures for thoracic disc herniation. Spine (PhilaPa 1976). 2014;39:E728-E733. [23] RUETTEN S, HAHN P, OEZDEMIR S, et al. Full-endoscopic uniportal decompression in disc herniations and stenosis of the thoracic spine using the interlaminar,extraforaminal,or transthoracic retropleural approach. J Neurosurg Spine. 2018;29(2):157-168. [24] Jho HD. Endoscopic microscopic transpedicular thoracic discectomy: Technical note. J Neurosurg. 1997;87(1):125-129. [25] BAE J, CHACHAN S, SHIN SH, et al. Percutaneous Endoscopic Thoracic Discectomy in the Upper and Midthoracic Spine: A Technical Note. Neurospine. 2019;16(1):148-153. [26] RUETTEN S, HAHN P, OEZDEMIR S, et al. Operation of Soft or Calcified Thoracic Disc Herniations in the Full-Endoscopic Uniportal Extraforaminal Technique. Pain Physician. 2018;21(4):E331-E340. [27] LIU W, YAO L, LI X, et al. Percutaneous endoscopic thoracic discectomy via posterolateral approach: A case report of migrated thoracic disc herniation. Medicine(Baltimore). 2019;98(41):e17579. [28] CHOI KY, EUN SS, LEE SH, et al. Percutaneous endoscopic thoracic discectomy; transforaminal approach. Minim Invasive Neurosurg. 2010;53:25-28. [29] YEUNG AT, TSOU PM. Posterolateral endoscop-icexcision for lumbar disc herniation:Surgical tech- Nique,outcome,and complications in 307 consecutive cases. Spine (Phila Pa 1976). 2002;27(7):722-731. [30] HOOGLAND T, SCHUBERT M, MIKLITZ B, et al. Transfo-raminal posterolateral endoscopic dis-cectomy with or without the combination of a low-dose chymopa-pain:a prospective randomized study in 280 consecutive cases. Spine (Phila Pa 1976). 2006;31(24):890-897. [31] 袁恒,张西峰,张琳,等.脊柱内镜下治疗胸腰段椎间盘突出的临床疗效[J].实用骨科杂志,2018,24(8):733-736. [32] AN B, LI XC, ZHOU CP, et al. Percutaneous full endoscopic posterior decompression of thoracic myelopathy caused by ossification of the ligamentum flavum. Eur Spine J. 2019;28(3):492-501. [33] DEBNATH UK, MCCONNELL JR, SENGUPTA DK, et al. Results of hemivertebrectomy and fusion for symptomatic thoracic disc herniation. Eur Spine J. 2003;12:292-299. [34] ODA I, ABUMI K, LÜ D, et al. Biomechanical role of the posterior elements, costovertebral joints, and rib cage in the stability of the thoracic spine. Spine (Phila Pa 1976). 1996;21:1423-1429. [35] AL-MAHFOUDH R, MITCHELL PS, WILBY M, et al. Management of Giant Calcified Thoracic Disks and Description of the Trench Vertebrectomy Technique. Global Spine J. 2016;6(6):584-591. |
| [1] | Xu Feng, Kang Hui, Wei Tanjun, Xi Jintao. Biomechanical analysis of different fixation methods of pedicle screws for thoracolumbar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1313-1317. |
| [2] | Jiang Yong, Luo Yi, Ding Yongli, Zhou Yong, Min Li, Tang Fan, Zhang Wenli, Duan Hong, Tu Chongqi. Von Mises stress on the influence of pelvic stability by precise sacral resection and clinical validation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1318-1323. |
| [3] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [4] | Zhang Yu, Tian Shaoqi, Zeng Guobo, Hu Chuan. Risk factors for myocardial infarction following primary total joint arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1340-1345. |
| [5] | Wei Wei, Li Jian, Huang Linhai, Lan Mindong, Lu Xianwei, Huang Shaodong. Factors affecting fall fear in the first movement of elderly patients after total knee or hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1351-1355. |
| [6] | Wang Jinjun, Deng Zengfa, Liu Kang, He Zhiyong, Yu Xinping, Liang Jianji, Li Chen, Guo Zhouyang. Hemostatic effect and safety of intravenous drip of tranexamic acid combined with topical application of cocktail containing tranexamic acid in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1356-1361. |
| [7] | Xiao Guoqing, Liu Xuanze, Yan Yuhao, Zhong Xihong. Influencing factors of knee flexion limitation after total knee arthroplasty with posterior stabilized prostheses [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1362-1367. |
| [8] | Huang Zexiao, Yang Mei, Lin Shiwei, He Heyu. Correlation between the level of serum n-3 polyunsaturated fatty acids and quadriceps weakness in the early stage after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1375-1380. |
| [9] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [10] | Wang Haiying, Lü Bing, Li Hui, Wang Shunyi. Posterior lumbar interbody fusion for degenerative lumbar spondylolisthesis: prediction of functional prognosis of patients based on spinopelvic parameters [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1393-1397. |
| [11] | Lü Zhen, Bai Jinzhu. A prospective study on the application of staged lumbar motion chain rehabilitation based on McKenzie’s technique after lumbar percutaneous transforaminal endoscopic discectomy [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1398-1403. |
| [12] | Chen Xinmin, Li Wenbiao, Xiong Kaikai, Xiong Xiaoyan, Zheng Liqin, Li Musheng, Zheng Yongze, Lin Ziling. Type A3.3 femoral intertrochanteric fracture with augmented proximal femoral nail anti-rotation in the elderly: finite element analysis of the optimal amount of bone cement [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1404-1409. |
| [13] | Du Xiupeng, Yang Zhaohui. Effect of degree of initial deformity of impacted femoral neck fractures under 65 years of age on femoral neck shortening [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1410-1416. |
| [14] | Zhang Shangpu, Ju Xiaodong, Song Hengyi, Dong Zhi, Wang Chen, Sun Guodong. Arthroscopic suture bridge technique with suture anchor in the treatment of acromioclavicular dislocation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1417-1422. |
| [15] | Liang Yan, Zhao Yongfei, Xu Shuai, Zhu Zhenqi, Wang Kaifeng, Liu Haiying, Mao Keya. Imaging evaluation of short-segment fixation and fusion for degenerative lumbar scoliosis assisted by highly selective nerve root block [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1423-1427. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||