Chinese Journal of Tissue Engineering Research ›› 2026, Vol. 30 ›› Issue (34): 9056-9066.doi: 10.12307/2026.868
Previous Articles Next Articles
Different physical factor therapies for knee osteoarthritis: a network meta-analysis of efficacy and safety
Wu Ruiqi1, 2, Dong Panfeng1, Zhang Hongrui1, 2, Lyu Yongbin1, 2, Peng Qinglin1, Zhuo Yinghong1, Chen Yueping1
- 1Affiliated Ruikang Hospital of Guangxi University of Chinese Medicine, Nanning 530000, Guangxi Zhuang Autonomous Region, China; 2Guangxi University of Chinese Medicine, Nanning 530299, Guangxi Zhuang Autonomous Region, China
-
Received:2025-11-19Revised:2026-01-23Online:2026-12-08Published:2026-04-15 -
Contact:Dong Panfeng, MS, Associate chief physician, Associate professor, Master’s supervisor, Affiliated Ruikang Hospital of Guangxi University of Chinese Medicine, Nanning 530000, Guangxi Zhuang Autonomous Region, China -
About author:Wu Ruiqi, PhD candidate, Affiliated Ruikang Hospital of Guangxi University of Chinese Medicine, Nanning 530000, Guangxi Zhuang Autonomous Region, China; Guangxi University of Chinese Medicine, Nanning 530299, Guangxi Zhuang Autonomous Region, China Corresponding author: Chen Yueping, PhD, Chief physician, Doctoral supervisor, Affiliated Ruikang Hospital of Guangxi University of Chinese Medicine, Nanning 530000, Guangxi Zhuang Autonomous Region, China -
Supported by:Department of Orthopedics and Traumatology, Ruikang Hospital Affiliated to Guangxi University of Chinese Medicine, a National Flagship Department for the Integration of Chinese and Western Medicine (to CYP); Guangxi Natural Science Foundation, No. 2023JJA140318 (to CYP); Guangxi Natural Science Foundation, No. 502189963012 (to DPF); Graduate Education Innovation Program of Guangxi University of Chinese Medicine, No. YCBXJ2025029 (to WRQ); Class A Project of the Guipai Traditional Chinese Medicine Inheritance and Innovation Team, Guangxi University of Chinese Medicine, No. 2022A004 (to CYP)
CLC Number:
Cite this article
Wu Ruiqi, Dong Panfeng, Zhang Hongrui, Lyu Yongbin, Peng Qinglin, Zhuo Yinghong, Chen Yueping . Different physical factor therapies for knee osteoarthritis: a network meta-analysis of efficacy and safety[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(34): 9056-9066.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
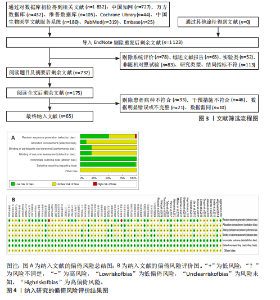
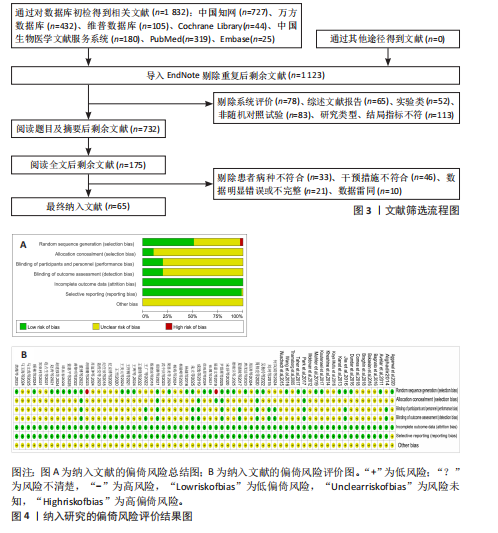
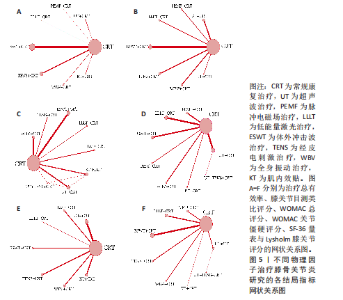
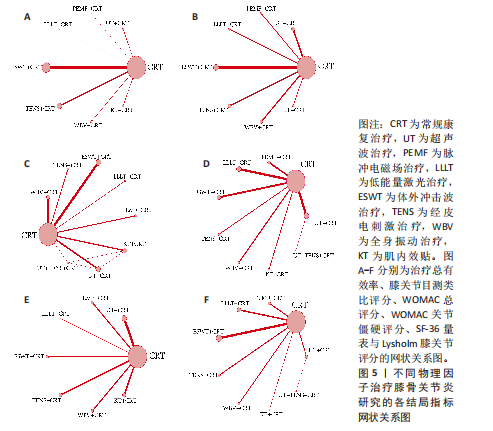
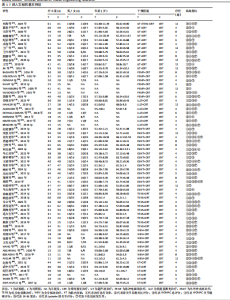
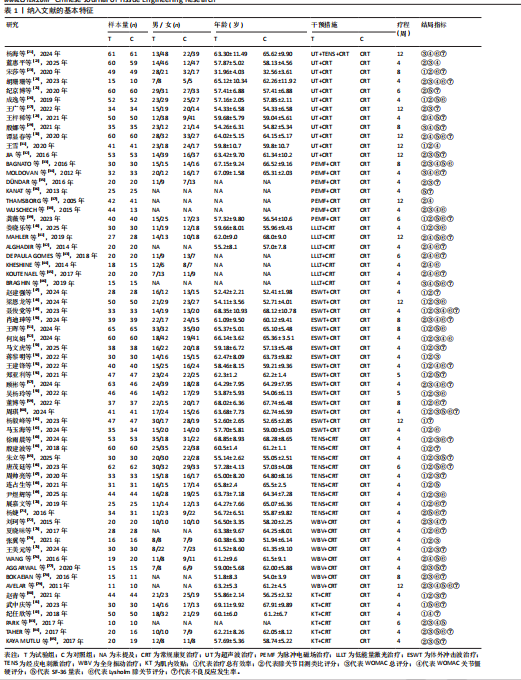
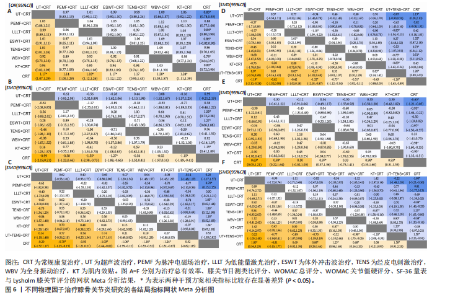
2.1 文献检索结果 初步搜索获得1 832篇文献,通过EndNote X9自动结合手动剔除重复文献后剩余1 123篇,阅读标题和摘要后排除一些不相关且明显不符合纳入要求的文章,如动物细胞实验、手术相关研究、病例报告和综述等,下载了175篇文献以供进一步筛选。通过阅读全文,排除不符合纳入标准的文献,最终纳入65个随机对照试验。文献筛选流程见图3。 2.2 纳入文献的基本特征 共纳入3 418例患者,均符合膝骨关节炎的临床诊断,其中治疗组1 726例、对照组1 692例,入选患者年龄40-75岁,其中55-70岁最常见。使用常规康复治疗作为对照组,包括常规的关节活动度训练、肌力训练、日常功能训练及一般护理指导等,试验组为常规康复治疗联合物理因子治疗,涉及超声波、脉冲电磁场、低能量激光、体外冲击波、经皮电刺激、全身振动和肌内效贴7种物理因子治疗,治疗持续时间为4-12周。结局指标方面,报道治疗总有效率的共有33项研究、膝关节目测类比评分的共有57项研究、WOMAC总评分的共有35项研究、WOMAC关节僵硬评分的共有29项研究,SF-36量表的24项研究、Lysholm膝关节评分的共有39项研究。纳入文献的基本特征,见表1。 2.3 纳入文献的质量评价 纳入65篇文献均为随机对照试验[21-85]。随机顺序产生方面,29项为随机数字表法[22-23,28-30,32,35,39-41,45,48,57-59,63,65-67,69,71,74-77,79-80,83-84],2项采用抽签随机法[51,54],1项采用分层区组随机[69],以上研究均判为“低风险”,1项根据治疗方案的不同进行分组[36],2项按照患者采用就诊先后顺序[24,70],均判为“高风险”,其余研究未报告具体随机方法判为“风险未知”。分配隐藏方面,7项研究采用信封法进行分配隐藏[26,59,29,67,69-70,83],判为“低风险”,其余研究均未提及分配隐藏方案,评为“风险未知”。盲法方面,13项研究采用双盲[27,29,32,39,42,52,59,65,67,69,72-73,83],均判为“低风险”, 其余研究均未提及盲法判为“风险未知”。纳入研究数据完整,结局评价可靠,评为“低风险”。在选择性报告方面,均未在中国临床试验注册中心上搜索到研究计划书均评为“风险未知”。在其他来源偏倚风险方面,所有研究对资助来源等方面未报告均评为“风险未知”。采用RevMan 5.3软件绘制纳入研究的偏倚风险图,见图4。 2.4 治疗总有效率分析结果 2.4.1 证据网络 33项随机对照试验报道了治疗总有效率[23,26,31,39-40,47-49,51-56,58-70,73-75,80-82],共涉及8种干预措施:超声波+常规康复、脉冲电磁场+常规康复、低能量激光+常规康复、体外冲击波+常规康复、经皮电刺激+常规康复、全身振动+常规康复、肌内效贴+常规康复和单纯常规康复治疗,总样本量2 689例。网络图中,各圆点分别表示不同的干预措施,圆点大小代表此干预措施的样本量,圆点之间连线粗细代表各干预措施的研究数量,直线表示2种干预措施间存在的直接或间接比较,不同干预措施间均存在直接或间接比较的证据,具备进行网状Meta分析的基本条件。治疗有效率的证据网络总体以常规康复治疗为中心,干预措施间无闭合环产生,无需进行不一致性检验,见图5A。 2.4.2 网状Meta分析与SUCRA排序 对8种干预措施进行两两比较,共产生28项两两比较。网状Meta分析显示,肌内效贴+常规康复(OR=1.17,95%CI[1.07,1.29])、经皮电刺激+常规康复(OR=1.18,95%CI[1.12,1.26])、体外冲击波+常规康复(OR=1.17,95%CI[1.12,1.22])、脉冲电磁场+常规康复(OR=1.28,95%CI [1.03,1.57])、超声波+常规康复治疗(OR=1.24,95%CI[1.11,1.39])治疗在提高治疗总有效率均优于单纯常规康复治疗(P < 0.05),其余干预措施间治疗总有效率相比较差异无显著性意义 (P > 0.05),见图6A。 在报告治疗总有效率的研究中,治疗总有效率的SUCRA值由高到低排序为:脉冲电磁场+常规康复(77.5%) >超声波+常规康复(76.8%) >经皮电刺激+常规康复(56.5%) >肌内效贴+常规康复(51.4%) >低能量激光+常规康复(50.0%) >体外冲击波+常规康复(47.4%) >全身振动+常规康复(38.7%) >常规康复(2.6%),见图7A。"
"
"
"
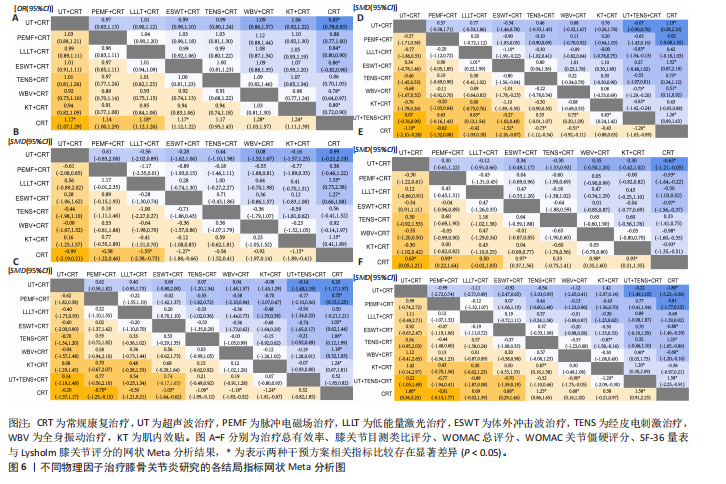
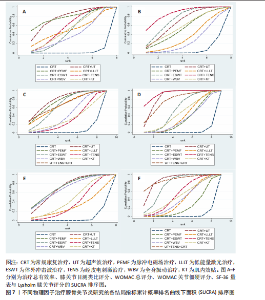
2.5 膝关节目测类比评分分析结果 2.5.1 证据网络 57项随机对照试验报道了膝关节目测类比评分[22-28,30-33,35,37-45,47-60,62-80,83-85],共涉及8种干预措施,总样本量4 044例,证据网络总体以常规康复治疗为中心,干预措施间无闭合环产生,故无需进行不一致性检验,见图5B。 2.5.2 网状Meta分析与SUCRA排序 对8种干预措施进行两两比较,共产生28项两两比较。网状Meta分析显示,经皮电刺激+常规康复(SMD=-1.55,95%CI[-2.38,-0.73])、体外冲击波+常规康复(SMD=-1.27,95%CI[-1.88,-0.66])、超声波+常规康复(SMD=-1.15,95%CI [-1.89,-0.41])治疗在改善膝关节目测类比评分方面优于常规康复治疗(P < 0.05),其余干预措施间相膝关节目测类比评分比较差异无显著性意义(P > 0.05),见图6B。 在报告膝关节目测类比评分的研究中,膝关节目测类比评分的SUCRA值概率排序为:经皮电刺激+常规康复(85.6%) >体外冲击波+常规康复(72.9%) >超声波+常规康复(65.8%) >肌内效贴+常规康复(57.1%) >脉冲电磁场+常规康复(53.0%) >低能量激光+常规康复(34.1%) >全身振动+常规康复(25.4%) >常规康复(6.1%),见图7B。 2.6 WOMAC总评分分析结果 2.6.1 证据网络 35项随机对照试验报道了WOMAC总评分[21-22,24,28-29,32-35,38,40,46,48-50,52-54,57-58,60,63,65,67,69,72,74-75,77-80,83-85],共涉及9种干预措施,总样本量2 379例,证据网络总体以常规康复治疗为中心,干预措施间产生闭合环,见图5C。为了确保分析结果的稳健性,需运用节点分裂法进行局部的一致性检验,检验结果显示P > 0.05,是说明研究间具有一致性,故在一致性模型下进行网状Meta分析。对闭环进行一致性检验,结果显示闭环IF=1.98、95%CI[0.73,3.42],提示一致性良好。 2.6.2 网状Meta分析与SUCRA排序 对9种干预措施进行两两比较,共产生36项两两比较。网状Meta分析显示,与常规康复治疗相比,肌内效贴+常规康复(SMD=-0.70,95%CI[-1.25,-0.15])、经皮电刺激+常规康复(SMD=-1.03,95%CI[-1.44,-0.62])、体外冲击波+常规康复(SMD=-1.06,95%CI[-1.99,-0.12])、低能量激光+常规康复(SMD=-1.18,95%CI[-1.83,-0.52])、脉冲电磁场+常规康复(SMD=-1.24,95%CI[-1.81,-0.67])治疗在减少WOMAC总评分方面的效果更佳(P < 0.05),其余干预措施间WOMAC总评分相比较差异无显著性意义(P > 0.05),见图6C。 在报告WOMAC总评分的研究中,WOMAC总评分的SUCRA值由高到低排序为:超声波+常规康复(77.6%) >脉冲电磁场+常规康复(72.9%) >超声波+经皮电刺激+常规康复治疗(66.0%) >低能量激光+常规康复(63.8%) >体外冲击波+常规康复(63.5%) >全身振动+常规康复(40.7%) >肌内效贴+常规康复(31.3%) >经皮电刺激+常规康复(29.7%) >常规康复(4.6%),见图7C。 2.7 WOMAC关节僵硬评分分析结果 2.7.1 证据网络 27项随机对照试验报道了WOMAC关节僵硬评分[21-22,24,28-31,33-34,37-38,41-46,49-50,52,55,57,72,76,79,82-83],共涉及9种干预措施,总样本量2 000例,证据网络总体以常规康复治疗为中心,干预措施间无闭合环产生,故无需进行不一致性检验,见图5D。 2.7.2 网状Meta分析与SUCRA排序 对9种干预措施进行两两比较,共产生36项两两比较。网状Meta分析显示,与常规康复治疗相比,超声波+经皮电刺激+常规康复(SMD=-1.19,95%CI[-2.10,-0.28])、经皮电刺激+常规康复(SMD=-1.52,95%CI[-2.18,-0.87])、体外冲击波+常规康复(SMD=-0.73,95%CI[-1.12,-0.34])、低能量激光+常规康复(SMD=-0.51,95%CI[-0.92,-0.11])、超声波+常规康复(SMD=-1.26,95%CI[-1.63,-0.89])在减少WOMAC关节僵硬评分方面的效果更佳。此外,经皮电刺激+常规康复治疗在减少WOMAC关节僵硬评分方面优于全身振动+常规康复(SMD=-1.10,95%CI[-1.99,-0.22]),超声波+常规康复治疗在减少WOMAC关节僵硬评分方面优于全身振动+常规康复(SMD=-0.83,95%CI[-1.54,-0.13])、低能量激光+常规康复(SMD=-0.75,95%CI[-1.29,-0.20])、脉冲电磁场+常规康复(SMD=-0.83,95%CI[-1.42,-0.24])治疗,差异有显著性意义(P < 0.05),其余干预措施间WOMAC关节僵硬评分比较差异无显著性意义(P > 0.05),见图6D。 在报告WOMAC关节僵硬评分的研究中,WOMAC关节僵硬评分的SUCRA值由高到低排序为:经皮电刺激+常规康复(92.8%) >超声波+常规康复(83.9%) >超声波+经皮电刺激+常规康复(75.9%) >体外冲击波治疗+常规康复治疗(53.1%) >肌内效贴+常规康复(44.0%) >低能量激光+常规康复(37.0%) >全身振动+常规康复(30.9%) >脉冲电磁场+常规康复(30.1%) >常规康复(3.0%),见图7D。 2.8 SF-36量表分析结果 2.8.1 证据网络 25项随机对照试验报道了SF-36量表[25-26,28-30,32-33,36,39,41,46,51,56,60,65-66,68,71,76-77,79,81,83-85],共涉及8种干预措施,总样本量1 727例,证据网络总体以常规康复治疗为中心,干预措施间无闭合环产生,故无需进行不一致性检验,见图5E。 2.8.2 网状Meta分析与SUCRA排序 对8种干预措施进行两两比较,共产生28项两两比较。网状Meta分析显示,肌内效贴+常规康复(SMD=0.63,95%CI[0.05,1.21])、全身振动+常规康复(SMD=0.93,95%CI[0.22,1.64])、体外冲击波+常规康复(SMD=0.97,95%CI[0.37,1.56])、脉冲电磁场+常规康复(SMD= 0.98,95%CI[0.35,1.60])、超声波+常规康复(SMD=0.93,95%CI[0.51,1.35])治疗在改善SF-36量表方面优于常规康复治疗(P < 0.05),其余干预措施间SF-36量表相比较差异无显著性意义(P > 0.05),见图6E。 在报告SF-36量表的研究中,SF-36量表的SUCRA值由高到低排序为:脉冲电磁场+常规康复(72.8%) >体外冲击波+常规康复(72.2%) >超声波治疗+常规康复(70.8%) >全身振动+常规康复(68.4%) >肌内效贴+常规康复(45.4%) >经皮电刺激+常规康复(35.9%) >低能量激光+常规康复(29.8%) >常规康复(4.7%),见图7E。 2.9 Lysholm膝关节评分分析结果 2.9.1 证据网络 38项随机对照试验报道了Lysholm膝关节评分[21,23-24,26,30,33-34,38-46,48-52,55,57-60,62-63,66,69-71,73,76,78-79,81,84],共涉及9种干预措施,总样本量2 783例,证据网络总体以常规康复治疗为中心,干预措施间无闭合环产生,故无需进行不一致性检验,见图5F。2.9.2 网状Meta分析与SUCRA排序 对9种干预措施进行两两比较,共产生36项两两比较。网状Meta分析显示,超声波+经皮电刺激+常规康复(SMD=1.80,95%CI[0.36,3.23])、经皮电刺激+常规康复(SMD=0.88,95%CI[0.29,1.46])、体外冲击波+常规康复(SMD=1.25,95%CI[0.86,1.65])、低能量激光+常规康复(SMD=0.68,95%CI[0.16,1.20])、超声波+常规康复(SMD=1.58,95%CI[0.91,2.25])治疗在改善Lysholm膝关节评分方面优于常规康复治疗(P < 0.05);此外,体外冲击波+常规康复治疗在改善Lysholm膝关节评分方面优于脉冲电磁场+常规康复治疗(SMD=0.87,95%CI[0.16,1.58]),超声波+常规康复治疗在改善Lysholm膝关节评分方面优于脉冲电磁场+常规康复(SMD=1.20,95%CI[0.30,2.09])、低能量激光+常规康复治疗(SMD=0.90,95%CI[0.05,1.75]),差异有显著性意义(P < 0.05),其余干预措施间"
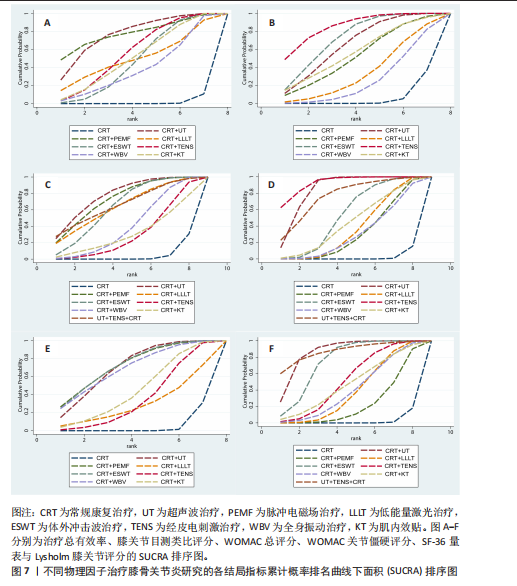

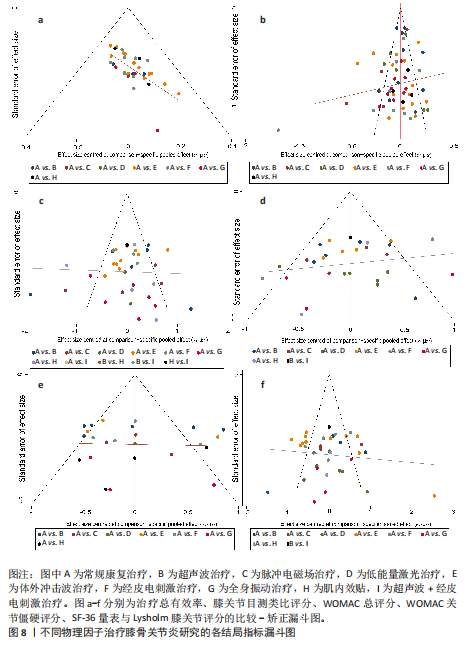
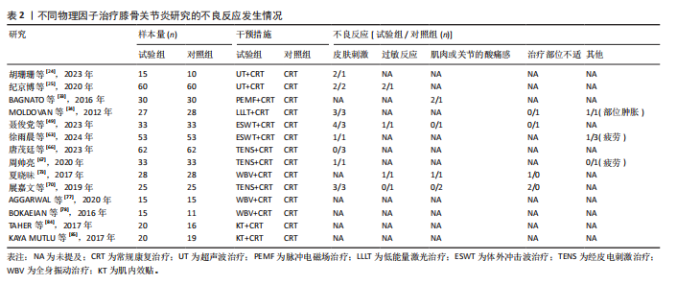
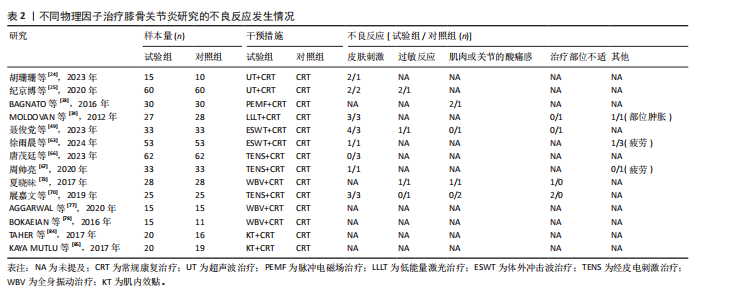
Lysholm膝关节评分比较差异无显著性意义(P > 0.05),见图6F。 在报告Lysholm膝关节评分的研究中,Lysholm膝关节评分的SUCRA值由高到低排序为:超声波+常规康复(86.6%) >超声波+经皮电刺激+常规康复(86.5%) >体外冲击波+常规康复(74.1%) >经皮电刺激+常规康复(51.5%) >肌内效贴+常规康复(48.0%) >全身振动+常规康复(39.7%) >低能量激光+常规康复(38.9%) >脉冲电磁场+常规康复(22.3%) >常规康复(4.5%),见图7F。 2.10 不良反应发生率 46项随机对照试验报道了不良反应发生率[21,23-25,27-30,32,34-36,39,41-43,45-47,49-50,53,55-57,59-61,63-67,70-73,75,77-82,84-85],其中,32篇报告治疗期间均未发生与干预措施等相关的不良反应,14篇对不良反应发生情况进行了描述,共涉及8种干预措施,共有65例患者出现不良反应,主要包括皮肤刺激、过敏反应、肌肉或关节的酸痛感和治疗部位稍肿胀等表现,由于每个研究间不良反应不同,因此只作描述性统计,见表2。 2.11 文献发表偏倚 此次研究对各结局指标进行发表偏倚分析,绘制“比较-矫正”漏斗图,进行偏倚分析,漏斗图中的圆点表示不同干预措施之间的一对一比较,点的颜色代表不同的干预措施或对照组类别,每种颜色点的数量代表报告比较的研究数量。如果不存在小样本量或发表偏差的影响,漏斗图中的点对称且均匀分布在垂直线的两侧(X=0)。检验结果显示,治疗总有效率、WOMAC总评分、WOMAC关节僵硬评分、SF-36量表和Lysholm膝关节评分结局指标的纳入研究总体对称分布于倒漏斗图的中上部,围绕中线左右两侧,提示发表偏倚的可能性较小;膝关节目测类比评分结局指标的漏斗图左右对称性欠佳,并且部分圆点散落在95%CI区域外,提示纳入文献可能存在一定的发表偏倚或是小样本效应,见图8。 进一步进行对所有结局指标进行敏感性分析Egger检验,结果显示治疗总有效率的P=0.532、膝关节目测类比评分的 P=0.780、WOMAC总评分的P=0.322、WOMAC关节僵硬评分的P=0.725、SF-36量表的P=0.617、Lysholm膝关节评分的P=0.403,提示所纳入的研究不存在小样本研究效应且具有一定的稳健性。"
"
| [1] BANNURU RR, OSANI MC, VAYSBROT EE, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578-1589. [2] 中华中医药学会.膝骨关节炎中西医结合诊疗指南(2023年版)[J].中医正骨,2023,35(6):1-10. [3] DI J, BAI J, ZHANG J, et al. Regional disparities, age-related changes and sex-related differences in knee osteoarthritis. BMC Musculoskelet Disord. 2024;25(1):66. [4] GIORGINO R, ALBANO D, FUSCO S, et al. Knee Osteoarthritis: Epidemiology, Pathogenesis, and Mesenchymal Stem Cells: What Else Is New? An Update. Int J Mol Sci. 2023;24(7):6405. [5] TONG L, YU H, HUANG X, et al. Current understanding of osteoarthritis pathogenesis and relevant new approaches. Bone Res. 2022; 10(1):60. [6] ZENG C, ZHANG W, DOHERTY M, et al. Initial analgesic prescriptions for osteoarthritis in the United Kingdom, 2000-2016. Rheumatology (Oxford). 2021;60(1):147-159. [7] WENG Q, GOH SL, WU J, et al. Comparative efficacy of exercise therapy and oral non-steroidal anti-inflammatory drugs and paracetamol for knee or hip osteoarthritis: a network meta-analysis of randomised controlled trials. Br J Sports Med. 2023;57(15):990-996. [8] JANG S, LEE K, JU JH. Recent Updates of Diagnosis, Pathophysiology, and Treatment on Osteoarthritis of the Knee. Int J Mol Sci. 2021;22(5):2619. [9] DANTAS LO, SALVINI TF, MCALINDON TE. Knee osteoarthritis: key treatments and implications for physical therapy. Braz J Phys Ther. 2021;25(2): 135-146. [10] PERS YM, NGUYEN C, BORIE C, et al. Recommendations from the French Societies of Rheumatology and Physical Medicine and Rehabilitation on the non-pharmacological management of knee osteoarthritis. Ann Phys Rehabil Med. 2024;67(7):101883. [11] YANG X, HE H, YE W, et al. Effects of Pulsed Electromagnetic Field Therapy on Pain, Stiffness, Physical Function, and Quality of Life in Patients With Osteoarthritis: A Systematic Review and Meta-Analysis of Randomized Placebo-Controlled Trials. Phys Ther. 2020;100(7):1118-1131. [12] AVENDAÑO-COY J, COMINO-SUÁREZ N, GRANDE-MUÑOZ J, et al. Extracorporeal shockwave therapy improves pain and function in subjects with knee osteoarthritis: A systematic review and meta-analysis of randomized clinical trials. Int J Surg. 2020;82:64-75. [13] WU Y, ZHU F, CHEN W, et al. Effects of transcutaneous electrical nerve stimulation (TENS) in people with knee osteoarthritis: A systematic review and meta-analysis. Clin Rehabil. 2022;36(4):472-485. [14] PAGE MJ, MOHER D, BOSSUYT PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. [15] 骨科学分会关节外科学组.骨关节炎诊治指南(2018年版)[J].中华骨科杂志,2018,38(12):705-715. [16] KOLASINSKI SL, NEOGI T, HOCHBERG MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020;72(2):220-233. [17] 中华医学会物理医学与康复学分会,四川大学华西医院.中国膝骨关节炎康复治疗指南(2023版)[J].中国循证医学杂志,2024,24(1):1-14. [18] HIGGINS JP, ALTMAN DG, GØTZSCHE PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. [19] EGGER M, DAVEY SMITH G, SCHNEIDER M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629-634. [20] BEGG CB, MAZUMDAR M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088-1101. [21] 杨海,蔡菊红,周驰,等.超声波结合经皮神经电刺激对膝骨关节炎患者膝关节疼痛和功能的影响[J].中国康复医学杂志,2024,39(8):1174-1179. [22] 蓝惠平,刘芳.超声波治疗仪联合抗阻训练在膝骨关节炎患者中的应用效果[J].医疗装备, 2025,38(4):85-88. [23] 宋莎,刘勇,张彬霞,等.低强度脉冲超声波联合股四头肌肌力强化训练治疗膝骨关节炎患者的临床疗效观察[J].现代生物医学进展, 2020,20(14):2668-2671. [24] 胡珊珊,刘晓,罗汉才,等.低强度脉冲超声调控治疗疼痛性膝骨关节炎的临床研究[J].实用医学杂志,2023,39(21):2783-2788. [25] 纪京博,赵忠全,李学福,等.低强度脉冲超声对膝骨关节炎患者血清TIMP-2和软骨MMP-13表达的影响[J].川北医学院学报,2020,35(6): 986-989. [26] 成逸,徐艳,王飞.低强度脉冲超声缓解膝骨关节炎疼痛与修复关节软骨损伤研究[J].中国现代医生,2019,57(25):32-35. [27] 王广,王传敏,马利中.低强度脉冲超声联合本体感觉训练治疗膝骨关节炎疗效观察[J].医学理论与实践,2022,35(1):161-163. [28] 王枰稀,曾凡伟,张东,等.低强度脉冲聚焦超声对早中期膝关节骨关节炎患者关节功能影响的研究[J].川北医学院学报,2021,36(4):433-436. [29] 殷娜,汤锋武,符锋,等.低强度脉冲聚焦超声联合等速肌力训练对膝骨关节炎患者膝关节本体感觉、生活质量和炎性因子水平的影响[J].现代生物医学进展,2021,21(22):4275-4278,4297. [30] 谭显春,李智,李欣,等.低强度脉冲聚焦超声治疗对膝骨关节炎患者疼痛和关节功能的改善作用及其安全性[J].临床和实验医学杂志, 2020,19(5):541-544. [31] 王雪.扶他林乳胶剂局部外用作为超声介质联合超声波治疗膝骨性关节炎的疗效[J].中国处方药,2020,18(10):94-95. [32] JIA L, WANG Y, CHEN J, et al. Efficacy of focused low-intensity pulsed ultrasound therapy for the management of knee osteoarthritis: a randomized, double blind, placebo-controlled trial. Sci Rep. 2016;6:35453. [33] BAGNATO GL, MICELI G, MARINO N, et al. Pulsed electromagnetic fields in knee osteoarthritis: a double blind, placebo-controlled, randomized clinical trial. Rheumatology (Oxford). 2016;55(4): 755-762. [34] MOLDOVAN I, DIŢĂ R, POP L. The effects of focused pulsed electromagnetic field therapy in patients with knee osteoarthritis. A randomised, placebo-controlled study. Palestrica of the Third Millennium Civilization and Sport. 2012;13:91-95. [35] DÜNDAR Ü, AŞIK G, ULAŞLI AM, et al. Assessment of pulsed electromagnetic field therapy with Serum YKL-40 and ultrasonography in patients with knee osteoarthritis. Int J Rheum Dis. 2016; 19(3):287-293. [36] KANAT E, ALP A, YURTKURAN M. Magnetotherapy in hand osteoarthritis: a pilot trial. Complement Ther Med. 2013;21(6):603-608. [37] THAMSBORG G, FLORESCU A, OTURAI P, et al. Treatment of knee osteoarthritis with pulsed electromagnetic fields: a randomized, double-blind, placebo-controlled study. Osteoarthritis Cartilage. 2005;13(7):575-581. [38] WUSCHECH H, VON HEHN U, MIKUS E, et al. Effects of PEMF on patients with osteoarthritis: Results of a prospective, placebo-controlled, double-blind study. Bioelectromagnetics. 2015; 36(8):576-585. [39] 龚薇,龚瑜,陈淑君.脉冲电磁场联合康复护理对膝骨关节炎患者的疗效[J].医疗装备, 2023,36(15):114-116. [40] 娄晓乐,陶雅亭,林霖,等.神经肌肉运动训练联合半导体激光对膝骨关节炎患者的影响[J].康复学报,2025,35(4):439-444. [41] MAHLER EAM, MINTEN MJ, LESEMAN-HOOGENBOOM MM, et al. Effectiveness of low-dose radiation therapy on symptoms in patients with knee osteoarthritis: a randomised, double-blinded, sham-controlled trial. Ann Rheum Dis. 2019;78(1):83-90. [42] ALGHADIR A, OMAR MT, AL-ASKAR AB, et al. Effect of low-level laser therapy in patients with chronic knee osteoarthritis: a single-blinded randomized clinical study. Lasers Med Sci. 2014;29(2):749-755. [43] DE PAULA GOMES CAF, LEAL-JUNIOR ECP, DIBAI-FILHO AV, et al. Incorporation of photobiomodulation therapy into a therapeutic exercise program for knee osteoarthritis: A placebo-controlled, randomized, clinical trial. Lasers Surg Med. 2018;50(8):819-828. [44] KHESHIE AR, ALAYAT MS, ALI MM. High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: a randomized controlled trial. Lasers Med Sci. 2014;29(4):1371-1376. [45] KOUTENAEI FR, MOSALLANEZHAD Z, NAGHIKHANI M, et al. The Effect of Low Level Laser Therapy on Pain and Range of Motion of Patients With Knee Osteoarthritis. Phys Treatments, 2017;7(1):13-18. [46] BRAGHIN A, MOEZY A, NEJATI P, et al. Efficacy of high-intensity laser therapy in comparison with conventional physiotherapy and exercise therapy on pain and function of patients with knee osteoarthritis: a randomized controlled trial with 12-week follow up. Lasers Med Sci. 2019; 34(3):505-516. [47] 赵建强,陈颖,张帅.不同频率冲击波治疗膝骨性关节炎效果观察[J].中国城乡企业卫生,2024, 39(1):137-138. [48] 梁恩龙,胡运翔,唐玉萍,等.体外冲击波触发点疗法治疗早中期膝骨关节炎的临床研究[J].中国医药科学,2024,14(24):165-169. [49] 聂俊党,宋涛.体外冲击波联合常规康复治疗膝骨关节炎疼痛的临床效果[J].长治医学院学报,2023,37(6):435-438. [50] 肖迪珅,赵恒,刘凌.体外冲击波联合扶他林乳胶剂外用治疗对早中期膝骨关节炎患者的临床研究[J].中华保健医学杂志,2024,26(2):254-256. [51] 王晖,杨佳媛,李文.体外冲击波联合神经肌肉训练治疗老年膝骨关节炎及对膝关节滑液IL-1β、IL-17、PGE2水平的影响[J].宁夏医科大学学报,2024,46(8):791-796. [52] 何岚娟.体外冲击波联合双氯芬酸二乙胺乳胶剂治疗膝骨关节炎患者的效果[J].中国民康医学,2024,36(22):49-51. [53] 马文虎,祁晓.体外冲击波联合中药外敷治疗膝骨关节炎的临床效果及对炎症因子的影响[J].中国当代医药,2025,32(9):48-58. [54] 蒋黎明,于小明,丁余武,等.体外冲击波疗法联合站桩训练治疗膝骨关节炎的临床疗效[J].广西医学,2022,44(16):1847-1850. [55] 王建锋,张海明,刘杰.体外冲击波穴位疗法对膝骨性关节炎患者关节功能及骨代谢分子分泌的影响[J].中国卫生检验杂志,2022,32(15):1855-1859. [56] 郑亚利,杨青山.体外冲击波治疗对膝骨关节炎患者临床相关指标的影响[J].中国临床医生杂志,2021,49(6):717-719. [57] 顾彬,段建军,谢红霞,等.体外冲击波治疗膝骨性关节炎的近期疗效分析[J].中外医疗, 2024,43(20):79-83. [58] 吴杨玲,钟婷,唐芳.体外冲击波治疗早中期膝骨关节炎的临床效果观察[J].实用医院临床杂志,2022,19(2):62-64. [59] 董博,雷涛.体外穴位冲击波治疗早期膝骨关节炎的疗效研究[J].现代中医药,2022,42(1): 108-110. [60] 周琪.推拿手法配合冲击波穴位疗法治疗膝骨性关节炎患者的疗效及其对运动功能的影响[J].慢性病学杂志,2024,25(5):745-751. [61] 杨毅峰,黄健,邸申,等.膝骨关节炎患者应用体外冲击波联合站桩训练的效果及炎症水平分析[J].中国医学创新,2023,20(10):116-119. [62] 马玉海,张霆,赵文修,等.穴位及经筋结点体外冲击波疗法治疗膝骨关节炎的临床研究[J].浙江中西医结合杂志,2024,34(12):1147-1150. [63] 徐雨晨,沈松筠.常规康复治疗配合经皮穴位电刺激在膝骨关节炎中的应用效果[J].中外医学研究,2024,22(34):169-172. [64] 殷建波,王敏,任丽,等.经皮电刺激神经疗法配合宣氏强刺激推拿法治疗膝骨性关节炎[J].中医临床研究,2018,10(3):64-67. [65] 朱立,赵学田.经皮神经电刺激联合等速离心训练对膝骨关节炎患者疼痛程度及肌肉力量的影响[J].临床医药实践,2025,34(2):109-112. [66] 唐茂廷,王振.经皮神经电刺激治疗对膝骨关节炎患者膝关节功能、VAS评分及效果的影响[J].名医,2023(6):51-53. [67] 周帅亮,岑珏,郭艳明,等.经皮穴位电刺激结合运动疗法治疗膝骨关节炎的临床研究[J].中国中医骨伤科杂志,2020,28(2):15-18. [68] 连占生,徐振文,李青天.经皮穴位电刺激治疗膝骨关节炎的临床效果研究[J].名医, 2021(10):141-142. [69] 尹煜辉,陈明,李玲慧,等.松筋调膝手法联合经皮神经电刺激治疗膝骨关节炎的临床研究[J].中国中医骨伤科杂志,2025,33(4):27-32. [70] 展嘉文,王尚全,朱立国,等.经皮穴位电刺激治疗膝骨关节炎的临床研究[J].中国中医骨伤科杂志,2019,27(8):28-31. [71] 杨婕.经皮穴位电刺激与温针灸治疗膝骨性关节炎的比较研究[J].内蒙古中医药,2016,35(2): 134-135. [72] 刘珂,陈光,黄月乔,等.全身振动训练对膝骨关节炎有效性的随机对照研究[J].生物医学工程与临床,2015,19(6):609-612. [73] 夏晓昧,刘臻,陆飞,等.全身振动训练联合有氧训练治疗膝关节骨性关节炎的疗效观察[J].影像研究与医学应用,2017,1(11):186-188. [74] 张翼,秦佳维,何泽祥,等.全身振动训练联合运动疗法在膝关节骨性关节炎中的应用效果[J].中国当代医药,2021,28(8):77-80. [75] 王美元,冯瑞伟,雷鸣,等.针刺配合全身振动训练治疗膝骨关节炎的临床观察[J].中国中医急症,2024,33(12):2152-2155. [76] WANG P, YANG L, LI H, et al. Effects of whole-body vibration training with quadriceps strengthening exercise on functioning and gait parameters in patients with medial compartment knee osteoarthritis: a randomised controlled preliminary study. Physiotherapy. 2016;102(1):86-92. [77] AGGARWAL A, PARANJAPE PR, PALEKAR TJ, et al. Effect of whole body vibration on lower body strength and balance in osteoarthritis knee. Int J Physiother. 2020;7:86-92. [78] BOKAEIAN HR, BAKHTIARY AH, MIRMOHAMMADKHANI M, et al. The effect of adding whole body vibration training to strengthening training in the treatment of knee osteoarthritis: A randomized clinical trial. J Bodyw Mov Ther. 2016;20(2):334-340. [79] AVELAR NC, SIMÃO AP, TOSSIGE-GOMES R, et al. The effect of adding whole-body vibration to squat training on the functional performance and self-report of disease status in elderly patients with knee osteoarthritis: a randomized, controlled clinical study. J Altern Complement Med. 2011; 17(12):1149-1155. [80] 赵青,代洪燕,张春雷,等.肌内效贴扎辅助治疗对膝骨关节炎患者疼痛水平的影响[J].武警后勤学院学报(医学版),2021,30(11):20-22. [81] 武中庆,许侃娜,沈云龙,等.肌内效贴治疗早期膝骨关节炎的效果[J].中国医药导报,2023, 20(24):89-92. [82] 纪任欣,余波,何霏,等.中西医结合改良肌内效贴对膝骨性关节炎影响的临床研究[J].上海中医药杂志,2018,52(2):71-74,108. [83] PARK SH, PARK YH, LEE JH. Effects of magnetic field therapy after taping application on pain and function of patients with knee osteoarthritis. J Phys Ther Sci. 2017;29(9):1548-1551. [84] TAHERI P, VAHDATPOUR B, ASL MM, et al. Effects of Taping on Pain and Functional Outcome of Patients with Knee Osteoarthritis: A Pilot Randomized Single-blind Clinical Trial. Adv Biomed Res. 2017;6:139. [85] KAYA MUTLU E, MUSTAFAOGLU R, BIRINCI T, et al. Does Kinesio Taping of the Knee Improve Pain and Functionality in Patients with Knee Osteoarthritis?: A Randomized Controlled Clinical Trial. Am J Phys Med Rehabil. 2017;96(1):25-33. [86] TUNCER T, CAY FH, ALTAN L, et al. 2017 update of the Turkish League Against Rheumatism (TLAR) evidence-based recommendations for the management of knee osteoarthritis. Rheumatol Int. 2018;38(8):1315-1331. [87] SABHA M, HOCHBERG MC. Non-surgical management of hip and knee osteoarthritis; comparison of ACR/AF and OARSI 2019 and VA/DoD 2020 guidelines. Osteoarthr Cartil Open. 2021;4(1):100232. [88] MELZACK R, WALL PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971-979. [89] VANCE CGT, DAILEY DL, CHIMENTI RL, et al. Using TENS for Pain Control: Update on the State of the Evidence. Medicina (Kaunas). 2022;58(10):1332. [90] REICHENBACH S, JÜNI P, HINCAPIÉ CA, et al. Effect of transcutaneous electrical nerve stimulation (TENS) on knee pain and physical function in patients with symptomatic knee osteoarthritis: the ETRELKA randomized clinical trial. Osteoarthritis Cartilage. 2022;30(3):426-435. [91] TEIXEIRA PEP, ALAWDAH L, ALHASSAN HAA, et al. The Analgesic Effect of Transcranial Direct Current Stimulation (tDCS) combined with Physical Therapy on Common Musculoskeletal Conditions: A Systematic Review and Meta-Analysis. Princ Pract Clin Res. 2020;6(1):23-26. [92] RAHIMI F, NEJATI V, NASSADJ G, et al. The effect of transcranial direct stimulation as an add-on treatment to conventional physical therapy on pain intensity and functional ability in individuals with knee osteoarthritis: A randomized controlled trial. Neurophysiol Clin. 2021;51(6):507-516. [93] TAVARES DRB, OKAZAKI JEF, SANTANA MVA, et al. Motor cortex transcranial direct current stimulation effects on knee osteoarthritis pain in elderly subjects with dysfunctional descending pain inhibitory system: A randomized controlled trial. Brain Stimul. 2021;14(3):477-487. [94] SCHAMBRA HM, BIKSON M, WAGER TD, et al. It’s all in your head: reinforcing the placebo response with tDCS. Brain Stimul. 2014;7(4):623-634. [95] CAKIR S, HEPGULER S, OZTURK C, et al. Efficacy of therapeutic ultrasound for the management of knee osteoarthritis: a randomized, controlled, and double-blind study. Am J Phys Med Rehabil. 2014;93(5):405-412. [96] ÖZGÖNENEL L, OKUR SÇ, DOGAN YP, et al. Effectiveness of Therapeutic Ultrasound on Clinical Parameters and Ultrasonographic Cartilage Thickness in Knee Osteoarthritis: A Double-Blind Trial. J Med Ultrasound. 2018;26(4):194-199. [97] JIA L, CHEN J, WANG Y, et al. Focused Low-intensity Pulsed Ultrasound Affects Extracellular Matrix Degradation via Decreasing Chondrocyte Apoptosis and Inflammatory Mediators in a Surgically Induced Osteoarthritic Rabbit Model. Ultrasound Med Biol. 2016;42(1):208-219. [98] YEĞIN T, ALTAN L, KASAPOĞLU AKSOY M. The Effect of Therapeutic Ultrasound on Pain and Physical Function in Patients with Knee Osteoarthritis. Ultrasound Med Biol. 2017;43(1):187-194. [99] RODRÍGUEZ-GRANDE EI, OSMA-RUEDA JL, SERRANO-VILLAR Y, et al. Effects of pulsed therapeutic ultrasound on the treatment of people with knee osteoarthritis. J Phys Ther Sci. 2017;29(9):1637-1643. [100] YILDIZ SK, ÖZKAN FÜ, AKTAŞ I, et al. The effectiveness of ultrasound treatment for the management of knee osteoarthritis: a randomized, placebo-controlled, double-blind study. Turk J Med Sci. 2015;45(6):1187-1191. |
| [1] | Liu Jinlong, Abuduwupuer·Haibier, Bai Zhen, Su Danyang, Miao Xin, Li Fei, Yang Xiaopeng. Efficacy of different nonsurgical treatments for adolescent idiopathic scoliosis: a systematic review and network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2370-2379. |
| [2] | Yang Qiongqiong, Liu Wei. Comparison of performance and clinical effects of zirconia and titanium implants [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 2063-2071. |
| [3] | Wang Zhenze, Liu Fende, Zhang Rui, Li Wujun. Mesenchymal stem cells in treatment of arteriosclerosis obliterans of lower extremities: systematic review and meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(7): 1869-1876. |
| [4] | Zheng Yin, Wu Zhenhua, Zhang Cheng, Ruan Kexin, Gang Xiaolin, Ji Hong. Safety and efficacy of immunoadsorption therapy for rheumatoid arthritis: a network meta-analysis and systematic review [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(5): 1260-1268. |
| [5] | Leng Xiaoxuan, Zhao Yuxin, Liu Xihua. Effects of different neuromodulatory stimulation modalities on non-motor symptoms in Parkinson’s patients: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(5): 1282-1293. |
| [6] | Yang Yuanyuan, Zhou Shanshan, Cheng Xiaofei, Feng Luye, Tang Jiqin. Network meta-analysis of non-invasive brain stimulation in the treatment of lower limb motor dysfunction after stroke [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(4): 1008-1018. |
| [7] | Wang Yanfei, Jin Lianhai, Li Qingya, Fu Yuanfei, Tan Huangsheng, Deng Pengwei, Gao Kun. Synovial fluid exosome-mediated crosstalk between synoviocytes and chondrocytes in development and progression of knee osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(34): 9032-9040. |
| [8] | Wang Yalei, Wang Xuezhi, Zhou Tao, Shen Xinxin, Fang Ding, Chen Hongliang. Effect of sacroiliac joint ankylosis on outcomes of L5/S1 transforminal lumbar interbody fusion and lumbar sagittal parameters [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(3): 634-641. |
| [9] | Liao Guangtao, Feng Ziyu, Fu Xiaoyong, Zhao Qinglan, Chen Chao, Hong Jinsong. Subtalar arthroereisis for treatment of pediatric flexible flatfoot: relationship between radiographic indicators and clinical efficacy [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(3): 661-670. |
| [10] | Zhao Ke, Zhang Ping, Xi Yongping, Zeng Fanzhi, Zhang Liru. Optimal exercise prescription for chronic low back pain in adults: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(29): 7688-7695. |
| [11] | Yong Qiao, Sun Xin, Wang Guoyou, Zhang Lei, Shen Huarui, Liu Huan, Guan Taiyuan. Shaoyang Shenggu Fang inhibits oxidative stress and delays cartilage aging in rats with knee osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(28): 7251-7259. |
| [12] | Bai Xue, Tian Yukui, Guo Lei, Shi Mengni, Cui Xiaofeng, Wang Cheng, Li Jingxian, Zhu Qingguang, Liu Junchang. Construction of an early knee osteoarthritis rat model: CatWalk-based gait analysis and evaluation [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(28): 7280-7286. |
| [13] | Li Sihui, Wang Qin, Cui Shenhong, Cheng Xiaofei, Feng Ziyun, Wang Dehua, Liang Chunting, Leng Jun. A network meta-analysis of effects of non-invasive neuromodulation techniques on language function in patients with aphasia after stroke [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(28): 7485-7493. |
| [14] | Fan Mengmeng, Ding Jiali, Wan Yujie, Huang Hailiang. A systematic review and network meta-analysis of neuromodulation techniques for promoting upper limb motor function after stroke [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(28): 7494-7504. |
| [15] | Zhang Kaijing, Li Chunnian, Li Yizhuo, Xu Shifang, Liu Xinyue. A network meta-analysis of therapeutic effects of different bone repair materials on apical bone defects [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(26): 6946-6951. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||