Chinese Journal of Tissue Engineering Research ›› 2019, Vol. 23 ›› Issue (28): 4576-4583.doi: 10.3969/j.issn.2095-4344.1456
Previous Articles Next Articles
Preoperative clinical evaluation and surgical indication selection strategy of high tibial osteotomy
- 1Second Clinical Medical College of Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China; 2Second Affiliated Hospital of Guangzhou University of Chinese Medicine (Guangdong Provincial Hospital of Traditional Chinese Medicine), Guangzhou 510120, Guangdong Province, China
-
Online:2019-10-08Published:2019-10-08 -
Contact:Liu Jun, Chief physician, Professor, Doctoral supervisor, Second Affiliated Hospital of Guangzhou University of Chinese Medicine (Guangdong Provincial Hospital of Traditional Chinese Medicine), Guangzhou 510120, Guangdong Province, China -
About author:Hou Senrong, Second Clinical Medical College of Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China -
Supported by:the Guangdong Provincial Finance Department Project, Nos. [2014]157, [2018]8 (to LJ)| the Research Project of TCM Science and Technology in Guangdong Hospital of Traditional Chinese Medicine, Nos. YK2013B2N19, YN2015MS15 (to LJ)
CLC Number:
Cite this article
Hou Senrong, Pan Jianke, Yang Weiyi, Luo Minghui, Huang Hetao, Zeng Lingfeng, Lin Jiongtong, Han Yanhong, Liu Jun. Preoperative clinical evaluation and surgical indication selection strategy of high tibial osteotomy[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(28): 4576-4583.
share this article
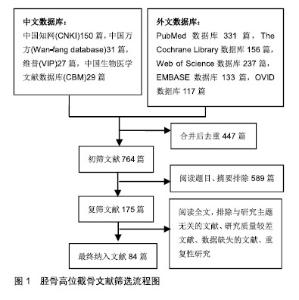
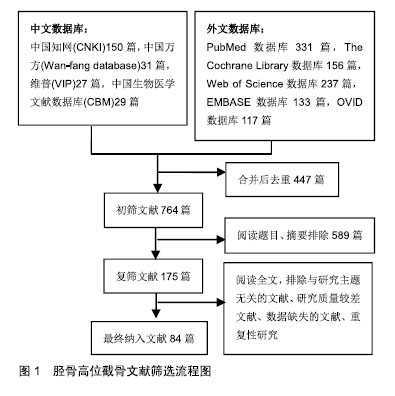
2.1 纳入资料基本概况 计算机初检,通过阅读文章题目及其摘要进行初步筛选,排除质量较差、重复或与文章主题不相关的文献,通篇阅读后,根据纳入标准和排除标准进行进一步筛查,最后纳入84篇与胫骨高位截骨相关的文献进行综述。 2.2 文献筛选流程图 见图1。"
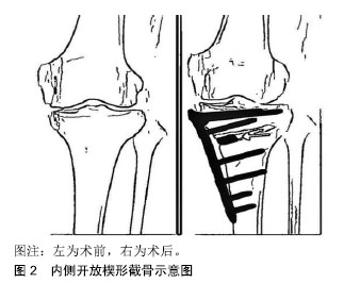
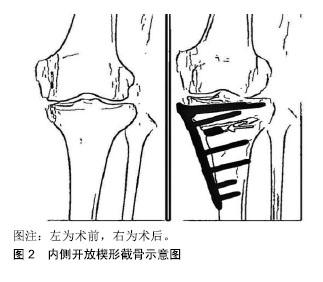
2.3 胫骨高位截骨术的种类 目前文献报道中较常见的胫骨高位截骨方式主要包括内侧开放楔形截骨、外侧闭合楔形截骨、胫骨髁外翻截骨术以及穹顶样截骨术等截骨方式[2],前2种高位截骨手术则是目前临床采用较多的术式。 2.3.1 内侧开放楔形截骨术 因其手术切口较小,且技术难度相对较低,是当前临床常用截骨术中优势较为明显的手术方式。因内侧开放楔形截骨在术中可继续调节力线,可更好地调整截骨,以及三平面和更加精确地矫正畸形[23]。内侧开放楔形截骨可保留外侧骨性合页,可避免截骨端移位,不易造成骨质流失,没有缩短肢体。一般不需要进行腓骨截骨,故而可最大程度地避免腓总神经损伤。在出现手术失败或膝骨关节炎后期手术翻修时更易转换到关节置换[24]。但若截骨面撑开过大,则需要进行骨移植,这也同时增加了骨愈合延迟或骨不愈合的风险[2,25-28]。基于内侧开放楔形截骨疗效等各方面因素的综合影响,在相关领域内,内侧开放楔形截骨近年愈加受临床骨科医生的青睐[17,29-30]。内侧开放楔形截骨示意图见图2。"

2.3.2 外侧闭合楔形截骨术 是最早开展的截骨手术方式之一。很长一段时间内,外侧闭合楔形截骨被认为是治疗内侧间室关节炎这一领域内的金标准[31-33]。外侧闭合楔形截骨具有较为优良的初始稳定性,无需植骨,且较之于内侧开放楔形截骨,其手术截骨部位为完整的骨性面接触,基于截骨端的加压使其具有更高的术后愈合率[34-36]。然而,因手术需行腓骨截骨或上胫腓关节分离,故此也极大地增加了腓总神经损伤的风险。但外侧闭合楔形截骨往往会造成解剖结构的改变,且有时矫正角度也相对较大,二者皆加大了后续全膝关节置换的难度。此外,此术很难得到轴的逐渐修正。有研究发现,外侧闭合楔形截骨与内侧开放楔形截骨2种手术方式的效果并无明显差异,且部分研究表明二者后续全膝关节置换手术后关节功能结局、存活率及并发症发生率差异无显著性意义[37-38]。Kim等[39]的一项回顾性研究则发现,开放楔形和闭式楔形截骨在5年生存率方面没有差异,但在10年生存率的比较中,内侧开放楔形截骨的生存率[91.6%(95%CI:88.5%-94.8%)]则高于外侧闭合楔形截骨[85.4%(95%CI:84.0%-86.7%)]。 2.3.3 胫骨髁外翻截骨术 由于胫骨髁外翻截骨术在胫骨近端行“L”形截骨,又称为L型高位胫骨截骨术。不同于前2种手术方式,它是一种关节内开放式的截骨技术,可以对膝关节面进行一定的适应性调整,且不追求精确的计算矫正角度。Chiba等[40]的研究同样确定了胫骨髁外翻截骨术的疗效。但不同于其他截骨术,Kettelkamp等[41]认为,胫骨髁外翻截骨术无法矫正中重度膝关节内侧间室膝骨关节炎患者存在的关节内畸形[2]。 2.3.4 穹顶样截骨术 并不会引起下肢长度的明显改变,在纠正及调整角度方面具有一定优势[42]。手术并不造成骨量丢失,且允许患者早期下地活动,术后愈合相对较快。但由于手术难度较大,且手术创口较大,故目前临床较少使用[43-44]。 以上4种胫骨高位截骨方式各有优劣,无论使用哪种手术方式,其术前临床评估与手术适应证的选择都极为重要。 2.4 胫骨高位截骨术前临床评估及手术适应证选择 理想的患者选择是胫骨高位截骨成功的决定性因素之一。随着临床研究数据的积累,胫骨高位截骨的手术适应证及禁忌证也逐渐发生变化[33]。尽管目前胫骨高位截骨的手术适应证的选择仍存在争议,但年龄、体质量指数、膝关节的磨损部位、关节面磨损程度、关节内外翻的程度等因素都明显与胫骨高位截骨手术结果及生存率有关。 2.4.1 年龄 年龄一直以来都是影响胫骨高位截骨手术效果及术后生存率的重要因素之一。胫骨高位截骨的理想手术患者年龄范围为< 65岁膝关节炎患者[45]。即便有部分研究发现年龄对术后的临床和放射学结果无影响[46-47],国外专家也认为年龄与胫骨高位截骨术后牛津关节评分无明显联系[48],且有学者认为在拥有丰富手术经验及谨慎的适应证选择的前提下,胫骨高位截骨对高龄老人(>70岁)同样有效[49],但一般仍认为65岁以上老年患者不宜行胫骨高位截骨术治疗,为胫骨高位截骨手术禁忌患者。 Bonasia等[50]认为年龄是与不良结局有显著关系的变量,其在一项纳入99例患者的研究中发现发现年龄是一个与不良结果显著相关术前变量,年龄大于56岁的患者手术失败的风险高出5倍。Trieb等[51]的研究则发现,65岁以上患者胫骨高位截骨失败的风险明显高于年轻患者[失败率(38.4±11.3)% vs. (23.1±5.8)%],相对风险为1.5 (P=0.0461),年龄每增长1岁,其手术失败的风险增加7.6%。Sabzevari等[52]则认为胫骨高位截骨最合适的年龄范围是40-60岁;Howells等[53]发现生存率的提高明显与年龄小于55岁这一因素相关;而Flecher等[54]则认为翻修的最重要危险因素之一是年龄大于50岁;Koh等[55]研究发现年轻患者对胫骨高位截骨的满意度相对较高。若将胫骨高位截骨失败定义为再次手术改为全膝关节置换术,Keenan等[56]则认为47岁以上女性过早转入全膝关节置换的风险显著增加。 综上,考虑到65岁以上老年患者因膝关节外侧软骨也相应出现退行性变,转移力线后更易加速外侧软骨磨损,每年失败风险的增加和较高的失败率,故65岁以上的患者慎行胫骨高位截骨。尽管有观点认为胫骨高位截骨几乎没有年龄的下限,只要骨骺闭合便可以适用,然而在足够的术前功能评分的前提下,有研究则证明55岁以上的患者其生存率、功能结果均要优于年轻患者。故胫骨高位截骨目前最理想的年龄范围可能为40-65岁。 2.4.2 体质量指数 目前体质量指数与开放楔形胫骨高位截骨术结果之间的关系在文献中存在不小的争议,大多数专家学者认为小于30 kg/m2的体质量指数往往具有更好的结果,当体质量指数>30 kg/m2时,胫骨高位截骨手术失败概率同比增加10倍[50,53-54,57]。Akizuki等[58]对132例患者进行了前瞻性研究,这些患者在1988至1997年接受了闭合楔形胫骨高位截骨术治疗严重的内侧室骨关节炎,其研究指出,术前体质量指数大于27.5 kg/m2是预测早期失败的危险因素。体质量指数的正常值为18.5-24.9 kg/m2,Giagounidis等[59]对94例胫骨高位截骨患者进行了平均9年的随访,其研究数据表明,体质量指数高于正常值10%的患者无痛期为5.07年,而体质量指数低于正常值10%的患者其无痛期可达7.80年。Yokoyama等[60]2008至2011年对47例接受了开放楔形截骨治疗的患者进行了研究随访,发现体质量指数较高的患者和女性的愈合期往往较长,晚期愈合组平均体质量指数(28.3±0.4)kg/m2明显高于早期愈合组(25.7±1.6)kg/m2。Sprenger等[61]对66例接受了胫骨高位截骨手术治疗的内侧室关节病患者术后进行了平均10.8年的随访,发现较高的体质量指数是早期手术失败的重要影响因素。 早在1978年有研究对54例胫骨高位截骨手术患者在术前及术后6年进行关节镜检查,发现了关节软骨的修复现象。Jung等[62]的研究也同样证实了这一点,但这一修复能力究竟是软骨本身的再生能力还是内部其他组织细胞的修复能力则有待进一步考证[63]。Kumagai等[64]认为年龄、性别并不会对胫骨高位截骨术后软骨再生产生影响,但较低的体质量指数则明显有利于软骨再生。而后续Takeuchi等[65]对30例内侧开放楔形截骨术后患者进行24-62个月不等的随访研究也证实了膝关节内软骨的可再生性。故从软骨再生的角度出发,体质量指数应为首先考虑的因素。在总结了多项与体质量指数相关的研究后,Loia等[45]认为胫骨高位截骨的理想体质量指数值应在25-27.5 kg/m2之间。 既往研究固然表明体质量指数过大不利于胫骨高位截骨,但体质量指数也并非越小越好。早在1999年,Naudie等[66]通过对106例胫骨高位截骨手术在至少10年的随访后,对其统计结果经多变量Cox回归分析显示,体质量指数<25 kg/m2的患者中,其胫骨延迟愈合或不愈合的发生与早期失败的概率显著相关。 2.4.3 骨关节炎等级 根据影像学检查,可对膝骨关节炎的分期主要有Kellgren-Lawrence分级、Ahlback分级法、David区分法以及Holden分级等分级法,其中前2种分级方法为目前临床胫骨高位截骨术前评估中最常采用的分级方法[67]。 胫骨高位截骨原理是通过纠正膝关节承重轴、将负荷从内侧隔室向外侧移动,从而缓解膝关节疼痛症状,达到保膝的目的。由于内侧面高压解除,纤维软骨得以形成,甚至一定程度上可以扭转关节软骨磨损的境况。若外侧膝关节磨损,力轴的改变则会加速其磨损过程,使得反而无法缓解疼痛。胫骨高位截骨术前评估时,外侧软骨必须是完好的,否则是胫骨高位截骨绝对禁忌证。 目前,学界多以Ahlback分级作为胫骨高位截骨术前内侧膝骨关节炎评估的指标,大多数人认为Ahlback Ⅱ及以下的患者是较为理想的胫骨高位截骨适应证患者。Flecher等[54]研究数据表明,理想的闭合楔状胫骨高位截骨患者是股骨内侧骨关节炎程度相对较轻(Ahlback等级<Ⅲ)的患者。Efe等[47]则是认为胫骨高位截骨失败的一个重要危险因素是术前Kellgren-Lawrence骨关节炎等级>Ⅱ。Koh等[55]的一项回顾性分析也证实了严重骨关节炎与胫骨高位截骨术后不满的风险增加有关(P < 0.01)。Ivarsson等[68]观察到在截骨术前患有Ⅰ级或Ⅱ级骨关节炎和外翻偏离的患者其胫骨高位截骨术后随访反馈到的结果最佳。当膝关节内侧软骨完好到完全磨损但尚未侵蚀到软骨下骨时(Ahlback等级≤Ⅲ级),胫骨高位截骨结果良好,在文献中没有发现任何证据表明将力线转向侧隔间会使这个隔间的状况恶化[50,57]。 在相关领域内,内侧隔间骨关节炎的严重程度也是胫骨高位截骨术后结果的相关预测指标,,尽管目前具体骨关节炎严重程度仍未有统一定论,但目前学界普遍认为内侧室骨关节炎较严重(Ahlback Ⅲ级,轻度骨磨损或更高,中度骨磨损,骨对骨阶段)不适合截骨,应作为胫骨高位截骨的禁忌证,Aglietti等[69]早在其1983年发表的文章中也对这一观点持肯定态度,他在对139例胫骨高位截骨患者作了至少10年的随访期后发现,有64%的手术效果优异或良好,且在其中Ⅰ级或Ⅱ级骨关节炎理想患者4年的术后随访评估中88%具有优异或良好的结果,显然Ahlback等级较低的患者的手术结果更佳。Flecher等[54]对301例接受胫骨高位截骨的患者进行了平均为期18年的长期随访后发现31例需要翻修的患者中有23例(74%)在首次胫骨高位截骨术前被分类为Ahlback Ⅲ,故他们预测胫骨高位截骨术后失败翻修的最重要的风险因素是年龄大于50岁和术前关节炎Ahlback等级为Ⅲ或更高。同时也有作者提出三室骨性关节炎也是截骨禁忌证[57,68-69]。 2.4.4 胫骨内翻程度 胫骨高位截骨既能缓解因内侧膝关节磨损造成的疼痛,又可矫正关节外畸形。有文献对217例胫骨高位截骨术后患者进行了平均9年后的长期随访研究,结果表明,关节外畸形(膝关节内翻)< 0°的患者,术后满意度为36%;关节外畸形为0°到2°的患者,术后满意度为56%;关节外畸形为2°到5°的患者,术后满意度为71%;关节外畸形>5°的时候,患者术后满意度可达83%[70]。故Bonnin等[70]认为胫骨内翻>5°,胫骨近端内侧角<85°是胫骨高位截骨的必要条件。而部分作者则认为胫骨内翻>10°是胫骨高位截骨的强适应证。Rudan等[71]的一项前瞻性研究数据结果表明,在纳入的79例胫骨高位截骨术后患者80%的有良好或优异的结果,对外翻6°和14°之间的股胫角进行校正与最佳临床结果相关,且矫正不够(<5°)的膝外翻会有较高的失败率(62.5%)这与Bonnin等[70]的最终结论有一致性。故此,有理由认为胫骨内翻程度过小均不利于胫骨高位截骨的结果,有限的文献证据表明理想的胫骨高位截骨手术适应证胫骨内翻应>5°,胫骨近端内侧角<85°。 2.4.5 运动范围 人体正常膝关节活动范围屈曲为120°-150°,过伸为5°-10°,屈膝时内外旋分别为10°和20°。在膝骨关节炎相关领域内,通常用到运动范围来指代患者关节的运动范围,一般为患者的屈曲范围。运动范围是胫骨高位截骨术前评估的一项重要指标,但不同研究作者对运动范围的研究结果也不尽相同。 有研究指出,运动范围<90°早期失败密切相关,结果良好的患者通常术前活动范围至少为90°[9]。Akizuki等[58]对纳入的94例接受外侧闭合楔形截骨治疗的严重内侧室骨关节炎患者的前瞻性研究中,对他们展开了16-20年的随访,术前膝关节运动范围小于100°是预测早期失败的危险因素。Naudie等[66]对85例患者进行了至少10年的随访评估,以确定其存活率,并发症和与衰竭相关的危险因素,发现术前运动范围低于120°同时屈曲挛缩大于5°与胫骨高位截骨早期失败有密切联系。国内也有作者则发现运动范围为(125.21±4.77)°的单间室骨性关节炎伴后交叉韧带损伤患者采用胫骨高位截骨结合后交叉韧带重建治疗可取得良好的近期疗效[72]。除此之外,其他不少文献同样有证据表明在膝关节活动度低于120°时,胫骨高位截骨的手术结果不良的风险通常较高[24,73]。故此,运动范围<120°、屈曲挛缩> 5°通常都被当做是胫骨高位截骨手术的禁忌证,而当患者膝关节活动度与正常膝关节活动度接近时,则较适合胫骨高位截骨。 2.4.6 膝关节的稳定性 膝关节稳定与否是关乎着胫骨高位截骨最终结果的一项重要因素。下肢韧带稳定的下肢原发性内翻畸形是胫骨高位截骨的最佳适应证。内翻性骨畸形伴韧带不稳定,主要是前交叉韧带损伤造成的。术前患者膝内翻伴膝外摆步态通常与内翻性骨畸形伴中心韧带功能不全和后外侧角损伤有关。研究表明胫骨高位截骨适用于这2种类型的膝关节不稳,在日常生活和运动活动中疼痛、肿胀、疼痛和功能的改善有统计学意义[74]。国内外临床研究结果发现开放楔形截骨同样适用于后外侧角损伤伴前交叉韧带损伤伴韧带不稳定[75-76]。部分文献表明前胫骨高位截骨术和前交叉韧带重建适用于交叉韧带损伤伴冠状面或矢状面对线不良单节段,而在慢性前交叉韧带损伤伴内翻畸形建议单独胫骨高位截骨或联合重建前交叉韧带,但若存在残余不稳定性,则通常需延迟后交叉韧带重建[77]。而近期的研究同样发现前交叉韧带缺损内翻-膝关节骨折患者不仅需要行单独胫骨高位截骨,还需要额外的前交叉韧带重建术[78]。 2.4.7 其他因素 影响胫骨高位截骨结果的因素多种多样,除了以上6种重要因素外,运动需求、半月板功能等也同样是胫骨高位截骨术前评估的需要重点考量的范畴。 (1)很少有作者把恢复体育活动或恢复体力劳动能力作为截骨术后的预后标准。Nagel等[79]对34例胫骨高位截骨术后患者进行了回顾性研究,根据Tegner和Lysholm的系统评估功能结果,其中参与工作和体育活动的水平按照从0分(完全残疾)到10分(精英职业运动员水平上表现的能力)的等级进行评分。术前平均功能评分为5.4分(范围2-8分),术后平均4.8分(范围1-8分)。术后许多胫骨高位截骨术后的患者可能允许参加部分剧烈活动,例如跑步和跳跃等,而这在全膝关节置换术后是禁忌的,因为这可能导致全膝关节置换部件损伤,术后满意度达82%。Odenbring等[80]及Korovessis等[81]有限的研究结果也表明胫骨高位截骨适用于有恢复运动需求的患者。 (2)功能评分:Howells等[53]在一项纳入95例外侧闭合楔形截骨患者的10年长期随访研究表明,年龄在55岁以上的患者,在有足够的术前功能评分(日本骨科协会膝关节评分66.7分以上,西安大略和麦克马斯特大学骨关节炎指数45分以上)的前提下,其生存率较好,术后功能结果明显优于年轻患者,故对于考虑进行胫骨高位截骨术的患者,建议胫骨高位截骨术前常规使用功能性评分指数进行临床评估。 (3)半月板功能异常的患者应先予半月板修复等手术改善半月板功能后,方可考虑胫骨高位截骨,否则与“宝塔形”胫骨关节面一样同属胫骨高位截骨禁忌证[52,78]。 (4)因为胫骨高位截骨术及单髁置换术虽能极大程度缓解患者膝关节疼痛,但部分术后会残留一定程度的疼痛,故而需要患者有一定的疼痛的耐受能力。 (5)吸烟、嗜酒、高血压、糖尿病等也是影响胫骨高位截骨结果的一方面因素,而Miller等[82]的研究结果表明,重度吸烟患者胫骨高位截骨术后不愈合率明显升高,也是胫骨高位截骨的禁 忌证之一。而Cotter等[83]的研究也有类似的结论。 "

| [1]Hantes ME, Natsaridis P, Koutalos AA, et al. Satisfactory functional and radiological outcomes can be expected in young patients under 45 years old after open wedge high tibial osteotomy in a long-term follow-up. Knee Surg Sports Traumatol Arthrosc. 2018;26(11):3199-3205.[2]骆巍,马信龙,黄竞敏. 高位胫骨截骨术研究进展[J]. 中国矫形外科杂志,2018,26(19):1786-1789.[3]Lee DC, Byun SJ. High tibial osteotomy. Knee Surg Relat Res. 2012;24(2):61-69.[4]赵蔚峰,段戡,袁长深,等. 膝骨关节炎的非全膝关节置换术手术治疗进展[J]. 中国矫形外科杂志,2016,24(17):1593-1596.[5]于沂阳,常恒瑞,张英泽. 保膝治疗的研究进展[J]. 中华关节外科杂志(电子版),2017,11(1):73-77.[6]White SH, Ludkowski PF, Goodfellow JW. Anteromedial osteoarthritis of the knee. J Bone Joint Surg Br. 1991;73(4):582-586.[7]张英泽,李存祥,李冀东,等. 不均匀沉降在膝关节退变及内翻过程中机制的研究[J]. 河北医科大学学报,2014,35(2):218-219.[8]Ritter MA, Fechtman RA. Proximal tibial osteotomy. A survivorship analysis. J Arthroplasty. 1988;3(4):309-311.[9]Berman AT, Bosacco SJ, Kirshner S, et al. Factors influencing long-term results in high tibial osteotomy. Clin OrthopRelat Res. 1991;(272):192-198.[10]Chillag KJ, Nicholls PJ. High tibial osteotomy: a retrospective analysis of 30 cases. Orthopedics. 1984;7(12):1821-1822.[11]Hernigou P, Medevielle D, Debeyre J, et al. Proximal tibial osteotomy for osteoarthritis with varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg Am.1987;69(3):332-354.[12]Odenbring S, Tjornstrand B, Egund N, et al. Function after tibial osteotomy for medial gonarthrosis below aged 50 years. Acta Orthop Scand. 1989;60(5):527-531.[13]Saito T, Kumagai K, Akamatsu Y, et al. Five- to ten-year outcome following medial opening-wedge high tibial osteotomy with rigid plate fixation in combination with an artificial bone substitute. Bone Joint J. 2014;96-B(3):339-344.[14]Roberson TA, Momaya AM, Adams K, et al. High tibial osteotomy performed with all-peek implants demonstrates similar outcomes but less hardware removal at minimum 2-year follow-up compared with metal plates. Orthop J Sports Med. 2018;6(3): 1808797008.[15]Borjesson M, Weidenhielm L, Mattsson E, et al. Gait and clinical measurements in patients with knee osteoarthritis after surgery: a prospective 5-year follow-up study. Knee. 2005;12(2):121-127.[16]Stukenborg-Colsman C, Wirth CJ, Lazovic D, et al. High tibial osteotomy versus unicompartmental joint replacement in unicompartmental knee joint osteoarthritis: 7-10-year follow-up prospective randomised study. Knee. 2001;8(3):187-194.[17]Brouwer RW, Raaij VT, Bierma-Zeinstra SM, et al. Osteotomy for treating knee osteoarthritis. Cochrane Database Syst Rev. 2007; (3):D4019.[18]Cao Z, Mai X, Wang J, et al. Unicompartmental knee arthroplasty vs high tibial osteotomy for knee osteoarthritis: a systematic review and meta-analysis. J Arthroplasty. 2018;33(3):952-959.[19]Fu YW, Liu BG, Luo J, et al. Meta analysis of unilateral condylar replacement and high tibial osteotomy in the treatment of medial compartment osteoarthritis of the knee. Zhongguo Gu Shang. 2018;31(12):1156-1163.[20]Rodriguez-Merchan EC. Unicompartmental Knee Osteoarthritis (UKOA): Unicompartmental Knee Arthroplasty (UKA) or High Tibial Osteotomy (HTO)? Arch Bone Jt Surg. 2016;4(4):307-313.[21]Fu D, Li G, Chen K, et al. Comparison of high tibial osteotomy and unicompartmental knee arthroplasty in the treatment of unicompartmental osteoarthritis: a meta-analysis. J Arthroplasty. 2013;28(5):759-765.[22]Spahn G, Hofmann GO, von Engelhardt LV, et al. The impact of a high tibial valgus osteotomy and unicondylar medial arthroplasty on the treatment for knee osteoarthritis: a meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):96-112.[23]Han SB, Lee JH, Kim SG, et al. Patient-reported outcomes correlate with functional scores after opening-wedge high tibial osteotomy: a clinical study. Int Orthop. 2018;42(5):1067-1074.[24]Amendola A, Bonasia DE. Results of high tibial osteotomy: review of the literature. Int Orthop. 2010;34(2):155-160.[25]Ruangsomboon P, Chareancholvanich K, Harnroongroj T, et al. Survivorship of medial opening wedge high tibial osteotomy in the elderly: two to ten years of follow up. Int Orthop.2017;41(10): 2045-2052.[26]Pipino G, Indelli PF, Tigani D, et al. Opening-wedge high tibial osteotomy: a seven - to twelve-year study. Joints. 2016;4(1):6-11.[27]Woodacre T, Ricketts M, Evans JT, et al. Complications associated with opening wedge high tibial osteotomy--A review of the literature and of 15 years of experience. Knee. 2016;23(2):276-282.[28]Duivenvoorden T, van Diggele P, Reijman M, et al. Adverse events and survival after closing- and opening-wedge high tibial osteotomy: a comparative study of 412 patients. Knee Surg Sports Traumatol Arthrosc. 2017;25(3):895-901.[29]Webb M, Dewan V, Elson D. Functional results following high tibial osteotomy: a review of the literature. Eur J Orthop Surg Traumatol. 2018;28(4):555-563.[30]Coventry MB. Osteotomy about the knee for degenerative and rheumatoid arthritis. J Bone Joint Surg Am. 1973;55(1):23-48.[31]Jackson JP, Waugh W. Tibial Osteotomy for Osteoarthritis of the Knee. Proc R Soc Med. 1960;53(10):888.[32]Coventry MB. Osteotomy about the knee for degenerative and rheumatoid arthritis. J Bone Joint Surg Am. 1973;55(1):23-48.[33]金成,魏勇,胡继超. 胫骨高位截骨术的研究进展[J]. 浙江创伤外科,2018,23(4):848-850.[34]Duivenvoorden T, Brouwer RW, Baan A, et al. Comparison of closing- wedge and opening-wedge high tibial osteotomy for medial compartment osteoarthritis of the knee: a randomized controlled trial with a six-year follow-up. J Bone Joint Surg Am. 2014;96(17):1425-1432.[35]Song EK, Seon JK, Park SJ, et al. The complications of high tibial osteotomy: closing- versus opening-wedge methods. J Bone Joint Surg Br. 2010;92(9):1245-1252.[36]van Houten AH, Heesterbeek PJ, van Heerwaarden RJ, et al. Medial open wedge high tibial osteotomy: can delayed or nonunion be predicted? Clin OrthopRelat Res. 2014;472(4):1217-1223.[37]Preston S, Howard J, Naudie D, et al. Total knee arthroplasty after high tibial osteotomy: no differences between medial and lateral osteotomy approaches.Clin OrthopRelat Res.2014;472(1): 105-110.[38]Bastos FR, Magnussen RA, Duthon V, et al. Total knee arthroplasty after high tibial osteotomy: a comparison of opening and closing wedge osteotomy. Int Orthop. 2013;37(3):427-431.[39]Kim JH, Kim HJ, Lee DH. Survival of opening versus closing wedge high tibial osteotomy: A meta-analysis. Sci Rep. 2017;7(1):7296.[40]Chiba K, Yonekura A, Miyamoto T, et al. Tibial condylar valgus osteotomy (TCVO) for osteoarthritis of the knee: 5-year clinical and radiological results. Arch Orthop Trauma Surg. 2017;137(3): 303-310.[41]Kettelkamp DB, Leach RE, Nasca R. Pitfalls of proximal tibial osteotomy. Clin OrthopRelat Res. 1975;(106):232-241.[42]Chiang H, Hsu HC, Jiang CC. Dome-shaped high tibial osteotomy: a long-term follow-up study. J Formos Med Assoc.2006;105(3):214-219.[43]Hankemeier S, Paley D, Pape HC, et al. [Knee para-articular focal dome osteotomy]. Orthopade. 2004;33(2):170-177.[44]Schroter S, Konstantinidis L, Kraus TM, et al. Open wedge re-correction high tibial osteotomy in an elderly patient with a varus angulated non-united dome-shaped high tibial osteotomy. J Zhejiang Univ Sci B. 2013;14(11):1054-1058.[45]Loia MC, Vanni S, Rosso F, et al. High tibial osteotomy in varus knees: indications and limits. Joints. 2016;4(2):98-110.[46]Goshima K, Sawaguchi T, Sakagoshi D, et al. Age does not affect the clinical and radiological outcomes after open-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc.2017;25(3):918-923.[47]Efe T, Ahmed G, Heyse T, et al. Closing-wedge high tibial osteotomy: survival and risk factor analysis at long-term follow up. BMC Musculoskelet Disord. 2011;12:46.[48]Floerkemeier S, Staubli AE, Schroeter S, et al. Outcome after high tibial open-wedge osteotomy: a retrospective evaluation of 533 patients. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):170-180.[49]黄野. 胫骨高位截骨术治疗膝关节骨关节炎的现状[J]. 中华关节外科杂志(电子版),2016,10(5):470-473.[50]Bonasia DE, Dettoni F, Sito G, et al. Medial opening wedge high tibial osteotomy for medial compartment overload/arthritis in the varus knee: prognostic factors. Am J Sports Med. 2014;42(3):690-698.[51]Trieb K, Grohs J, Hanslik-Schnabel B, et al. Age predicts outcome of high-tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2006;14(2):149-152.[52]Sabzevari S, Ebrahimpour A, Roudi MK, et al. High Tibial Osteotomy: A Systematic Review and Current Concept. Arch Bone Jt Surg. 2016;4(3):204-212.[53]Howells NR, Salmon L, Waller A, et al. The outcome at ten years of lateral closing-wedge high tibial osteotomy: determinants of survival and functional outcome. Bone Joint J. 2014;96-B(11):1491-1497.[54]Flecher X, Parratte S, Aubaniac JM, et al. A 12-28-year followup study of closing wedge high tibial osteotomy. Clin Orthop Relat Res. 2006;452:91-96.[55]Koh IJ, Kim MS, Sohn S, et al. Predictive factors for satisfaction after contemporary unicompartmental knee arthroplasty and high tibial osteotomy in isolated medial femorotibial osteoarthritis. OrthopTraumatol Surg Res. 2018.[56]Keenan O, Clement ND, Nutton R, et al. Older age and female gender are independent predictors of early conversion to total knee arthroplasty after high tibial osteotomy. Knee. 2019;26(1):207-212.[57]Niemeyer P, Stohr A, Kohne M, et al. Medial opening wedge high tibial osteotomy. OperOrthop Traumatol. 2017;29(4):294-305.[58]Akizuki S, Shibakawa A, Takizawa T, et al. The long-term outcome of high tibial osteotomy: a ten- to 20-year follow-up. J Bone Joint Surg Br. 2008;90(5):592-596.[59]Giagounidis EM, Sell S. High tibial osteotomy: factors influencing the duration of satisfactory function. Arch Orthop Trauma Surg. 1999;119(7-8):445-449.[60]Yokoyama M, Nakamura Y, Onishi T, et al. Healing period after open high tibial osteotomy and related factors: Can we really say that it is long? Springerplus. 2016;5:123.[61]Sprenger TR, Doerzbacher JF. Tibial osteotomy for the treatment of varusgonarthrosis. Survival and failure analysis to twenty-two years. J Bone Joint Surg Am. 2003;85-A(3):469-474.[62]Jung WH, Takeuchi R, Chun CW, et al. Second-look arthroscopic assessment of cartilage regeneration after medial opening-wedge high tibial osteotomy. Arthroscopy. 2014;30(1):72-79.[63]Ushijima T. Arthroscopic Findings of Articular Cartilage and Radiographic Assessment after High Tibial Osteotomy for Spontaneous Osteonecrosis of the Knee. 2010.[64]Kumagai K, Akamatsu Y, Kobayashi H, et al. Factors affecting cartilage repair after medial opening-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2017;25(3):779-784.[65]Takeuchi R, Aratake M, Bito H, et al. Clinical results and radiographical evaluation of opening wedge high tibial osteotomy for spontaneous osteonecrosis of the knee. Knee Surg Sports Traumatol Arthrosc. 2009;17(4):361-368.[66]Naudie D, Bourne RB, Rorabeck CH, et al. The Install Award. Survivorship of the high tibial valgus osteotomy. A 10- to -22-year followup study. Clin Orthop Relat Res. 1999;(367):18-27.[67]Ahlback S. Osteoarthrosis of the knee. A radiographic investigation. Acta Radiol Diagn (Stockh). 1968:277.[68]Ivarsson I, Myrnerts R, Gillquist J. High tibial osteotomy for medial osteoarthritis of the knee. A 5 to 7 and 11 year follow-up. J Bone Joint Surg Br.1990;72(2):238-244.[69]Aglietti P, Rinonapoli E, Stringa G, et al. Tibial osteotomy for the varus osteoarthritic knee. Clin Orthop Relat Res.1983;(176): 239-251.[70]Bonnin M, Chambat P. Current status of valgus angle, tibial head closing wedge osteotomy in media gonarthrosis. Orthopade. 2004; 33(2):135-142.[71]Rudan JF, Simurda MA. High tibial osteotomy. A prospective clinical and roentgenographic review. Clin Orthop Relat Res. 1990; (255):251-256.[72]刘丙立,王雪,戴士峰. 膝内翻骨关节炎伴后交叉韧带损伤的同期治疗[J]. 中国修复重建外科杂志,2016,30(1):6-9.[73]Dettoni F, Bonasia DE, Castoldi F, et al. High tibial osteotomy versus unicompartmental knee arthroplasty for medial compartment arthrosis of the knee: a review of the literature. Iowa Orthop J. 2010;30:131-140.[74]Noyes FR, Barber-Westin SD, Hewett TE. High tibial osteotomy and ligament reconstruction for varus angulated anterior cruciate ligament-deficient knees. Am J Sports Med. 2000;28(3):282-296.[75]Rossi R, Bonasia DE, Amendola A. The role of high tibial osteotomy in the varus knee. J Am Acad Orthop Surg. 2011;19(10):590-599.[76]Jin C, Song EK, Jin QH, et al. Outcomes of simultaneous high tibial osteotomy and anterior cruciate ligament reconstruction in anterior cruciate ligament deficient knee with osteoarthritis. BMC Musculoskelet Disord. 2018;19(1):228.[77]Arthur A, Laprade RF, Agel J. Proximal tibial opening wedge osteotomy as the initial treatment for chronic posterolateral corner deficiency in the varus knee: a prospective clinical study. Am J Sports Med. 2007;35(11):1844-1850.[78]Malahias MA, Shahpari O, Kaseta MK. The clinical outcome of one-stage high tibial osteotomy and anterior cruciate ligament reconstruction. A current concept systematic and comprehensive review. Arch Bone Jt Surg. 2018;6(3):161-168.[79]Nagel A, Insall JN, Scuderi GR. Proximal tibial osteotomy. A subjective outcome study. J Bone Joint Surg Am. 1996;78(9): 1353-1358.[80]Odenbring S, Tjornstrand B, Egund N, et al. Function after tibial osteotomy for medial gonarthrosis below aged 50 years. Acta Orthop Scand. 1989;60(5):527-531.[81]Korovessis P, Katsoudas G, Salonikides P, et al. Medium- and long-term results of high tibial osteotomy for varusgonarthrosis in an agricultural population. Orthopedics. 1999;22(8):729-736.[82]Miller BS, Downie B, Mcdonough EB, et al. Complications after medial opening wedge high tibial osteotomy. Arthroscopy. 2009; 25(6):639-646.[83]Cotter EJ, Gowd AK, Bohl DD, et al. Medical comorbidities and functional dependent living are independent risk factors for short-term complications following osteotomy procedures about the knee. Cartilage. 2018:1947603518798889.[84]Niemeyer P, Stohr A, Kohne M, et al. Medial opening wedge high tibial osteotomy. Oper Orthop Traumatol. 2017;29(4):294-305. |
| [1] | Wang Jinjun, Deng Zengfa, Liu Kang, He Zhiyong, Yu Xinping, Liang Jianji, Li Chen, Guo Zhouyang. Hemostatic effect and safety of intravenous drip of tranexamic acid combined with topical application of cocktail containing tranexamic acid in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1356-1361. |
| [2] | Zhao Zhongyi, Li Yongzhen, Chen Feng, Ji Aiyu. Comparison of total knee arthroplasty and unicompartmental knee arthroplasty in treatment of traumatic osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 854-859. |
| [3] | Yuan Jun, Yang Jiafu. Hemostatic effect of topical tranexamic acid infiltration in cementless total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 873-877. |
| [4] | Cao Xuhan, Bai Zixing, Sun Chengyi, Yang Yanjun, Sun Weidong. Mechanism of “Ruxiang-Moyao” herbal pair in the treatment of knee osteoarthritis based on network pharmacology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 746-753. |
| [5] | Li Yonghua, Feng Qiang, Tan Renting, Huang Shifu, Qiu Jinlong, Yin Heng. Molecular mechanism of Eucommia ulmoides active ingredients treating synovitis of knee osteoarthritis: an analysis based on network pharmacology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 765-771. |
| [6] | Jie Ke, Deng Peng, Zeng Yirong. Application and comparison of four commonly used methods for patellar height measurement [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3875-3881. |
| [7] | Yang Wei, Chen Zehua, Yi Zhiyong, Huang Xudong, Han Qingmin, Zhang Ronghua. Effectiveness of intra-articular injection of hyaluronic acid versus placebo in the treatment of early and mid-stage knee osteoarthritis: a Meta-analysis based on randomized, double-blind, controlled, clinical trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(23): 3760-3766. |
| [8] | Mieralimu•Muertizha, Ainiwaerjiang•Damaola, Lin Haishan, Wang Li . Relationship between tibio-femoral mechanical axis deviation on coronal plane and early joint function recovery after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(21): 3300-3304. |
| [9] | Deng Zhibo, Li Zhi, Wu Yahong, Mu Yuan, Mu Yuexi, Yin Liangjun. Local infiltration anesthesia versus femoral nerve block for pain control and safety after total knee arthroplasty: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(21): 3401-3408. |
| [10] | Zuo Xiuqin, Yin Sasa, Xie Huimin, Jia Zishan, Zhang Lining. Applicability and specifications of platelet-rich plasma in musculoskeletal repair [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(20): 3239-3245. |
| [11] | Deng Bo, Hong Hainan, Fan Yongyong, Cai Guoping, Feng Xingbing, Hong Zhenghua. Efficacy and safety of tourniquet application in total knee arthroplasty and only at the time of cementing: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(18): 2908-2914. |
| [12] | Huang Chenyu, Tang Cheng, Wei Bo, Li Jiayi, Li Xuxiang, Zhang Huikang, Xu Yan, Yao Qingqiang, Wang Liming. Application of three-dimensional printing guide plate in total knee arthroplasty for patients with varus and valgus deformity [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(18): 2789-2793. |
| [13] | Li Shangzhi, Zheng Dezhi, Liu Jun. Early analgesia of cocktail therapy after total knee arthroplasty with enhanced recovery after surgery program [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(18): 2794-2798. |
| [14] | Liu Jinlei, Yin Li, Zhang Yi, Wang Haitao, Li Zhuangyan, Xia Peige, Qiao Renqiu. Effects of intravenous tranexamic acid combined with periarticular multipoint injection of tranexamic acid cocktail on blood loss and pain after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(18): 2833-2839. |
| [15] | Xu Hui, Kang Bingxin, Gao Chenxin, Zhao Chi, Xu Xirui, Sun Songtao, Xie Jun, Xiao Lianbo, Shi Qi. Effectiveness of Tuina in the treatment of pain after total knee arthroplasty in patients with knee osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(18): 2840-2845. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||