Chinese Journal of Tissue Engineering Research ›› 2020, Vol. 24 ›› Issue (30): 4905-4913.doi: 10.3969/j.issn.2095-4344.2844
Previous Articles Next Articles
A meta-analysis of high tibial osteotomy and monocondylar replacement for treating medial interventricular osteoarthritis of the knee
Bai Hao1, Sun Haibiao2, Han Xiaoqiang2, Xue Jiangang1
- 1Shanxi Medical University, Taiyuan 030001, Shanxi Province, China; 2First Hospital, Shanxi Medical University, Taiyuan 030001, Shanxi Province, China
-
Received:2019-12-23Revised:2019-12-27Accepted:2020-03-04Online:2020-10-28Published:2020-09-22 -
Contact:Sun Haibiao, MD, Chief physician, First Hospital, Shanxi Medical University, Taiyuan 030001, Shanxi Province, China -
About author:Bai Hao, Master candidate, Physician, Shanxi Medical University, Taiyuan 030001, Shanxi Province, China -
Supported by:the Support Plan for Distinguished Professors of Young Scholars in Shanxi Province, No. [Jincai (2016)128-2]
CLC Number:
Cite this article
Bai Hao, Sun Haibiao, Han Xiaoqiang, Xue Jiangang. A meta-analysis of high tibial osteotomy and monocondylar replacement for treating medial interventricular osteoarthritis of the knee[J]. Chinese Journal of Tissue Engineering Research, 2020, 24(30): 4905-4913.
share this article
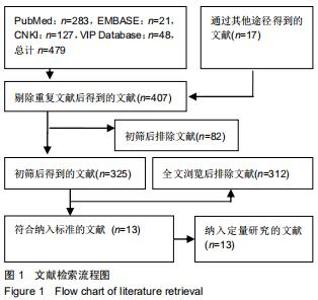
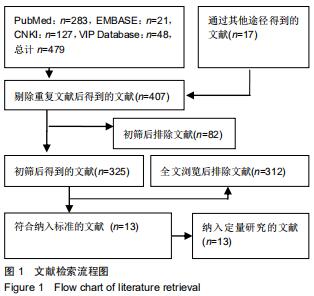
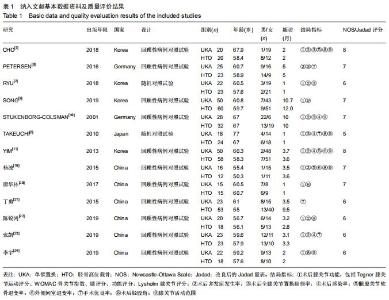
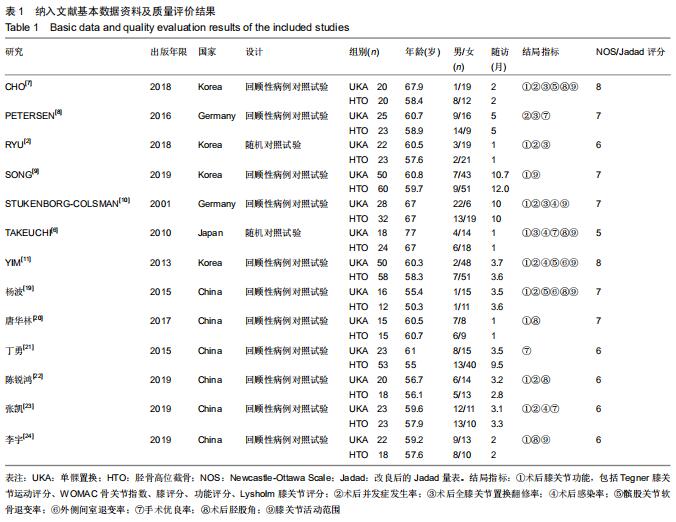
2.1 文献检索结果 共检索到479篇文献,其中PubMed 283篇,EMBASE 21篇,CNKI 127篇,VIP Database 48篇,其他来源17篇,通过纳入和排除标准,最后符合标准的共13篇,包括2篇随机对照试验[2,6],以及11篇回顾性病例对照研究[7-11,19-24];其中来自韩国4篇,德国2篇,日本1篇,中国6篇,见图1及表1,总计711例膝关节内侧间室骨关节炎患者,379例行胫骨高位截骨术,332例行单髁置换术。根据NOS量表进行文献质量评价,2篇8分,5篇7分,4篇6分;根据Jadad量表(改良后),1篇6分,1篇5分。 "
2.1 文献检索结果 共检索到479篇文献,其中PubMed 283篇,EMBASE 21篇,CNKI 127篇,VIP Database 48篇,其他来源17篇,通过纳入和排除标准,最后符合标准的共13篇,包括2篇随机对照试验[2,6],以及11篇回顾性病例对照研究[7-11,19-24];其中来自韩国4篇,德国2篇,日本1篇,中国6篇,见图1及表1,总计711例膝关节内侧间室骨关节炎患者,379例行胫骨高位截骨术,332例行单髁置换术。根据NOS量表进行文献质量评价,2篇8分,5篇7分,4篇6分;根据Jadad量表(改良后),1篇6分,1篇5分。 "
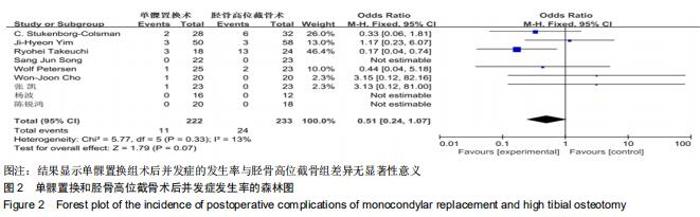
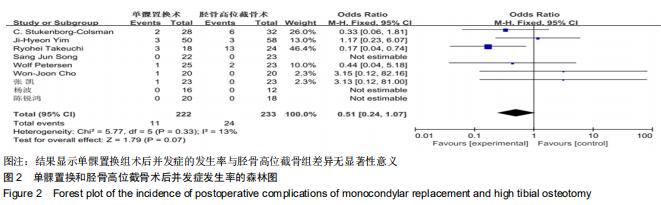
2.2 单髁置换和胫骨高位截骨术后并发症发生率的Meta分析结果 有9篇文献比较了末次随访总并发症发生率[6-11,19,22-23],共纳入455例患者进行Meta分析,单髁置换组222例,胫骨高位截骨组233例。Q检验,I2=13%,P=0.33,显示纳入的9篇文献异质性小,采用固定效应模型计算单髁置换组vs.胫骨高位截骨组的合并OR值为0.51,95%CI(0.24-1.07),P=0.07,结果显示单髁置换组术后并发症的发生率与胫骨高位截骨组差异无显著性意义,见图2。 "
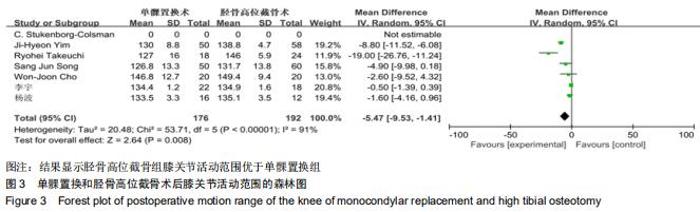
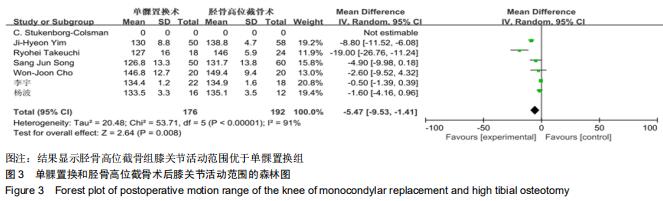
2.3 单髁置换和胫骨高位截骨术后膝关节活动范围的Meta分析结果 有7篇文献比较了膝关节活动范围[6-7,9-11,19,24],共纳入368例患者进行Meta分析,单髁置换组176例,胫骨高位截骨组192例。Q检验,I2=91%,P < 0.000 01,显示7篇纳入文献异质较大,采用随机效应模型计算单髁置换组vs.胫骨高位截骨组的合并MD值为-5.47,95%CI(-9.53,-1.41),合并结果显示胫骨高位截骨组膝关节活动范围优于单髁置换组,且差异有显著性意义(P=0.008),见图3。 "
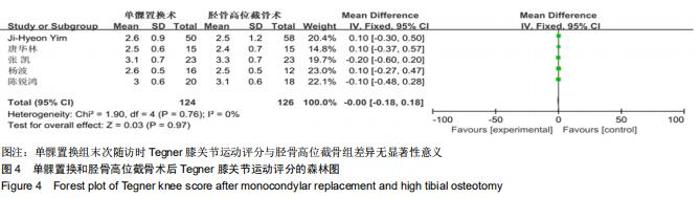
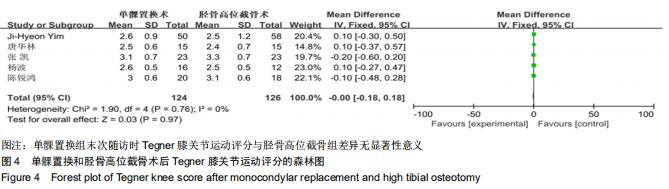
2.4.1 Tegner膝关节运动评分 有5篇文献比较了末次随访时Tegner膝关节运动评分[11,19-20,22-23],共纳入250例患者进行Meta分析,单髁置换组124例,胫骨高位截骨组126例。Q检验,I2=0%,P=0.76,显示5篇纳入文献不存在异质性,采用固定效应模型计算单髁置换组vs.胫骨高位截骨组的合并MD值为-0.00,95%CI(-0.18,0.18),P=0.97,结果显示单髁置换组末次随访时Tegner膝关节运动评分与胫骨高位截骨组差异无显著性意义,见图4。 "
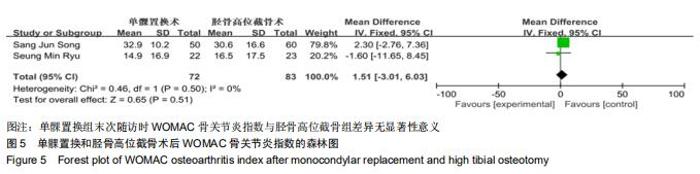
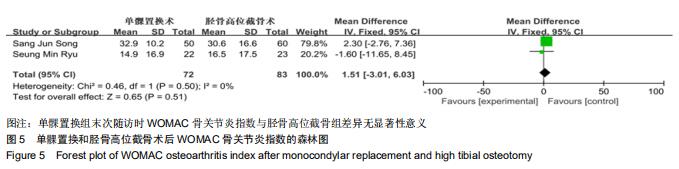
2.4.2 WOMAC骨关节炎指数 有2篇文献比较了末次随访时WOMAC骨关节炎指数[2,9],共纳入155例患者进行Meta分析,单髁置换组72例,胫骨高位截骨组83例。Q检验,I2=0%,P=0.50,显示2篇纳入文献不存在异质性,采用固定效应模型计算单髁置换组vs.胫骨高位截骨组的合并MD值为1.51,95%CI(-3.01,6.03),P=0.51,结果显示单髁置换组末次随访时WOMAC骨关节炎指数与胫骨高位截骨组差异无显著性意义,见图5。 "
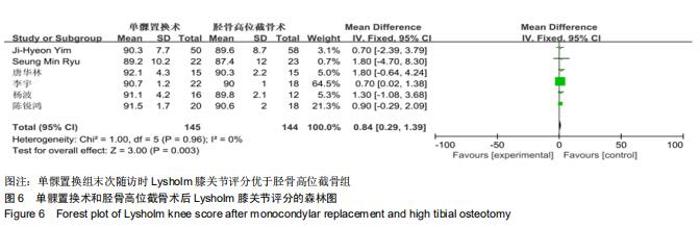
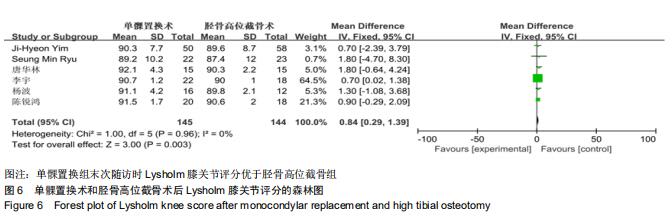
2.4.3 Lysholm膝关节评分 有6篇文献比较了末次随访时Lysholm膝关节评分[2,11,19-20,22,24],共纳入289例患者进行Meta分析,单髁置换组145例,胫骨高位截骨组144例。Q检验,I2=0%,P=0.96,显示6篇纳入文献不存在异质性,采用固定效应模型计算单髁置换组vs.胫骨高位截骨组的合并MD值为0.84,95%CI(0.29,1.39),结果显示单髁置换组末次随访时Lysholm膝关节评分优于胫骨高位截骨组,且差异有显著性意义(P=0.003),见图6。 "
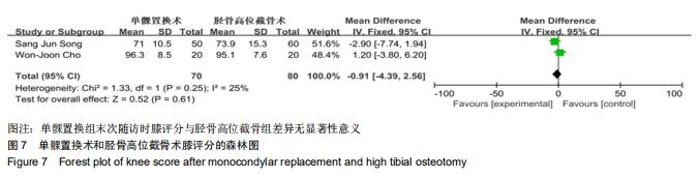
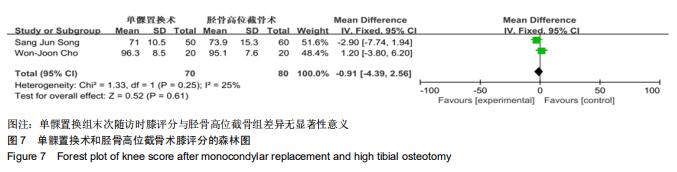
2.4.4 膝评分 有2篇文献比较了末次随访时膝评分[7,9],共纳入150例患者进行Meta分析,单髁置换组70例,胫骨高位截骨组80例。Q检验,I2=25%,P=0.25,显示2篇纳入文献不存在异质性,采用固定效应模型计算单髁置换组vs.胫骨高位截骨组的合并MD值为-0.91,95%CI(-4.39,2.56),P=0.61,结果显示单髁置换组末次随访时膝评分与胫骨高位截骨组差异无显著性意义,见图7。 "
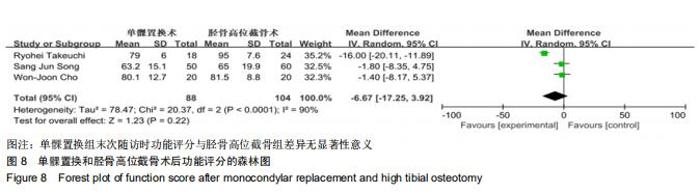
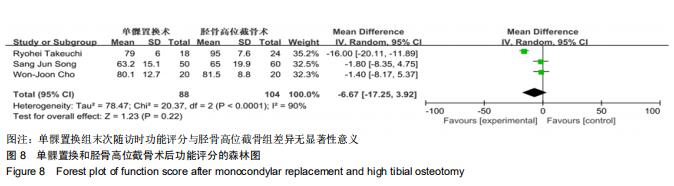
2.4.5 功能评分 有3篇文献比较了末次随访时功能评 分[6-7,9],共纳入192例患者进行Meta分析,单髁置换组88例,胫骨高位截骨组104例。Q检验,I2=90%,P < 0.000 01,显示3篇纳入文献异质较大,采用随机效应模型计算单髁置换组vs.胫骨高位截骨组的合并MD值为-6.67,95%CI(-17.25,3.92),P=0.22,结果显示单髁置换组末次随访时功能评分与胫骨高位截骨组差异无显著性意义,见图8。 "
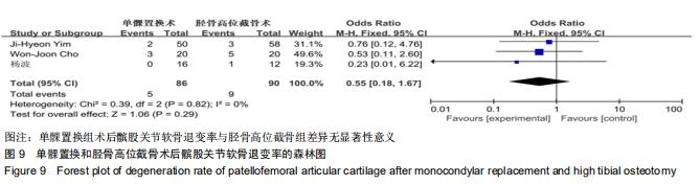
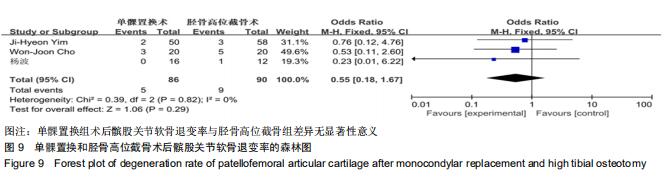
2.5.1 髌股关节软骨退变率 有3篇文献比较了末次随访髌股关节软骨退变率[7,11,19],共纳入176例患者进行Meta分析,单髁置换组86例,胫骨高位截骨组90例。Q检验,I2=0%,P=0.82,显示纳入的3篇文献异质性小,采用固定效应模型计算单髁置换组vs.胫骨高位截骨组的合并OR值为0.55,95%CI(0.18-1.67),P=0.29,结果显示单髁置换组术后髌股关节软骨退变率与胫骨高位截骨组差异无显著性意义,见图9。 "
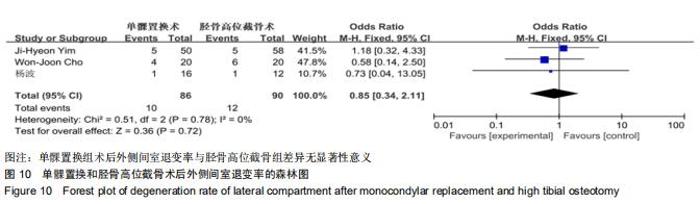
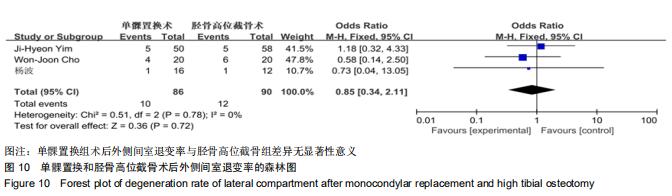
2.5.2 外侧间室退变率 有3篇文献比较了末次随访外侧间室退变率[7,11,19],共纳入176例患者进行Meta分析,单髁置换组86例,胫骨高位截骨组90例。Q检验,I2=0%,P=0.78,显示纳入的3篇文献异质性小,采用固定效应模型计算单髁置换组vs.胫骨高位截骨组的合并OR值为0.85,95%CI(0.34-2.11),P=0.72,结果显示单髁置换组术后外侧间室退变率与胫骨高位截骨组差异无显著性意义,见图10。 "
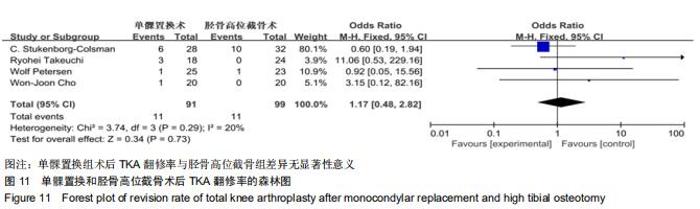
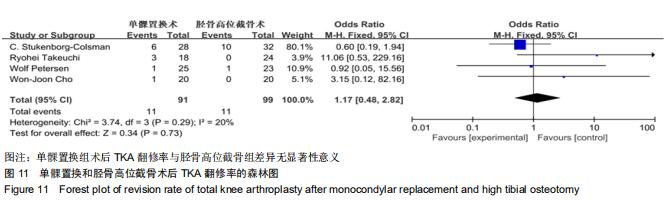
2.6 单髁置换和胫骨高位截骨术后TKA翻修率的Meta分析结果 有4篇文献比较了末次随访TKA翻修率[6-8,10],共纳入190例患者进行Meta分析,单髁置换组91例,胫骨高位截骨组99例。Q检验,I2=20%,P=0.29,显示纳入的4篇文献异质性小,采用固定效应模型计算单髁置换组vs.胫骨高位截骨组的合并OR值为1.17,95%CI(0.48-2.82),P=0.73,结果显示单髁置换组术后TKA翻修率与胫骨高位截骨组差异无显著性意义,见图11。 "
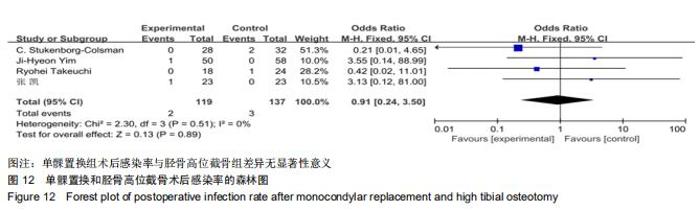
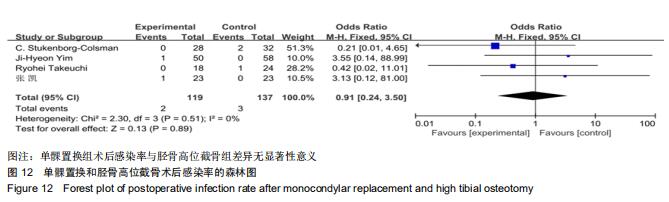
2.7 单髁置换和胫骨高位截骨术后感染率的Meta分析结果 有4篇文献比较了末次随访TKA翻修率[6,10-11,23],共纳入256例患者进行Meta分析,单髁置换组119例,胫骨高位截骨组137例。Q检验,I2=0%,P=0.51,显示纳入的4篇文献异质性小,采用固定效应模型计算单髁置换组vs.胫骨高位截骨组的合并OR值为0.91,95%CI(0.24-3.50),P=0.89,结果显示单髁置换组术后感染率与胫骨高位截骨组差异无显著性意义,见图12。 "
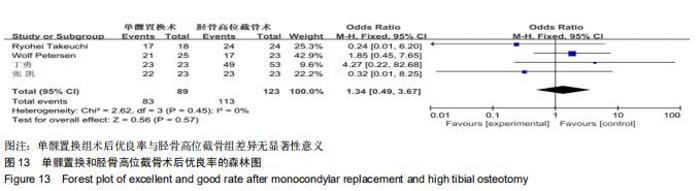
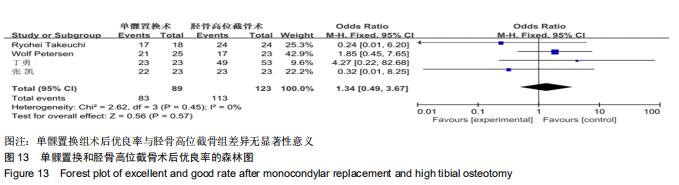
2.8 单髁置换和胫骨高位截骨术后优良率的Meta分析结果 有4篇文献比较了末次随访TKA翻修率[6,8,21,23],共纳入212例患者进行Meta分析,单髁置换组89例,胫骨高位截骨组123例。Q检验,I2=0%,P=0.45,显示纳入的4篇文献异质性小,采用固定效应模型计算单髁置换组vs.胫骨高位截骨组的合并OR值为1.34,95%CI(0.49-3.67),P=0.57,结果显示单髁置换组术后优良率与胫骨高位截骨组差异无显著性意义,见图13。 "
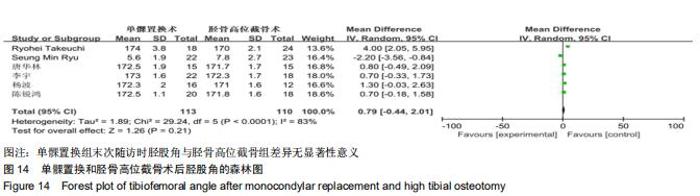
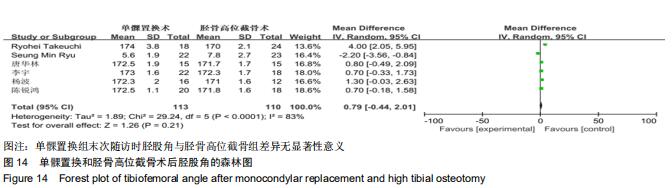
2.9 单髁置换和胫骨高位截骨术后胫股角的Meta分析结果 有6篇文献比较了末次随访时胫股角[2,6,19-20,22,24],共纳入223例患者进行Meta分析,单髁置换组113例,胫骨高位截骨组110例。Q检验,I2=83%,P < 0.000 1,显示6篇纳入文献异质性较大,采用随机效应模型计算单髁置换组vs.胫骨高位截骨组的合并MD值为0.79,95%CI(-0.44,2.01),P=0.21,结果显示单髁置换组末次随访时胫股角与胫骨高位截骨组差异无显著性意义,见图14。 "
|
[1] LOESER RF. Aging and osteoarthritis: the role of chondrocyte senescence and aging changes in the cartilage matrix. Osteoarthritis Cartilage. 2009;17(8):971-979.
[2] RYU SM, PARK JW, NA HD, et al. High Tibial Osteotomy versus Unicompartmental Knee Arthroplasty for Medial Compartment Arthrosis with Kissing Lesions in Relatively Young Patients. Knee Surg Relat Res. 2018;30(1):17-22.
[3] HAN SB, KYUNG HS, SEO IW, et al. Better clinical outcomes after unicompartmental knee arthroplasty when comparing with high tibial osteotomy. Medicine (Baltimore). 2017;96(50):e9268.
[4] DETTONI F, BONASIA DE, CASTOLDI F, et al. High tibial osteotomy versus unicompartmental knee arthroplasty for medial compartment arthrosis of the knee: a review of the literature. Iowa Orthop J. 2010;30:131-140.
[5] KIM YJ, KIM BH, YOO SH, et al. Mid-term results of oxford medial unicompartmental knee arthroplasty in young asian patients less than 60 years of age: a minimum 5-year follow-up. Knee Surg Relat Res. 2017;29(2):122-128.
[6] TAKEUCHI R, UMEMOTO Y, ARATAKE M, et al. A midterm comparison of open wedge high tibial osteotomy vs unicompartmental knee arthroplasty for medial compartment osteoarthritis of the knee. J Orthop Surg Res. 2010;5(1):65.
[7] CHO WJ, KIM JM, KIM WK, et al. Mobile-bearing unicompartmental knee arthroplasty in old-aged patients demonstrates superior short-term clinical outcomes to open-wedge high tibial osteotomy in middle-aged patients with advanced isolated medial osteoarthritis. Int Orthop. 2018;42(10): 2357-2363.
[8] PETERSEN W, METZLAFF S. Open wedge high tibial osteotomy (HTO) versus mobile bearing unicondylar medial joint replacement: five years results. Arch Orthop Trauma Surg. 2016; 136(7):983-989.
[9] SONG SJ, BAE DK, KIM KI, et al. Long-term survival is similar between closed-wedge high tibial osteotomy and unicompartmental knee arthroplasty in patients with similar demographics. Knee Surg Sports Traumatol Arthrosc. 2019; 27(4):1310-1319.
[10] STUKENBORG-COLSMAN C, WIRTH CJ, LAZOVIC D, et al. High tibial osteotomy versus unicompartmental joint replacement in unicompartmental knee joint osteoarthritis: 7-10-year follow-up prospective randomised study. Knee. 2001;8(3):187-194.
[11] YIM JH, SONG EK, SEO HY, et al. Comparison of high tibial osteotomy and unicompartmental knee arthroplasty at a minimum follow-up of 3 years. J Arthroplasty. 2013;28(2):243-247.
[12] BODE G, VON HEYDEN J, PESTKA J, et al. Prospective 5-year survival rate data following open-wedge valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2015;23(7): 1949-1955.
[13] BONASIA DE, DETTONI F, SITO G, et al. Medial opening wedge high tibial osteotomy for medial compartment overload/arthritis in the varus knee: prognostic factors. Am J Sports Med. 2014;42(3): 690-698.
[14] FU D, LI G, CHEN K, et al. Comparison of high tibial osteotomy and unicompartmental knee arthroplasty in the treatment of unicompartmental osteoarthritis: a meta-analysis. J Arthroplasty. 2013;28(5):759-765.
[15] HERRY Y, BATAILLER C, LORDING T, et al. Improved joint-line restitution in unicompartmental knee arthroplasty using a robotic- assisted surgical technique. Int Orthop. 2017;41(11): 2265-2271.
[16] SARAGAGLIA D, BEVAND A, REFAIE R, et al. Results with nine years mean follow up on one hundred and three KAPS(R) uni knee arthroplasties: eighty six medial and seventeen lateral. Int Orthop. 2018;42(5):1061-1066.
[17] RICHMOND JC. Surgery for osteoarthritis of the knee. Rheum Dis Clin North Am. 2013;39(1):203-211.
[18] SANTOSO MB, WU L. Unicompartmental knee arthroplasty, is it superior to high tibial osteotomy in treating unicompartmental osteoarthritis? A meta-analysis and systemic review. J Orthop Surg Res. 2017;12(1):50.
[19] 杨波,姜鑫.单髁置换术与胫骨高位截骨术治疗膝关节内侧间室骨关节炎的近期疗效比较[J].中国修复重建外科杂志,2015,29(5): 548-552.
[20] 唐华林,李玉军.单髁置换术与胫骨高位截骨术治疗膝骨性关节炎的效果对比分析[J].临床医药文献电子杂志,2017,4(77):15096-15097.
[21] 丁勇,李钊,胡运生,等.单髁置换术与胫骨高位截骨术治疗膝骨性关节炎疗效比较[J].生物骨科材料与临床研究,2015,12(2):75-77.
[22] 陈锐鸿,葛鸿庆,陈文治.单髁置换与胫骨高位截骨治疗膝关节内侧间室骨关节炎:1年随访比较[J].中国组织工程研究,2019,23(20): 3143-3147.
[23] 张凯,王晓鹏,戴志刚.胫骨高位截骨术与单髁置换术治疗膝内侧间室关节炎临床疗效对比[J].潍坊医学院学报, 2019,41(3):207-209.
[24] 李宇,王立志,郑秋,等.胫骨高位截骨与膝单髁置换治疗内侧间室骨关节炎的近期疗效比较[J].中国现代医学杂志, 2019,29(16):75-79.
[25] AMIN AK, PATTON JT, COOK RE, et al. Unicompartmental or total knee arthroplasty?: Results from a matched study. Clin Orthop Relat Res. 2006;451:101-106.
[26] KYUNG HS. High tibial osteotomy for medial knee osteoarthritis. Knee Surg Relat Res. 2016;28:253-254.
[27] PARKER DA, VISKONTAS DG. Osteotomy for the early varus arthritic knee. Sports Med Arthrosc. 2007;15:3-14.
[28] ENGH GA. Orthopaedic crossfire-can we justify unicondylar arthroplasty as a temporizing procedure? In the affirmative. J Arthroplasty. 2002;17:54-55.
[29] KO YB, GUJARATHI MR, OH KJ. Outcome of unicompartmental knee arthroplasty: a systematic review of comparative studies between fixed and mobile bearings focusing on complications. Knee Surg Relat Res. 2015;27:141-148.
[30] 宋伟,朱振国,徐进,等.单髁置换术与胫骨高位截骨术治疗膝关节骨性关节炎的荟萃分析[J].中国矫形外科杂志,2018,26(21): 1962-1968
[31] IVARSSON I, GILLQUIST J. Rehabilitation after high tibial osteotomy and unicompartmental arthroplasty. Clin Orthop Relat Res. 1991;266:139-144.
[32] ANDRIACCHI TP, GALANTE JO, FERMIER RW. The influence of total knee-replacement design on walking and stair-climbing. J Bone Joint Surg Am. 1982;64:1328-1335.
[33] WEINSTEIN JN, ANDRIACCHI TP, GALANTE J. Factors influencing walking and stair climbing following unicompartmental knee arthroplasty. J Arthroplasty. 986;1:109-115. [34] CARTIER P, SANOUILLER JL, GRELSAMER RP. Unicompartmental knee arthroplasty surgery. 10-year minimum follow-up period. J Arthroplasty. 1996;11:782-788. |
| [1] | Hu Kai, Qiao Xiaohong, Zhang Yonghong, Wang Dong, Qin Sihe. Treatment of displaced intra-articular calcaneal fractures with cannulated screws and plates: a meta-analysis of 15 randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1465-1470. |
| [2] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Comparison of the short-term efficacy of extracorporeal shock wave therapy for middle-aged and elderly knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1471-1476. |
| [3] | Li Dadi, Zhu Liang, Zheng Li, Zhao Fengchao. Correlation of total knee arthroplasty efficacy with satisfaction and personality characteristics [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1346-1350. |
| [4] | Wei Wei, Li Jian, Huang Linhai, Lan Mindong, Lu Xianwei, Huang Shaodong. Factors affecting fall fear in the first movement of elderly patients after total knee or hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1351-1355. |
| [5] | Wang Jinjun, Deng Zengfa, Liu Kang, He Zhiyong, Yu Xinping, Liang Jianji, Li Chen, Guo Zhouyang. Hemostatic effect and safety of intravenous drip of tranexamic acid combined with topical application of cocktail containing tranexamic acid in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1356-1361. |
| [6] | Xiao Guoqing, Liu Xuanze, Yan Yuhao, Zhong Xihong. Influencing factors of knee flexion limitation after total knee arthroplasty with posterior stabilized prostheses [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1362-1367. |
| [7] | Peng Zhihao, Feng Zongquan, Zou Yonggen, Niu Guoqing, Wu Feng. Relationship of lower limb force line and the progression of lateral compartment arthritis after unicompartmental knee arthroplasty with mobile bearing [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1368-1374. |
| [8] | Huang Zexiao, Yang Mei, Lin Shiwei, He Heyu. Correlation between the level of serum n-3 polyunsaturated fatty acids and quadriceps weakness in the early stage after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1375-1380. |
| [9] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [10] | Chen Jinping, Li Kui, Chen Qian, Guo Haoran, Zhang Yingbo, Wei Peng. Meta-analysis of the efficacy and safety of tranexamic acid in open spinal surgery [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1458-1464. |
| [11] | Wang Yongsheng, Wu Yang, Li Yanchun. Effect of acute high-intensity exercise on appetite hormones in adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1305-1312. |
| [12] | Liu Xiangxiang, Huang Yunmei, Chen Wenlie, Lin Ruhui, Lu Xiaodong, Li Zuanfang, Xu Yaye, Huang Meiya, Li Xihai. Ultrastructural changes of the white zone cells of the meniscus in a rat model of early osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1237-1242. |
| [13] | Kong Desheng, He Jingjing, Feng Baofeng, Guo Ruiyun, Asiamah Ernest Amponsah, Lü Fei, Zhang Shuhan, Zhang Xiaolin, Ma Jun, Cui Huixian. Efficacy of mesenchymal stem cells in the spinal cord injury of large animal models: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1142-1148. |
| [14] | Zhong Hehe, Sun Pengpeng, Sang Peng, Wu Shuhong, Liu Yi. Evaluation of knee stability after simulated reconstruction of the core ligament of the posterolateral complex [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 821-825. |
| [15] | Zhao Zhongyi, Li Yongzhen, Chen Feng, Ji Aiyu. Comparison of total knee arthroplasty and unicompartmental knee arthroplasty in treatment of traumatic osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 854-859. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||