Chinese Journal of Tissue Engineering Research ›› 2020, Vol. 24 ›› Issue (33): 5379-5384.doi: 10.3969/j.issn.2095-4344.2337
Previous Articles Next Articles
Imaging evaluation after minimally invasive total hip arthroplasty
Zhang Yuda1, Wang Changyao2, Wang Xiangyu1
1Medical College of Qingdao University, Qingdao 266071, Shandong Province, China; 2Affiliated Hospital of Qingdao University, Qingdao 266071, Shandong Province, China
-
Received:2020-02-12Revised:2020-02-22Accepted:2020-04-03Online:2020-11-28Published:2020-10-13 -
Contact:Wang Changyao, MD, Associate chief physician, Affiliated Hospital of Qingdao University, Qingdao 266071, Shandong Province, China -
About author:Zhang Yuda, Master candidate, Medical College of Qingdao University, Qingdao 266071, Shandong Province, China -
Supported by:the National Natural Science Foundation of China, No. 81772329
CLC Number:
Cite this article
Zhang Yuda, Wang Changyao, Wang Xiangyu. Imaging evaluation after minimally invasive total hip arthroplasty[J]. Chinese Journal of Tissue Engineering Research, 2020, 24(33): 5379-5384.
share this article
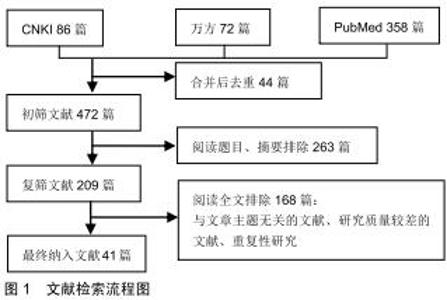
1.4 质量评估 通过上述计算机检索与手工检索,共检索到360篇参考文献。按入选标准进行人工筛选,排除与主题相关性差及重复、陈旧的文献,最终纳入41篇文献,见图1。纳入研究的文献包括研究原著、综述、临床试验、述论等。 "
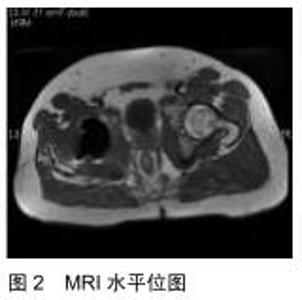
2.1.3 MRI 在暴露股骨颈及髋臼时,不可避免的要分离或切开髋周肌群,造成肌肉损伤。MRI是评估微创全髋关节置换术中肌肉损伤的重要影像学检查手段[10]。MRI结合了优越的组织对比度和检测骨髓水肿的能力,为软组织和骨性病理提供了准确和灵敏的评估,它可以确定全髋关节术后患者疼痛的肌肉原因,直观、准确地显示手术相关创伤的效果[11]。MüLLER等[12]针对接受直接外侧或微创全髋关节置换患者,在其术后3-12个月使用MRI评估了臀中肌的脂肪变性,结论显示使用微创方法可明显减少肌肉创伤,在老年人和超重患者中尤为明显。除软组织显像以外,MRI对人工假体周围骨组织显像也有独特价值,假体周围骨折MRI的诊断特点是急性期皮质、松质骨呈线性低信号改变,伴有周围骨髓水肿,而骨应力反应显示局限性水肿,其特征是髓腔、皮质、骨膜和邻近软组织高信号[13]。骨溶解患者的MR成像显示局灶性骨吸收区域,最常见的是等信号且边缘清晰的硬化灶。非特异性滑膜炎是指MRI显示单纯性关节液呈均匀的液体信号强度,滑膜厚度和信号强度正常或轻度增加的情况[14],这一直接的影像学证据在评估手术入路和置入技术的优劣性方面有很大的好处。肌腱缺损和脂肪萎缩是与臀中肌、臀小肌、外展肌、外旋肌群等肌肉功能直接相关的结构变化,而MRI能够将活体形态学与个体功能结果关联起来[15]。因此MRI已经成为评价肌肉,特别是肌肉形态学改变的金标准[4]。此文筛选并总结3篇文献共197例患者,从全髋关节置换术后发生骨溶解、无菌性松动、假体周围感染3方面分析与评价X射线片、CT、MRI三者的诊断阳性率。经分析数据发现,X射线片诊断骨溶解、无菌性松动、感染的阳性率分别为78.4%,83.7%,35.0%;CT诊断阳性率为88.2%,88.3%,40.0%;MRI诊断阳性率为84.3%,95.3%,98.3%。因此在诊断感染方面,MRI阳性率明显大于X射线和CT,见图2,3。但在诊断无菌性松动和骨溶解方面,3种检查无明显差异[16]。这一现象与临床相符,也普遍被临床医师所接受。"
2.1.3 MRI 在暴露股骨颈及髋臼时,不可避免的要分离或切开髋周肌群,造成肌肉损伤。MRI是评估微创全髋关节置换术中肌肉损伤的重要影像学检查手段[10]。MRI结合了优越的组织对比度和检测骨髓水肿的能力,为软组织和骨性病理提供了准确和灵敏的评估,它可以确定全髋关节术后患者疼痛的肌肉原因,直观、准确地显示手术相关创伤的效果[11]。MüLLER等[12]针对接受直接外侧或微创全髋关节置换患者,在其术后3-12个月使用MRI评估了臀中肌的脂肪变性,结论显示使用微创方法可明显减少肌肉创伤,在老年人和超重患者中尤为明显。除软组织显像以外,MRI对人工假体周围骨组织显像也有独特价值,假体周围骨折MRI的诊断特点是急性期皮质、松质骨呈线性低信号改变,伴有周围骨髓水肿,而骨应力反应显示局限性水肿,其特征是髓腔、皮质、骨膜和邻近软组织高信号[13]。骨溶解患者的MR成像显示局灶性骨吸收区域,最常见的是等信号且边缘清晰的硬化灶。非特异性滑膜炎是指MRI显示单纯性关节液呈均匀的液体信号强度,滑膜厚度和信号强度正常或轻度增加的情况[14],这一直接的影像学证据在评估手术入路和置入技术的优劣性方面有很大的好处。肌腱缺损和脂肪萎缩是与臀中肌、臀小肌、外展肌、外旋肌群等肌肉功能直接相关的结构变化,而MRI能够将活体形态学与个体功能结果关联起来[15]。因此MRI已经成为评价肌肉,特别是肌肉形态学改变的金标准[4]。此文筛选并总结3篇文献共197例患者,从全髋关节置换术后发生骨溶解、无菌性松动、假体周围感染3方面分析与评价X射线片、CT、MRI三者的诊断阳性率。经分析数据发现,X射线片诊断骨溶解、无菌性松动、感染的阳性率分别为78.4%,83.7%,35.0%;CT诊断阳性率为88.2%,88.3%,40.0%;MRI诊断阳性率为84.3%,95.3%,98.3%。因此在诊断感染方面,MRI阳性率明显大于X射线和CT,见图2,3。但在诊断无菌性松动和骨溶解方面,3种检查无明显差异[16]。这一现象与临床相符,也普遍被临床医师所接受。"
|
[1] WANG T, SHAO L, XU W, et al. Surgical injury and repair of hip external rotators in THA via posterior approach: a three-dimensional MRI-evident quantitative prospective study. BMC Musculoskelet Disord. 2019; 20(1):22.
[2] WANG T, SHAO L, XU W, et al. Comparison of morphological changes of gluteus medius and abductor strength for total hip arthroplasty via posterior and modified direct lateral approaches. Int Orthop. 2019;43(11):2467-2475.
[3] 黄行健,周一新,杨德金,等.全髋关节置换术后晚期并发症的影像学评估[J].骨科临床与研究杂志,2017,2(1):57-63.
[4] AGTEN CA, SUTTER R, DORA C, et al. MR imaging of soft tissue alterations after total hip arthroplasty: comparison of classic surgical approaches. Eur Radiol. 2017;27(3):1312-1321.
[5] VAN DEN WYNGAERT T, PAYCHA F, STROBEL K, et al. SPECT/CT in Postoperative Painful Hip Arthroplasty. Semin Nucl Med.2018;48(5):425-438.
[6] ALEXANDROV T, AHLMANN ER, MENENDEZ LR. Early clinical and radiographic results of minimally invasive anterior approach hip arthroplasty. Adv Orthop. 2014;2014: 954208.
[7] PENENBERG BL, SAMAGH SP, RAJAEE SS, et al. Digital Radiography in Total Hip Arthroplasty: Technique and Radiographic Results. J Bone Joint Surg Am. 2018;100(3):226-235.
[8] DOBRINDT O, AMTHAUER H, KRUEGER A, et al. Hybrid SPECT/CT for the assessment of a painful hip after uncemented total hip arthroplasty. BMC Med Imaging. 2015;15:18.
[9] TOKUNAGA K, OKAMOTO M, WATANABE K. Implant Orientation Measurement After THA Using the EOS X-Ray Image Acquisition System. Adv Exp Med Biol. 2018;1093:335-343.
[10] YUE B, TANG T. The use of nuclear imaging for the diagnosis of periprosthetic infection after knee and hip arthroplasties. Nucl Med Commun. 2015;36(4):305-311.
[11] BREMER AK, KALBERER FC, PFIRRMANN WA, et al. Soft-tissue changes in hip abductor muscles and tendons after total hip replacement: comparison between the direct anterior and the transgluteal approaches. J Bone Joint Surg Br. 2011;93(7): 886-889.
[12] MÜLLER M, TOHTZ S, DEWEY M, et al. Muscle trauma in primary total hip arthroplasty depending on age, BMI, and surgical approach: minimally invasive anterolateral versus modified direct lateral approach. Orthopade. 2011;40(3):217-223.
[13] VASILAKIS I, SOLOMOU E, VITSAS V, et al. Correlative analysis of MRI-evident abductor hip muscle degeneration and power after minimally invasive versus conventional unilateral cementless THA. Orthopedics. 2012;35(12):e1684-1691.
[14] FRITZ J, LURIE B, MILLER TT, et al. MR imaging of hip arthroplasty implants. Radiographics. 2014;34(4):E106-132.
[15] BLUM A, MEYER JB, RAYMOND A, et al. CT of hip prosthesis: New techniques and new paradigms. Diagn Interv Imaging.2016; 97(7-8):725-733.
[16] KHAN RJK, LAM LO, BREIDAHL W, et al. Magnetic resonance imaging features of preserved vs divided and repaired piriformis during total hip arthroplasty: a randomized controlled trial. J Arthroplasty. 2012; 27(4): 551-558.
[17] 艾英风.X线、CT及MRI对髋关节置换术后并发症的诊断价值[J]. 内蒙古医学杂志,2017,49(6):714-716.
[18] 李长军.X线、CT及MRI对髋关节置换术后并发症的诊断价值研究[J]. 中外医疗,2016,35(15):166-167.
[19] 刘红. X线、CT及MRI对髋关节置换术后并发症的诊断价值[J]. 影像研究与医学应用,2017,1(8):225-226.
[20] MARATT JD, GAGNIER JJ, BUTLER PD, et al. No Difference in Dislocation Seen in Anterior Vs Posterior Approach Total Hip Arthroplasty. J Arthroplasty. 2016;31(9 Suppl):127-130.
[21] VIDT ME, SANTAGO II AC, TUOHY CJ, et al. Assessments of fatty infiltration and muscle atrophy from a single magnetic resonance image slice are not predictive of 3-Dimensional measurements. Arthroscopy.2016;32(1):128-139.
[22] BABA T, HOMMA Y, TAKAZAWA N, et al. Is urinary incontinence the hidden secret complications after total hip arthroplasty? Eur J Orthop Surg Traumatol. 2014;24(8):1455-1460.
[23] LINDGREN K, ANDERSON MB, PETERS CL, et al. The prevalence of positive findings on metal artifact reduction sequence magnetic resonance imaging in metal-on-metal total hip arthroplasty. J Arthroplasty. 2016;31(7):1519-1523.
[24] JUNGMANN PM, CHRISTOPH A, AGTEN MD, et al. Advances in MRI around metal. J Magn Reson Imaging. 2017;46(4):972-991.
[25] KOVALAK E, ÖZDEMIR H, ERMUTLU C, et al. Assessment of hip abductors by MRI after total hip arthroplasty and effect of fatty atrophy on functional outcome. Acta Orthop Traumatol Turc. 2018; 52(3):196-200.
[26] APAYDIN N, KENDIR S, LOUKAS M, et al. Surgical anatomy of the superior gluteal nerve and landmarks for its localization during minimally invasive approaches to the hip. Clin Anat. 2013;26(5): 614-620.
[27] MÜLLER M, TOHTZ S, DEWEY M, et al. Evidence of reduced muscle trauma through a minimally invasive anterolateral approach by means of MRI. Clin Orthop Relat Res. 2010; 468(12): 3192-3200.
[28] PFIRRMANN CWA, NOTZLI HP, DORA C, et al. Abductor tendons and muscles assessed at MR imaging after total hip arthroplasty in asymptomatic and symptomatic patients. Radiology. 2005;235(3):969-976.
[29] URBANEK H, VAN DER SMAGT P. iEMG: Imaging electromyography. J Electromyogr Kinesiol. 2016;27:1-9.
[30] MÜLLER M, TOHTZ S, WINKLER T, et al. MRI findings of gluteus minimus muscle damage in primary total hip arthroplasty and the influence on clinical outcome. Arch Orthop Trauma Surg. 2010; 130(7):927-935.
[31] WANG Z, HOU J, WU C, et al. A systematic review and meta-analysis of direct anterior approach versus posterior approach in total hip arthroplasty. J Orthop Surg Res.2018;13(1): 229.
[32] VADALÀAP, MAZZA D, DESIDERI D, et al. Could the tendon degeneration and the fatty infiltration of the gluteus medius affect clinical outcome in total hip arthroplasty? Int Orthop. 2020;44(2): 275-282.
[33] LAFFOSSE JM, ACCADBLED F, MOLINIER F, et al. Anterolateral mini-invasive versus posterior mini-invasive approach for primary total hip replacement. Comparison of exposure and implant positioning. Arch Orthop Trauma Surg. 2008; 128(4): 363-369.
[34] 邓昶,李盛华,周明旺. SuperPATH入路微创全髋关节置换术的研究进展[J]. 中国微创外科杂志,2018,18(2):169-172.
[35] COHEN RG, KATZ JA, SKREPNIK NV. The relationship between skeletal muscle serum markers and primary THA: a pilot study. Clin Orthop Relat Res. 2009;467(7): 747-1752.
[36] BERGIN PF, DOPPELT JD, KEPHART CJ, et al. Comparison of minimally invasive direct anterior versus posterior total hip arthroplasty based on inflammation and muscle damage markers. J Bone Joint Surg Am. 2011; 93(15): 1392-1398.
[37] CHEN XX, WANG T, LI J, et al. Relationship between Inflammatory Response and Estimated Complication Rate after Total Hip Arthroplasty. Chin Med J (Engl). 2016;129(21): 2546-2551.
[38] LIN E, CALVANO SE, LOWRY SF. Inflammatory cytokines and cell response in surgery. Surgery. 2000;127(2):117-126.
[39] RUIZ-CABELLO J, CARRERO-GONZÁLEZ B, AVILÉS P, et al. Magnetic resonance imaging in the evaluation of inflammatory lesions in muscular and soft tissues: an experimental infection model induced by Candida albicans. Magn Reson Imaging. 1999; 17(9):1327-1334.
[40] OUYANG L, ZENG S, ZHENG G, et al. Early inflammatory response following traumatic brain injury in rabbits using USPIO- and Gd-Enhanced MRI. Biomed Res Int, 2016;2016: 8431987. [41] AMIRABADI A, VIDARSSON L, MILLER E, et al. USPIO-related T1 and T2 mapping MRI of cartilage in a rabbit model of blood-induced arthritis: a pilot study. Haemophilia. 2015;21(1): e59-69. |
| [1] | Min Youjiang, Yao Haihua, Sun Jie, Zhou Xuan, Yu Hang, Sun Qianpu, Hong Ensi. Effect of “three-tong acupuncture” on brain function of patients with spinal cord injury based on magnetic resonance technology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(在线): 1-8. |
| [2] | Pu Rui, Chen Ziyang, Yuan Lingyan. Characteristics and effects of exosomes from different cell sources in cardioprotection [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(在线): 1-. |
| [3] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Comparison of the short-term efficacy of extracorporeal shock wave therapy for middle-aged and elderly knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1471-1476. |
| [4] | Jiang Yong, Luo Yi, Ding Yongli, Zhou Yong, Min Li, Tang Fan, Zhang Wenli, Duan Hong, Tu Chongqi. Von Mises stress on the influence of pelvic stability by precise sacral resection and clinical validation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1318-1323. |
| [5] | Zhang Yu, Tian Shaoqi, Zeng Guobo, Hu Chuan. Risk factors for myocardial infarction following primary total joint arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1340-1345. |
| [6] | Li Dadi, Zhu Liang, Zheng Li, Zhao Fengchao. Correlation of total knee arthroplasty efficacy with satisfaction and personality characteristics [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1346-1350. |
| [7] | Wei Wei, Li Jian, Huang Linhai, Lan Mindong, Lu Xianwei, Huang Shaodong. Factors affecting fall fear in the first movement of elderly patients after total knee or hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1351-1355. |
| [8] | Wang Jinjun, Deng Zengfa, Liu Kang, He Zhiyong, Yu Xinping, Liang Jianji, Li Chen, Guo Zhouyang. Hemostatic effect and safety of intravenous drip of tranexamic acid combined with topical application of cocktail containing tranexamic acid in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1356-1361. |
| [9] | Xiao Guoqing, Liu Xuanze, Yan Yuhao, Zhong Xihong. Influencing factors of knee flexion limitation after total knee arthroplasty with posterior stabilized prostheses [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1362-1367. |
| [10] | Peng Zhihao, Feng Zongquan, Zou Yonggen, Niu Guoqing, Wu Feng. Relationship of lower limb force line and the progression of lateral compartment arthritis after unicompartmental knee arthroplasty with mobile bearing [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1368-1374. |
| [11] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [12] | Yao Rubin, Wang Shiyong, Yang Kaishun. Minimally invasive transforaminal lumbar interbody fusion for treatment of single-segment lumbar spinal stenosis improves lumbar-pelvic balance [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1387-1392. |
| [13] | Wang Haiying, Lü Bing, Li Hui, Wang Shunyi. Posterior lumbar interbody fusion for degenerative lumbar spondylolisthesis: prediction of functional prognosis of patients based on spinopelvic parameters [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1393-1397. |
| [14] | Lü Zhen, Bai Jinzhu. A prospective study on the application of staged lumbar motion chain rehabilitation based on McKenzie’s technique after lumbar percutaneous transforaminal endoscopic discectomy [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1398-1403. |
| [15] | Zhang Shangpu, Ju Xiaodong, Song Hengyi, Dong Zhi, Wang Chen, Sun Guodong. Arthroscopic suture bridge technique with suture anchor in the treatment of acromioclavicular dislocation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1417-1422. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||