Chinese Journal of Tissue Engineering Research ›› 2021, Vol. 25 ›› Issue (24): 3790-3795.doi: 10.12307/2021.081
Previous Articles Next Articles
Computer-assisted navigation combined with minimally invasive transforaminal lumbar interbody fusion for lumbar spondylolisthesis
Qian Xuankun, Huang Hefei, Wu Chengcong, Liu Keting, Ou Hua, Zhang Jinpeng, Ren Jing, Wan Jianshan
- Department of Spine Surgery, No.1 People’s Hospital of Qujing, Qujing 655000, Yunnan Province, China
-
Received:2020-09-25Revised:2020-09-28Accepted:2020-11-09Online:2021-08-28Published:2021-03-05 -
Contact:Ren Jing, Associate chief physician, Department of Spine Surgery, No.1 People’s Hospital of Qujing, Qujing 655000, Yunnan Province, China Wan Jianshan, Chief physician, Department of Spine Surgery, No.1 People’s Hospital of Qujing, Qujing 655000, Yunnan Province, China -
About author:Qian Xuankun, Master, Attending physician, Department of Spine Surgery, No.1 People’s Hospital of Qujing, Qujing 655000, Yunnan Province, China -
Supported by:the Scientific Research Foundation Project of Yunnan Provincial Department of Education, No. 2016ZDX074 (to WCC)
CLC Number:
Cite this article
Qian Xuankun, Huang Hefei, Wu Chengcong, Liu Keting, Ou Hua, Zhang Jinpeng, Ren Jing, Wan Jianshan. Computer-assisted navigation combined with minimally invasive transforaminal lumbar interbody fusion for lumbar spondylolisthesis[J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3790-3795.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
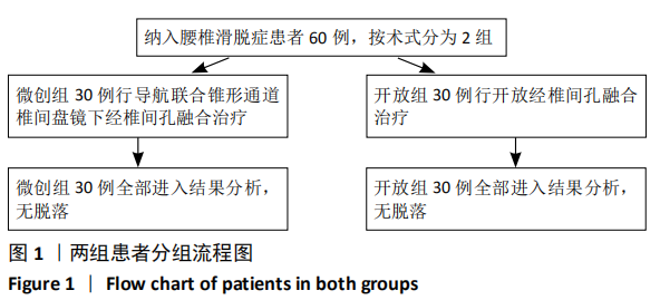
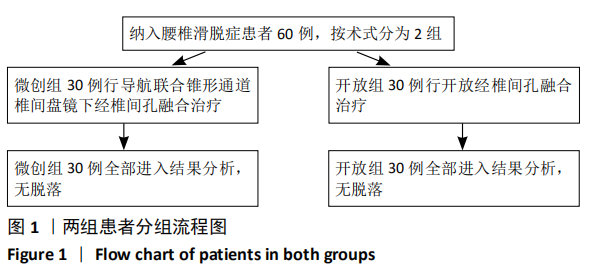
2.1 参与者数量分析 纳入腰椎滑脱症患者60例,随访期间影像资料完整,全部进入结果分析,无脱落。两组患者均顺利完成手术,术中、术后均无马尾及神经根损伤发生,无椎间隙感染。术后所有患者均获得12-40个月随访,随访过程中未发现内植物断裂、松动。 2.2 试验流程图 见图1。"
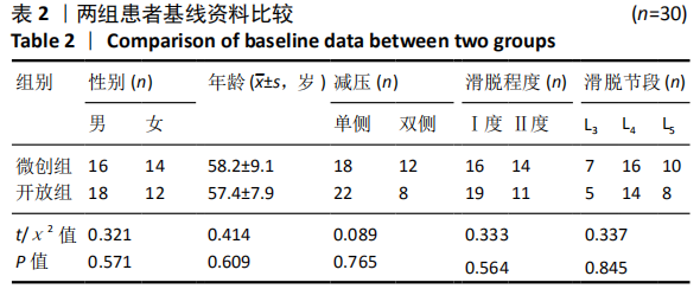
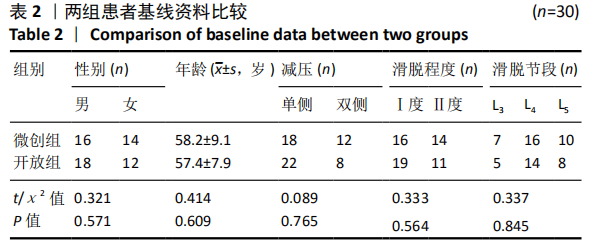
2.3 一般情况比较 两组患者性别、年龄、病程、滑脱节段分布、单、双侧症状的构成等一般资料比较,差异均无显著性意义(P > 0.05),见表2。"
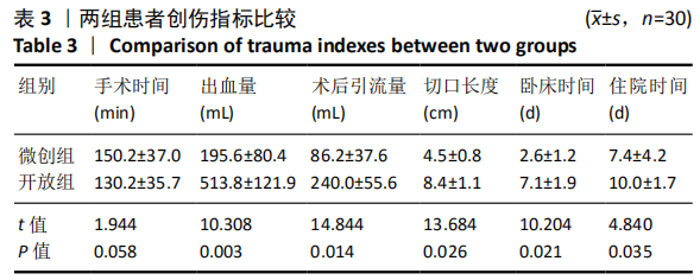
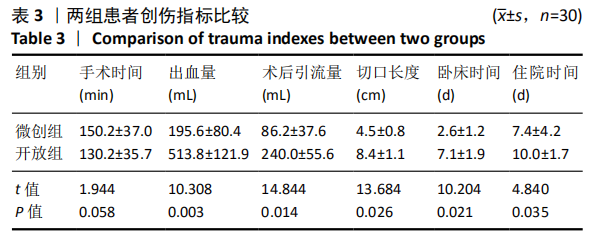
2.4 手术相关指标比较 微创组平均手术时间稍长于开放组,但差异无显著性意义(P > 0.05)。微创组出血量、术后引流量明显少于开放组,差异有显著性意义(P < 0.05);切口长度、术后卧床时间、住院时间微创组明显少于开放组,差异有显著性意义(P < 0.05),详见表3。"
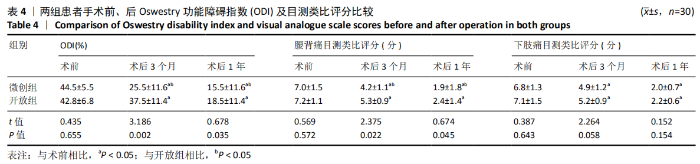
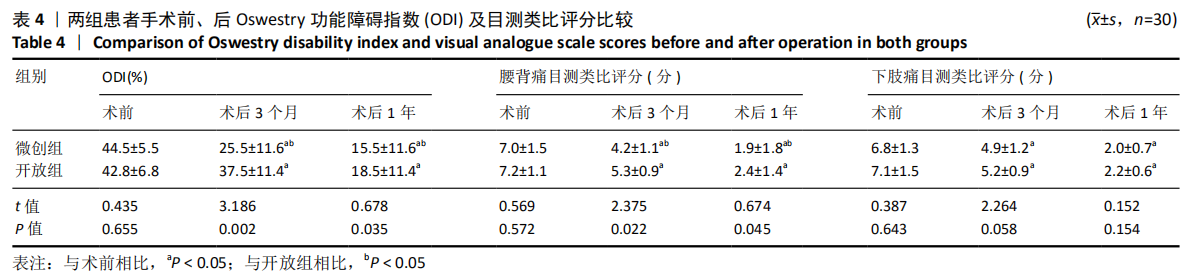
2.5 术后疗效指标比较 两组术前ODI、目测类比评分比较差异无显著性意义。术后ODI和腰腿痛目测类比评分与术前相比均明显降低,差异有显著性意义(P < 0.05);微创组术后随访ODI、腰背痛目测类比评分均明显低于开放组,差异有显著性意义(P < 0.05);术后下肢目测类比评分两组相比差异无显著性意义(P > 0.05),详见表4。"
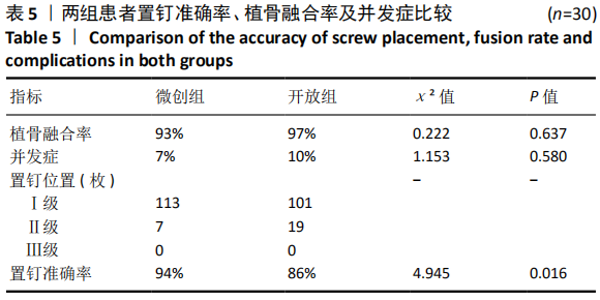
2.6 植骨融合率、置钉准确率比较 术后1年随访时微创组有2例、开放组有1例未达到骨性融合,末次随访均骨性融合,植骨融合率两组差异无显著性意义(P > 0.05)。椎弓根钉位置Ⅰ级微创组有113枚,开放组101枚,两组均无Ⅲ级椎弓根钉,置钉准确率微创组高于开放组,差异有显著性意义(P < 0.05),见表5。"

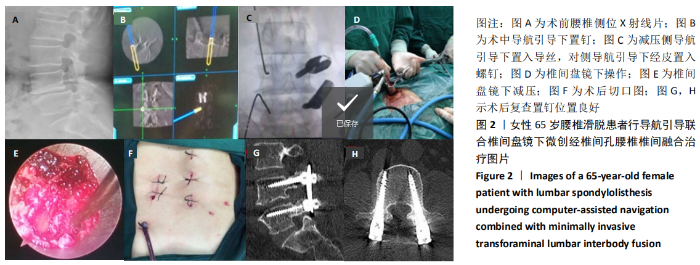
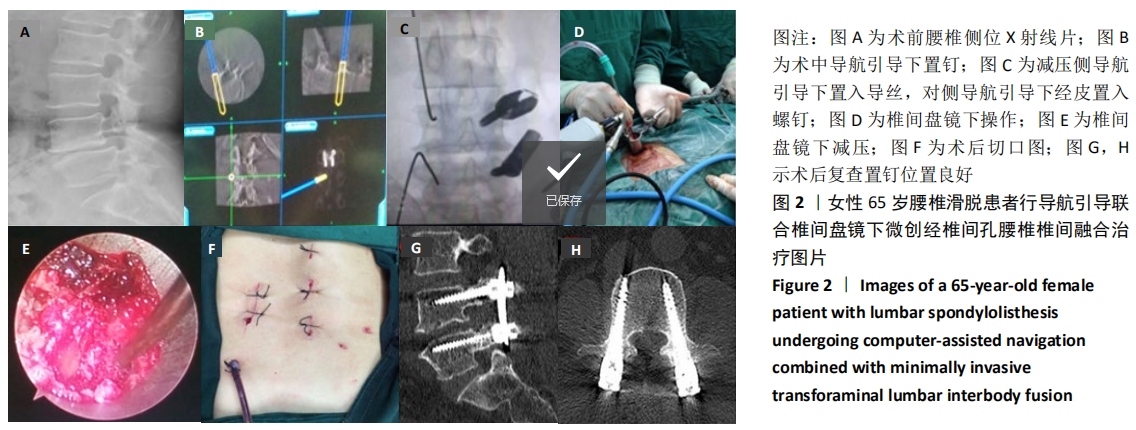
2.7 不良反应与内植物组织相容性 开放组有2例出现浅表皮肤感染、延迟愈合,经积极换药后切口愈合良好;微创组和开放组分别有2例、1例术中因严重退变,局部粘连术中出现硬脊膜破裂,两组并发症相比差异无显著性意义(P > 0.05)。随访结果显示植入物组织相容性良好,未出现植入物过敏、免疫排斥等不良反应。 2.8 典型病例 女性患者,65岁,腰痛4年,加重伴下肢麻木、跛行6个月,诊断为腰椎滑脱,入院后行导航引导联合椎间盘镜下MIS-TLIF术,术后患者腰腿痛症状明显缓解,复查影像资料见内固定物位置满意,见图2。"
| [1] BOZKUS H, DICKMAN CA. Transvertebral interbody cage and pedicle screw fixation for high-grade spondylolisthesis: case report. J Neurosurg. 2004;100(1):62-65. [2] HARMS J, ROLINGER H. A one-stager procedure in operative treatment of spondylolistheses: dorsal traction-reposition and anterior fusion (author’s transl). Z Orthop Ihre Grenzgeb. 1982;120(3):343-347. [3] 周长嵩, 黄聿峰, 彭云娟. 老年单节段腰椎退变性疾病的TLIF与PLIF治疗效果比较[J]. 中国初级卫生保健,2016,30(10):94-95. [4] 李一鹏, 段晓丰, 田玉良, 等. TLIF与PLIF治疗上腰段退行性Ⅰ度滑脱并椎管狭窄的疗效比较[J]. 现代中西医结合杂志,2016,25(13):1410-1413. [5] 董献成, 王庆伟, 荆鑫, 等. 应用PLIF及TLIF治疗腰椎退变性疾病的比较研究[J]. 颈腰痛杂志,2016,37(6):507-510. [6] FOLEY KT, LEFKOWITZ MA. Advances in minimally invasive spine surgery. Clin Neurosurg. 2001;49:499-517. [7] 张小会. 应用Mast-Quadrant可扩张通道系统显微镜下手术治疗腰椎间盘突出症的临床研究[J]. 世界最新医学信息文摘,2015,15(3):68-69. [8] KIM CH, EASLEY K, LEE JS, et al. Comparison of Minimally Invasive Versus Open Transforaminal Interbody Lumbar Fusion. Global Spine J. 2020;10(2):143S-150S. [9] GOLDSTEIN CL, PHILLIPS FM, RAMPERSAUD YR. Comparative Effectiveness and Economic Evaluations of Open Versus Minimally Invasive Posterior or Transforaminal Lumbar Interbody Fusion. Spine. 2016;41(8):S74-S89. [10] 王建, 周跃, 张正丰, 等. 微创经椎间孔腰椎体间融合术治疗腰椎滑脱症的临床研究[J]. 中华外科杂志,2011,49(12):1076-1080. [11] 曾顺福, 王建, 陆炎, 等. 单节段微创经椎间孔腰椎椎体间融合内固定治疗腰椎滑脱症的效果[J]. 中国脊柱脊髓杂志,2011,21(5):399-403. [12] 陈晓明, 肖增明, 宗少晖, 等. 计算机导航引导下脊柱后路椎弓根螺钉置入内固定: 准确性及安全性[J]. 中国组织工程研究,2015,19(13):2119-2124. [13] 殷铁林, 王祥善. 三维CT导航下微创经椎间孔腰椎椎体间融合术治疗单节段腰椎退行性疾病 [J]. 颈腰痛杂志,2019,40(6):860-861. [14] 桂召柳, 吴天亮, 林志祥, 等. 三维CT导航辅助下经椎间孔椎体间融合术治疗腰椎间盘突出症的临床疗效及安全性[J]. 山东医药,2017,57(17):85-87. [15] SUI RD, WANG CG, ZHANG JC, et al. Clinical Application of CT Navigation in treatment of Lumbar Spondylolisthesis with Minimally Invasive Surgery - Transforaminal Lumbar Interbody Fusion. Pak J Med Sci. 2020;36(5):935-940. [16] BARSA P, SUCHOMEL P. Portable CT scanner-based navigation in lumbar pedicle screw insertion. Eur Spine J. 2013;22(6):1446-1450. [17] YOUKILIS AS, QUINT DJ, MCGILLICUDDY JE, et al. Stereotactic navigation for placement of pedicle screws in the thoracic spine. Neurosurgery. 2001;48(4): 771-779. [18] FOLEY KT, SIMON DA, RAMPERSAUD YR. Virtual fluoroscopy: computer-assisted fluoroscopic navigation. Spine. 2001;26(4):347-351. [19] SUK S, LEE C, KIM W, et al. Adding posterior lumbar interbody fusion to pedicle screw fixation and posterolateral fusion after decompression in spondylolytic spondylolisthesis. Spine. 1997;22(2):210-219. [20] TALIA AJ, WONG ML, LAU HC, et al. Comparison of the different surgical approaches for lumbar interbody fusion. J Clin Neurosci. 2015;22(2):243-251. [21] YANG Y, YAN X, LI W, et al. Long‐Term Clinical Outcomes and Pain Assessment after Posterior Lumbar Interbody Fusion for Recurrent Lumbar Disc Herniation. Orthop Surg. 2020;12(3):907-916. [22] HARMS JG, JESZENSZKY D. The unilateral transforaminal approach for posterior lumbar interbody fusion. Orthop Traumatol. 1998;6(2):88-99. [23] ZENG ZL, JIA L, YU Y, et al. Clinical outcomes of single-level lumbar spondylolisthesis by minimally invasive transforaminal lumbar interbody fusion with bilateral tubular channels. Zhonghua Wai Ke Za Zhi. 2017;55(4):279-284. [24] KIM JY, PARK JY, KIM KH. Minimally Invasive Transforaminal Lumbar Interbody Fusion for Spondylolisthesis: Comparison Between Isthmic and Degenerative Spondylolisthesis. World Neurosurg. 2015;84(5):1284-1293. [25] FOLEY KT, HOLLY LT, SCHWENDER JD. Minimally invasive lumbar fusion. Spine (Phila Pa 1976). 2003;28(15 Suppl):S26-35. [26] SULAIMAN WA, SINGH M. Minimally invasive versus open transforaminal lumbar interbody fusion for degenerative spondylolisthesis grades 1-2: patient-reported clinical outcomes and cost-utility analysis. Ochsner J. 2014;14(1):32-37. [27] KULKARNI A, BOHRA H, DHRUV A, et al. Minimal invasive transforaminal lumbar interbody fusion versus open transforaminal lumbar interbody fusion. Indian J Orthop. 2016;50(5):464-472. [28] VAZAN M, GEMPT J, MEYER B, et al. Minimally invasive transforaminal lumbar interbody fusion versus open transforaminal lumbar interbody fusion: a technical description and review of the literature. Acta Neurochirurgica. 2017;159(6): 1137-1146. [29] 邹澍, 王建, 潘文琦, 等. 微创与开放经椎间孔腰椎椎间融合术组织创伤相关血清指标的比较研究[J]. 中国修复重建外科杂志,2013,27(8):960-964. [30] YOO J, MIN S, YOON S, et al. Paraspinal muscle changes of unilateral multilevel minimally invasive transforaminal interbody fusion. J Orthop Surg Res. 2014;9(1):130. [31] 汤红伟, 吴文坚, 张兴凯, 等. 微创与开放性经椎间孔腰椎椎间融合术创伤定量对比研究[J]. 国际骨科学杂志,2016,37(5):326-330. [32] 李明, 许红云, 鞠亮, 等. 微创与开放经椎间孔椎间融合术治疗腰椎不稳的疗效比较[J]. 临床骨科杂志,2016,19(5):534-537. [33] 吴茂成, 李康杰, 南军, 等. 计算机导航辅助下经wiltse入路在老年胸腰椎骨折治疗中的应用[J]. 中国老年学杂志,2015,35(16):4614-4616. [34] 俞伟杨, 何登伟, 刘飞俊. 微创与开放经椎间孔椎间融合术治疗单间隙腰椎退行性疾病及中长期临床疗效比较[J]. 浙江创伤外科,2015,20(2):201-205. [35] YILAR S. Comparison of the accuracy of cannulated pedicle screw versus conventional pedicle screw in the treatment of adolescent idiopathic scoliosis: A randomized retrospective study. Medicine. 2019;98(10):e14811. [36] YONG F, PENG DJ, JUN LJ, et al. Accuracy of pedicle screw placement comparing robot-assisted technology and the free-hand with fluoroscopy-guided method in spine surgery: An updated meta-analysis. Medicine. 2018;97(22):e10970. [37] LUTHER N, IORGULESCU JB, GEANNETTE C, et al. Comparison of navigated versus non-navigated pedicle screw placement in 260 patients and 1434 screws: screw accuracy, screw size, and the complexity of surgery. J Spinal Disord Tech. 2015;28(5):298-303. [38] 丁文彬, 郑召民, 王建儒, 等. 微创与开放经椎间孔椎体间融合术治疗单节段腰椎病变的Meta分析[J]. 中国脊柱脊髓杂志,2015,25(1):45-53. [39] 闫兵山, 徐宝山, 刘越, 等. 微创与开放经椎间孔椎体间融合治疗腰椎滑脱的Meta分析[J]. 中国组织工程研究,2017,21(15):2453-2460. |
| [1] | Yao Rubin, Wang Shiyong, Yang Kaishun. Minimally invasive transforaminal lumbar interbody fusion for treatment of single-segment lumbar spinal stenosis improves lumbar-pelvic balance [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1387-1392. |
| [2] | Wang Haiying, Lü Bing, Li Hui, Wang Shunyi. Posterior lumbar interbody fusion for degenerative lumbar spondylolisthesis: prediction of functional prognosis of patients based on spinopelvic parameters [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1393-1397. |
| [3] | Zhang Lei, Ma Li, Fu Shijie, Zhou Xin, Yu Lin, Guo Xiaoguang. Arthroscopic treatment of greater tuberosity avulsion fractures with anterior shoulder dislocation using the double-row suture anchor technique [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 895-900. |
| [4] | Liang Yan, Zhao Yongfei, Zhu Zhenqi, Liu Haiying, Mao Keya. Minimally invasive transforaminal lumbar interbody fusion in the treatment of sciatic scoliosis caused by lumbar disc herniation: a 2-year follow-up of coronal and sagittal balance [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 409-413. |
| [5] | Meng Lingjie, Qian Hui, Sheng Xiaolei, Lu Jianfeng, Huang Jianping, Qi Liangang, Liu Zongbao. Application of three-dimensional printing technology combined with bone cement in minimally invasive treatment of the collapsed Sanders III type of calcaneal fractures [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3784-3789. |
| [6] | Liu Jinyu, Ding Yiwei, Lu Zhengcao, Gao Tianjun, Cui Hongpeng, Li Wen, Du Wei, Ding Yu. Finite element biomechanical study of full endoscopic fenestration decompression for cervical spondylotic myelopathy [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3850-3854. |
| [7] | Zou Shouping, Lu Daoyun, Ye Li. Minimally invasive percutaneous pedicle screw technique for thoracolumbar fractures: biomechanical changes of the spine during 6-month follow-up [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3865-3869. |
| [8] | Wang Ziao, Song Wenhui, Liu Changwen . Short-segment fixation of thoracolumbar burst fractures: method modification and strategies to reduce failure [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3902-3907. |
| [9] | Zheng Kai, Li Rongqun, Sun Houyi, Zhang Weicheng, Li Ning, Zhou Jun, Zhu Feng, Wang Yijun, Xu Yaozeng. Computer-navigated versus conventional one-stage bilateral total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(21): 3305-3312. |
| [10] | Wu Yanyu, Zhang Chunlin, Shao Chenglong, Yan Xu, Liu Xiaokang, Wang Yongkui, Li Dongzhe. Quantitative measurement of resorption of cervical herniated disc after cervical microendoscopic laminoplasty by two-dimensional distance method and three-dimensional volume method [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(21): 3390-3394. |
| [11] |
Xie Fei, Li Yanle, Lin Xinxiao, Hu Haiwei, Sang Zhicheng, Sun Yongsheng, Jiang Kewei, Cheng Ying, Wen Guannan, Wen Jianmin, Sun Weidong.
Mechanism underlying mechanical stress regulating fibroblasts-derived
exosomes at the osteotomized end following hallux valgus correction |
| [12] | Wei Yangyang, Chen Jiacheng, Sun Jun, Wang Qiuan, Yuan Feng. Comparison of lumbar-pelvic sagittal parameters after single-level and double-level posterior lumbar interbody fusion [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(33): 5300-5306. |
| [13] | Chen Keyi, Yang Shun, Cheng Yabo, Xiang Wang, Zhang Jing, Chi Haotian. Wrist arthroscopy combined with 2.7 mm titanium osteotomy plate fixation in treatment of ulnar impaction syndrome [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(33): 5326-5331. |
| [14] | Zhang Yuda, Wang Changyao, Wang Xiangyu. Imaging evaluation after minimally invasive total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(33): 5379-5384. |
| [15] | Zhan Fangbiao, Xie Lizhong, Zou Xinsen, Long Jie, Cheng Jun, Zhang Xianwei. Efficacy and safety of percutaneous kyphoplasty versus posterior short-segment fixation with vertebra augmentation for Kummell’s disease: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(33): 5397-5404. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||