Chinese Journal of Tissue Engineering Research ›› 2019, Vol. 23 ›› Issue (16): 2516-2522.doi: 10.3969/j.issn.2095-4344.1148
Previous Articles Next Articles
Role of bone status in anterolateral portion of femoral head in the progression of osteonecrosis of the femoral head
Wei Qiushi1, 2, Fang Bin2, Chen Zhenqiu2, He Mincong3, Chen Xiaojun3, Yang Fan3, Zhang Qingwen1, 2, He Wei1, 2
- 1Hip Preserving Ward of Third Department of Orthopedics, 2Third Department of Orthopedics, the First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou 510407, Guangdong Province, China; 3Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China
-
Online:2019-06-08Published:2019-06-08 -
Contact:He Wei, Chief physician, Professor, Doctoral supervisor, Hip Preserving Ward of Third Department of Orthopedics, Third Department of Orthopedics, the First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou 510407, Guangdong Province, China -
About author:Wei Qiushi, MD, Hip Preserving Ward of Third Department of Orthopedics, Third Department of Orthopedics, the First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou 510407, Guangdong Province, China -
Supported by:国家自然科学基金(81573996),项目负责人:陈振秋|国家自然科学基金(81473697),项目负责人:何伟|广东省科技计划项目(2016A020226028)
CLC Number:
Cite this article
Wei Qiushi, Fang Bin, Chen Zhenqiu, He Mincong, Chen Xiaojun, Yang Fan, Zhang Qingwen, He Wei. Role of bone status in anterolateral portion of femoral head in the progression of osteonecrosis of the femoral head[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(16): 2516-2522.
share this article
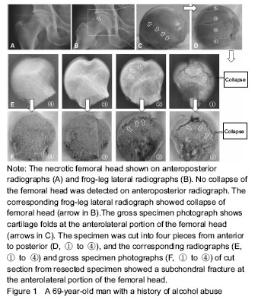
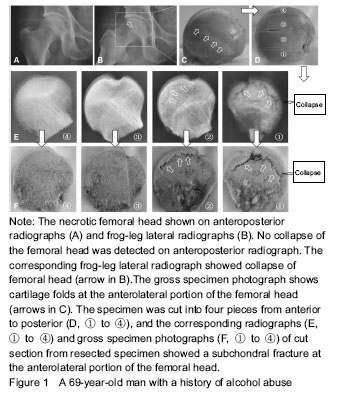
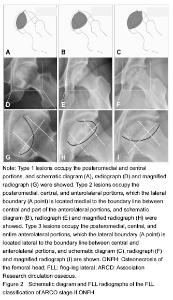
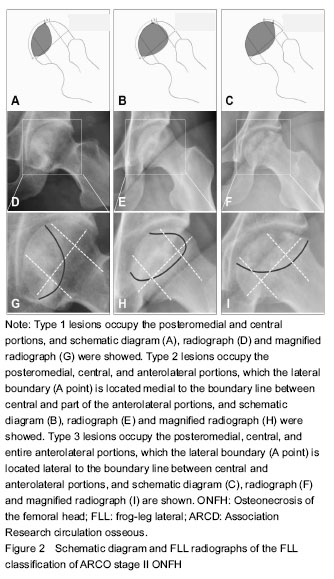
Imageology evaluation MRI and radiographs were analyzed in consensus by two experienced orthopedic surgeons in the diagnosis and treatment for ONFH. By screening T1-weighted MRI images, the diagnosis of ONFH was identified on the basis of previously published criteria, and the stage of the disease and subclassifications were defined according to the ARCO staging system[18]. The extent of the necrotic lesion in MRI was graded from A to C, representing less than 15% (type A), 15%-30% (type B) and more than 30% femoral head involvement (type C). Although the value of the China-Japan Friendship Hospital classification of ONFH based on 3 pillars of the femoral head is higher in predicting the collapse risk[19], the disadvantage is that the missed diagnosis rate of collapse is existent (Figure 1). Based on this, FLL classification was proposed according to the site of the necrotic lesion on the anterolateral portion of the femoral head. Accordingly, the location of the necrotic lesion within the femoral head was described as posteromedial and central portions (type 1), part of the anterolateral portion (type 2), and the entire anterolateral portion (type 3), which account for 25%, 50%, and 25% of the head width, respectively (Figure 2). The collapse rate and the time to collapse in different types were assessed."
"
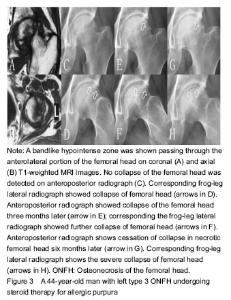
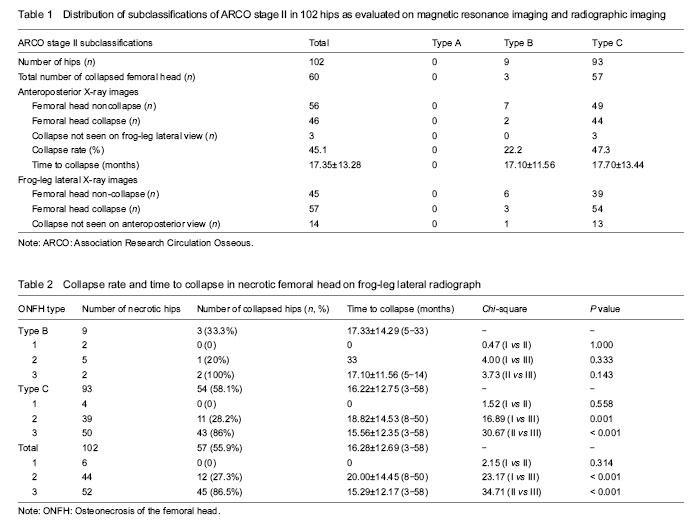
Statistical analysis The data were analyzed using SPSS version 13.0 (SPSS Inc., USA). A P value of less than 0.05 was considered statistically significant. Chi-square and Fisher’s exact tests were used for statistical analysis. RESULTS Clinical characteristics of the subjects Based on the inclusion and exclusion criteria, eight hips from five patients were excluded because of previous hip surgery in one patient, recent trauma to the femoral neck in two patients, and developmental dysplasia of the hip in two patients. Finally, 87 patients (102 hips) were enrolled into the study, including 65 men and 22 women with an average age of (44.38±12.74) years (19-73 years). Fifteen patients had bilateral sides and 72 patients had unilateral side of ONFH. All patients were followed for 3 to 58 months. MRI and radiographic imaging On MRI, the size of the necrotic lesion in the femoral head was graded as type A in zero hip, type B in 9 hips and type C in 93 hips (Table 1). On anteroposterior X-ray images, collapsed femoral heads were observed in 46 of 102 (45.1 %) hips, which were assigned to two hips in type B and 44 hips in type C (Table 1). On FLL images, collapsed femoral heads were found in 57 of 102 (55.9 %) hips, which were classified as type B (n=3) and type C (n=54), respectively. In the 60 collapsed-hips, the number of the collapsed femoral heads was viewed on FLL X-ray films and was significantly higher than that of on anteroposterior X-ray films (P < 0.01). However, the time to collapse were lower on FLL X-ray films than that of on anteroposterior X-ray films (16.28±12.69) months versus (17.35±13.28) months), although the P value was greater than 0.05 (Figure 3). Fourteen (23.3 %) hips were only seen on FLL X-ray films but not on anteroposterior X-ray images. The three collapsed-hips (5.0%) were only detected on anteroposterior images, but not on FLL images (Table 1)."

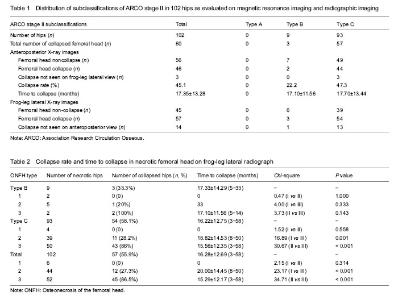
Collapse rate In all 102 hips with ARCO stage II ONFH, the collapse rate in type 3 ONFH was significantly higher than that of in type 2 ONFH (P < 0.001),and the time to collapse was markedly shortened. No femoral head collapse was found in six hips with type 1 ONFH. In nine hips with ARCO stage II type B ONFH, there was a higher collapse rate in type 3 ONFH compared with type 2 lesions (100% vs. 20%), but this was not statistically significant because of the low number of patients. In 93 hips with ARCO stage II type C ONFH, the collapse rate for type 3 ONFH was significantly higher than compared with both type 1 and type 2 (Table 2). "
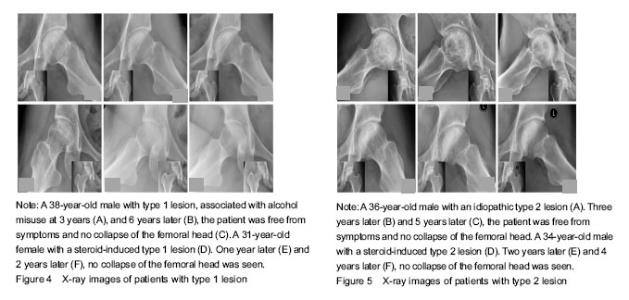
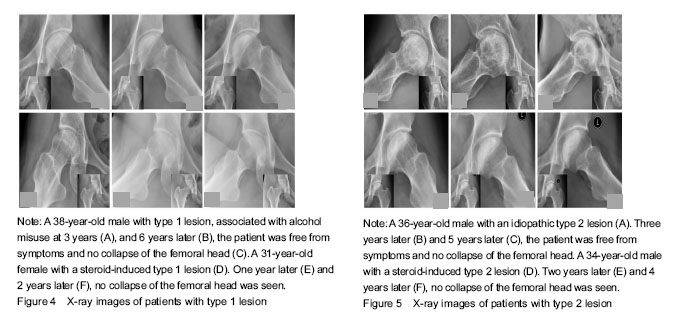
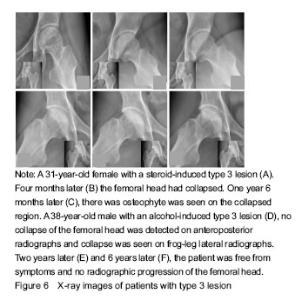
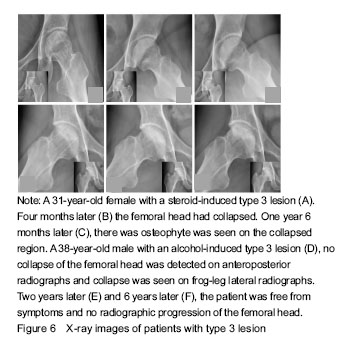
Only six hips were classified as type 1 at entry into the study. At the final examination, all these joints were still at ARCO stage II, the patients were free from symptoms (Figure 4). All 44 hips of type 2 were at stage II at the initial examination, 32 (72.7%) were still at stage II and 12 (27.3%) had collapsed of the femoral head during follow-up (Figure 5). The total incidence of collapse in all type 3 femoral heads, was 86.5% (45 to 52), 26 of these developed to stage III in three to 43 months (mean 21 months), and 19 of these having advanced to ARCO stage IV in three to 18 months (mean 11.5 months) after entry to the study (Figure 6)."
"
| [1] Kawai T, Shanjani Y, Fazeli S, et al. Customized, degradable, functionally graded scaffold for potential treatment of early stage osteonecrosis of the femoral head. J Orthop Res. 2018;36(3): 1002-1011. [2] Yue YB, Liu X, Wei BF. Attenuated serum adiponectin levels are associated with disease severity in patients with non-traumatic osteonecrosis of the femoral head. J Pain Res. 2017;10:2387-2393. [3] Wu W, He W, Wei QS, et al. Prognostic analysis of different morphology of the necrotic-viable interface in osteonecrosis of the femoral head. Int Orthop. 2018;42(1):133-139. [4] Houdek MT, Wyles CC, Collins MS, et al. Stem cells combined with platelet-rich plasma effectively treat corticosteroid-induced osteonecrosis of the hip: a prospective study. Clin Orthop Relat Res. 2018;476(2):388-397. [5] Mohanty SP, Singh KA, Kundangar R, et al. Management of non-traumatic avascular necrosis of the femoral head-a comparative analysis of the outcome of multiple small diameter drilling and core decompression with fibular grafting. Musculoskelet Surg. 2017; 101(1):59-66. [6] Chen L, Hong G, Fang B, et al. Predicting the collapse of the femoral head due to osteonecrosis: From basic methods to application prospects. J Orthop Translat. 2017;11:62-72. [7] Wang C, Meng H, Wang Y, et al. Analysis of early stage osteonecrosis of the human femoral head and the mechanism of femoral head collapse. Int J Biol Sci. 2018;14(2):156-164. [8] Daniel M, Herman S, Dolinar D, et al. Contact stress in hips with osteonecrosis of the femoral head. Clin Orthop Relat Res. 2006; 447:92-99. [9] Yu T, Xie L, Chu F. A sclerotic rim provides mechanical support for the femoral head in osteonecrosis. Orthopedics. 2015;38(5): e374-379. [10] Wen PF, Guo WS, Zhang QD, et al. Significance of lateral pillar in osteonecrosis of femoral head: a finite element analysis. Chin Med J (Engl). 2017;130(21):2569-2574. [11] Zhao D, Xie H, Xu Y, et al. Management of osteonecrosis of the femoral head with pedicled iliac bone flap transfer: A multicenter study of 2190 patients. Microsurgery. 2017;37(8):896-901. [12] Yu T, Xie L, Zhang Z, et al. Prediction of osteonecrosis collapse of the femoral head based on the proportion of the proximal sclerotic rim. Int Orthop. 2015;39(6):1045-50. [13] Sun W, Li ZR, Wang BL, et al. Relationship between preservation of the lateral pillar and collapse of the femoral head in patients with osteonecrosis. Orthopedics. 2014;37(1):e24-8. [14] Yang JW, Koo KH, Lee MC, et al. Mechanics of femoral head osteonecrosis using three-dimensional finite element method. Arch Orthop Trauma Surg. 2002;122:88-92. [15] Dolinar D, Antolic V, Herman S, et al. Influence of contact hip stress on the outcome of surgical treatment of hips affected by avascular necrosis. Arch Orthop Trauma Surg. 2003;123:509-513. [16] Takashima K, Sakai T, Hamada H, et al. Which classification system is most useful for classifying osteonecrosis of the femoral head? Clin Orthop Relat Res. 2018;476(6):1240-1249. [17] Hipfl C, Titz M, Chiari C, et al. Detecting cam-type deformities on plain radiographs: what is the optimal lateral view? Arch Orthop Trauma Surg. 2017;137(12):1699-1705. [18] Wu W, He W, Wei QS, et al. Prognostic analysis of different morphology of the necrotic-viable interface in osteonecrosis of the femoral head. Int Orthop. 2018;42(1):133-139. [19] Ma J, Guo W, Li Z, et al. Hip Osteonecrosis Is Associated with Increased Plasma IL-33 Level. Mediators Inflamm. 2017;2017: 1732638. [20] Kubo Y, Motomura G, Ikemura S, et al. The effect of the anterior boundary of necrotic lesion on the occurrence of collapse in osteonecrosis of the femoral head. Int Orthop. 2018;42(7): 1449-1455. [21] Baba T, Nozawa M, Homma Y, et al. Long-term results of rotational acetabular osteotomy for osteonecrosis with collapse of the femoral head in young patients. Arch Orthop Trauma Surg. 2017;137(7): 925-931. [22] Gao F, Han J, He Z, et al. Radiological analysis of cystic lesion in osteonecrosis of the femoral head. Int Orthop. 2018;42(7): 1615-1621. [23] Hu LB, Huang ZG, Wei HY, et al. Osteonecrosis of the femoral head: using CT, MRI and gross specimen to characterize the location, shape and size of the lesion. Br J Radiol. 2015;88(1046):20140508. [24] Kang JS, Moon KH, Kwon DG, et al. The natural history of asymptomatic osteonecrosis of the femoral head. Int Orthop. 2013;37(3):379-84. [25] Zhang Y, Zhang L, Sun R, et al. A new 3D printed titanium metal trabecular bone reconstruction system for early osteonecrosis of the femoral head. Medicine (Baltimore). 2018;97(26):e11088. [26] Hamada H, Takao M, Sakai T, et al. Subchondral fracture begins from the bone resorption area in osteonecrosis of the femoral head: a micro-computerised tomography study. Int Orthop. 2018;42(7): 1479-1484. [27] Koo KH, Kim R. Quantifying the extent of osteonecrosis of the femoral head. A new method using MRI. J Bone Joint Surg Br. 1995; 77:875-880. [28] Ha YC, Jung WH, Kim JR et al. Prediction of collapse in femoral head osteonecrosis: a modified Kerboul method with use of magnetic resonance images. J Bone Joint Surg Am. 2006;88:35-40. [29] Nishii T, Sugano N, Ohzono K, et al. Significance of lesion size and location in the prediction of collapse of osteonecrosis of the femoral head: a new three-dimensional quantification using magnetic resonance imaging. J Orthop Res. 2002;20:130-136. [30] Motomura G, Yamamoto T, Yamaguchi R, et al. Morphological analysis of collapsed regions in osteonecrosis of the femoral head. J Bone Joint Surg Br. 2011;93(2):184-187. [31] Hipfl C, Titz M, Chiari C, et al. Detecting cam-type deformities on plain radiographs: what is the optimal lateral view? Arch Orthop Trauma Surg. 2017;137(12):1699-1705. [32] Nagoya S, Nagao M, Takada J, et al. Predictive factors for vascularized iliac bone graft for nontraumatic osteonecrosis of the femoral head. J Orthop Sci. 2004;9(6):566-570. [33] Zhao D, Xie H, Xu Y, et al. Management of osteonecrosis of the femoral head with pedicled iliac bone flap transfer: A multicenter study of 2190 patients. Microsurgery. 2017;37(8):896-901. [34] Steinberg ME, Oh SC, Khoury V, et al. Lesion size measurement in femoral head necrosis. Int Orthop. 2018;42(7):1585-1591. |
| [1] | Min Youjiang, Yao Haihua, Sun Jie, Zhou Xuan, Yu Hang, Sun Qianpu, Hong Ensi. Effect of “three-tong acupuncture” on brain function of patients with spinal cord injury based on magnetic resonance technology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(在线): 1-8. |
| [2] | He Li, Tian Wei, Xu Song, Zhao Xiaoyu, Miao Jun, Jia Jian. Factors influencing the efficacy of lumbopelvic internal fixation in the treatment of traumatic spinopelvic dissociation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 884-889. |
| [3] | Liu Lihua, Sun Wei, Wang Yunting, Gao Fuqiang, Cheng Liming, Li Zirong, Wang Jiangning. Type L1 steroid-induced osteonecrosis of the femoral head through femoral head and neck junction decompression by fenestration: a single-center prospective clinical study [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 906-911. |
| [4] | Liu Zhao, Xu Xilin, Shen Yiwei, Zhang Xiaofeng, Lü Hang, Zhao Jun, Wang Zhengchun, Liu Xuzhuo, Wang Haitao. Guiding role and prospect of staging and classification combined collapse prediction method for osteonecrosis of femoral head [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 929-934. |
| [5] | Zheng Xiaolong, He Xiaoming, Gong Shuidi, Pang Fengxiang, Yang Fan, He Wei, Liu Shaojun, Wei Qiushi. Bone turnover characteristics in patients with alcohol-induced osteonecrosis of the femoral head [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 657-661. |
| [6] | Yi Meizhi, Luo Guanghua, Xiao Yawen, Hu Rong, Chen Xiaolong, Zhao Heng. MRI findings of anatomical variations of the talus [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3888-3893. |
| [7] | Xie Jingshu, Zhang Xianglin, Liu Jinlei, Wen Jing. Application of High Resolution reconstruction algorithm in precision CT scans of the middle and inner ears [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(23): 3614-3618. |
| [8] | Liu Ningning, Wang Bing. Feasibility of repairing the fixed end non-bolt abutment crown of MK1 precision attachment with porcelain-fused-to-metal crown [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3517-3521. |
| [9] | Yu Yinghao, Zhao Jijun, Liu Dongcheng, Chen Yuhao, Feng Dehong. Clinical significance of preoperative planning assisted unicompartmental knee arthroplasty with digital imaging system for fixed-bearing prosthesis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(21): 3324-3331. |
| [10] | Liu Xing, Wei Xiaohan, Deng Jie, Li Zhongming . Preparing a blunt contusion model of rabbit skeletal muscle under different blow strengths [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(2): 196-200. |
| [11] | Du Xueting, Yang Yang, Huang Wenhua, Chen Wubiao. Clinical application and breakthrough of three-dimensional printing based on medical imaging technology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(18): 2887-2894. |
| [12] | Zhou Yi, Chen Yueping, Zhang Xiaoyun, Lai Yu, Liao Jianzhao, Li Shibin. An exploration on mechanism of Shengyu Decoction in treating osteonecrosis of the femoral head based on network pharmacology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(17): 2687-2696. |
| [13] | Xin Pengfei, Ke Mengnan, Zhang Haitao, Urishana, Li Ziqi, Zhuang Zhikun, Wei Qiushi, He Wei. Common mechanism of Chinese herbs for promoting blood circulation and removing blood stasis in the treatment of osteonecrosis of the femoral head: an analysis based on network pharmacology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(17): 2727-2733. |
| [14] | Su Jingyang, Zhang Yaojie, Cao Bin, Hao Xuewei, Li Xiao, Han Yongtai. Analysis of collapse and related factors in the treatment of ARCO I-II non-traumatic necrosis of femoral head with porous tantalum rod [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(15): 2400-2404. |
| [15] | Chen Xiaolong, Zhao Heng, Hu Rong, Luo Guanghua, Liu Jincai . Correlation of infrapatellar fat pad edema with trochlear and patellofemoral joint morphology: MRI evaluation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(15): 2410-2415. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||