Chinese Journal of Tissue Engineering Research ›› 2021, Vol. 25 ›› Issue (21): 3409-3415.doi: 10.3969/j.issn.2095-4344.3851
Previous Articles Next Articles
Efficacy of anterolateral minimally invasive approach versus traditional posterolateral approach in total hip arthroplasty: a meta-analysis
Fu Panfeng, Shang Wei, Kang Zhe, Deng Yu, Zhu Shaobo
- Department of Orthopedic Surgery, Zhongnan Hospital, Wuhan University, Wuhan 430071, Hubei Province, China
-
Received:2020-08-05Revised:2020-08-11Accepted:2020-09-11Online:2021-07-28Published:2021-01-25 -
Contact:Zhu Shaobo, MD, Chief physician, Department of Orthopedic Surgery, Zhongnan Hospital, Wuhan University, Wuhan 430071, Hubei Province, China -
About author:Fu Panfeng, Physician, Department of Orthopedic Surgery, Zhongnan Hospital, Wuhan University, Wuhan 430071, Hubei Province, China
CLC Number:
Cite this article
Fu Panfeng, Shang Wei, Kang Zhe, Deng Yu, Zhu Shaobo. Efficacy of anterolateral minimally invasive approach versus traditional posterolateral approach in total hip arthroplasty: a meta-analysis[J]. Chinese Journal of Tissue Engineering Research, 2021, 25(21): 3409-3415.
share this article
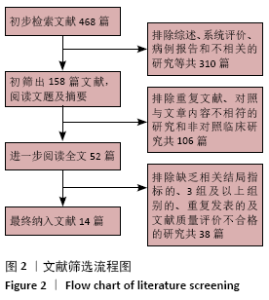
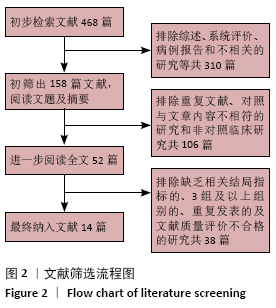
2.1 文献搜索结果 依据上述检索策略,共检索相关文献468篇。经阅读文题和(或)摘要后剔除明显不符合纳入标准的文献,并进一步阅读全文,最终纳入文献14篇[11-24]。共纳入患者共1 160例,试验组(微创ALA)583例,对照组(常规PLA)577例。文献筛选流程及结果见图2。"
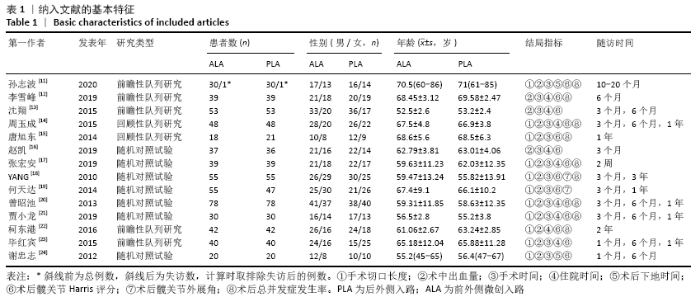
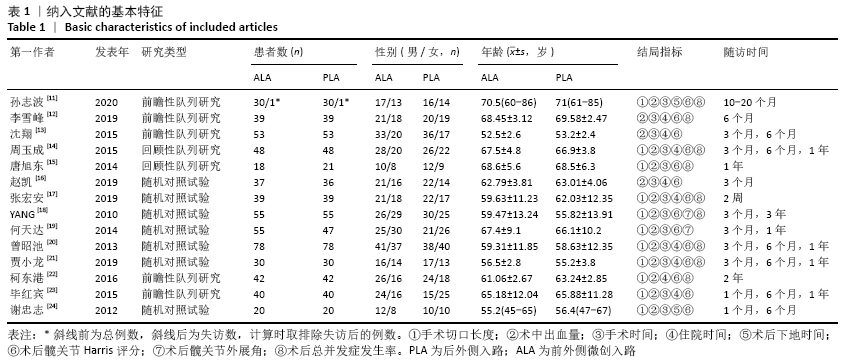
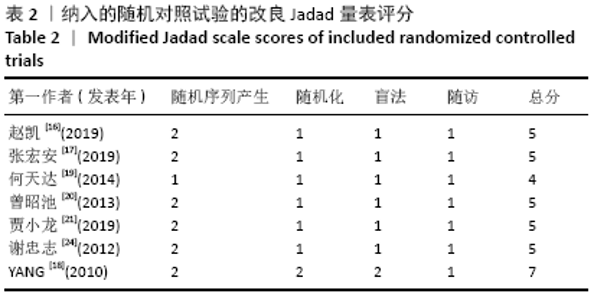
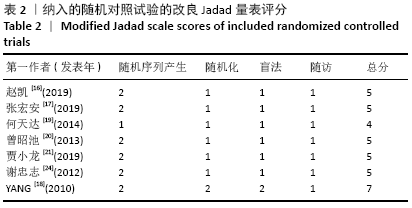
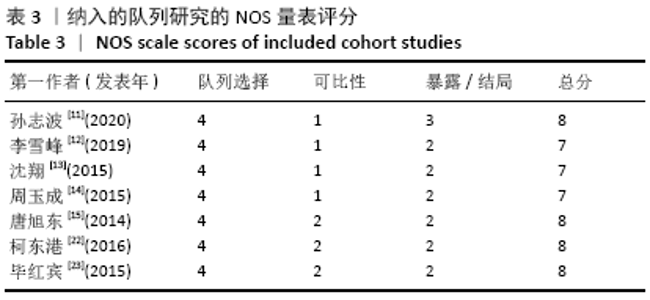
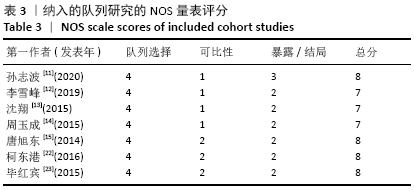
2.2 文献基本特征及质量评价 纳入的14项研究中含7项随机对照试 验[16-21,24],7项队列研究[11-15,22-23]。此7项随机对照试验的改良Jadad评分均至少4分,此7项队列研究的NOS量表评分均至少7颗星,故纳入的14项研究均为高质量研究。纳入文献的基本特征及质量评价见表1-3。"
"
"
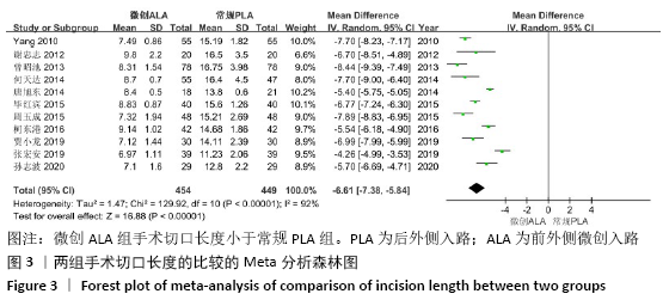
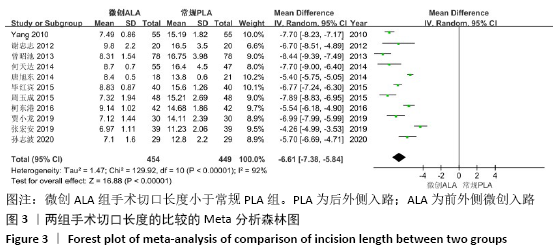
2.3 Meta分析结果 2.3.1 各组手术切口长度的比较 手术切口长度是临床患者关注的重点,也是评判患者手术创伤大小最常用的指标之一。纳入的11篇文献对微创ALA与常规PLA组手术切口长度进行了比较[11,14-15,17-24],此结局指标为连续性变量,用MD作为合并统计量。各研究结果间存在明显异质性(P < 0.000 01,I2=92%),根据年龄、性别和研究类型分组进行亚组分析,异质性无明显变化;逐一去除研究,异质性亦无明显变化。异质性分析未发现明确的异质性来源,临床一致性良好,采用随机效应模型分析。结果显示,微创ALA组手术切口长度小于常规PLA组(MD=-6.61,95%CI:-7.38至-5.84,P < 0.000 01),见图3。将随机效应模型更换为固定效应模型,结果无明显变化(MD=-6.26,95%CI:-6.46至-6.07,P < 0.000 01),表明稳定性良好。 "
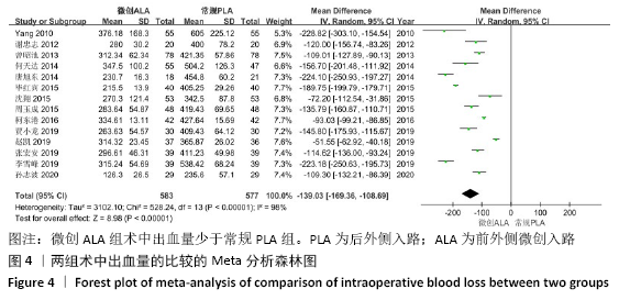
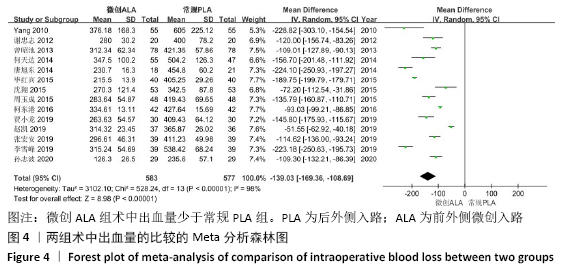
2.3.2 各组术中出血量的比较 术中出血量也是临床医护用来评价手术疗效的重要指标,直接或间接关系到手术安全、术后恢复及治疗费用。纳入的14篇文献都对微创ALA组与常规PLA组术中出血量进行了比较[11-24],此结局指标为连续性变量,用MD作为合并统计量。各研究结果间存在明显异质性(P < 0.000 01,I2=98%),根据年龄、性别和研究类型分组进行亚组分析,发现年龄对异质性有一定影响;逐一去除研究,异质性无明显变化。异质性分析发现年龄因素可能是异质性来源,采用随机效应模型分析。结果显示,微创ALA组术中出血量少于常规PLA组(MD=-139.03,95%CI: -169.36至-108.69,P < 0.000 01),见图4。将随机效应模型更换为固定效应模型,结果无明显变化(MD=-115.50,95%CI: -119.65至-111.35,P < 0.000 01),表明结果稳定性良好。 "
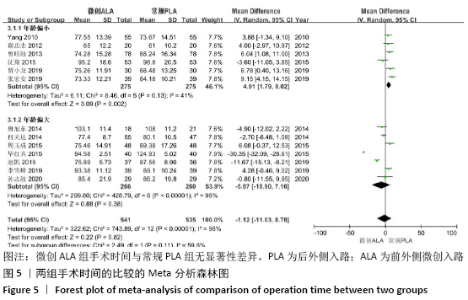
2.3.3 各组手术时间的比较 手术时间决定因素较多,除了手术入路,也是麻醉水平及术者对手术的熟练程度的综合反映。纳入的13篇文献对微创ALA组与常规PLA组手术时间进行了比较[11-21,23-24],此结局指标为连续性变量,用MD作为合并统计量。各研究结果间存在明显异质性(P < 0.000 01,I2=98%),根据年龄、性别及研究类型分组进行亚组分析,年龄亚组分析结果见图5,其他亚组异质性无明显变化;逐一去除研究,异质性亦无明显变化。除年龄因素可能是异质性来源外,术者的熟练度也可能作为异质性来源,故采用随机效应模型分析。结果显示,在年龄偏小亚组中,微创ALA组手术时间略多于常规PLA组(MD=4.91,95%CI:1.79-8.02,P=0.002);在年龄偏大亚组中,两组手术时间无明显差异(P=0.38);总体而言,微创ALA组手术时间与常规PLA组无显著性差异(MD= -1.12,95%CI:-11.03-8.78,P=0.82),见图5。将随机效应模型更换为固定效应模型,结果差异有显著性意义(MD= -13.17,95%CI:-14.31至-12.02,P < 0.000 01),考虑为固定效应模型运算时忽略异质性造成的假阳性误差,此时更为保守的随机效应模型结果更为可信。"

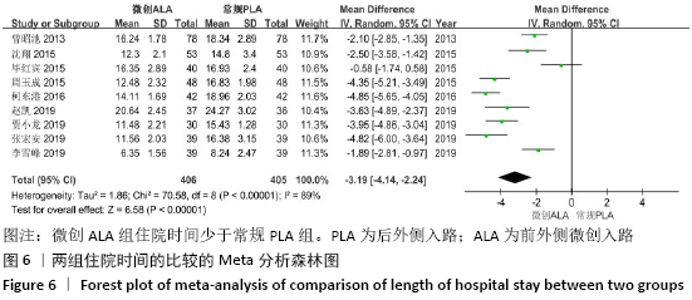
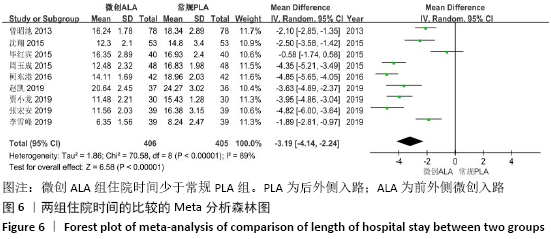
2.3.4 各组住院时间的比较 住院时间是由围术期多种因素共同决定的,除了手术疗效本身,还包括术前慢性病管理、术后感染控制、营养支持以及医疗保险等社会因素方面。纳入的9篇文献对微创ALA组与常规PLA组住院时间进行了比较[12-14,16-17,20-23],此结局指标为连续性变量,用MD作为合并统计量。各研究结果间存在明显异质性(P < 0.000 01,I2=89%),根据年龄、性别及研究类型分组进行亚组分析,异质性无明显变化;逐一去除研究,异质性亦无明显变化。异质性分析未发现明确的异质性来源,临床一致性良好,采用随机效应模型分析。结果显示,微创ALA组住院时间少于常规PLA组(MD=-3.19,95%CI: -4.14至-2.24,P < 0.000 01),见图6。将随机效应模型更换为固定效应模型,结果无显著变化(MD=-3.24,95%CI: -3.56至-2.93,P < 0.000 01),表明结果稳定性良好。 "
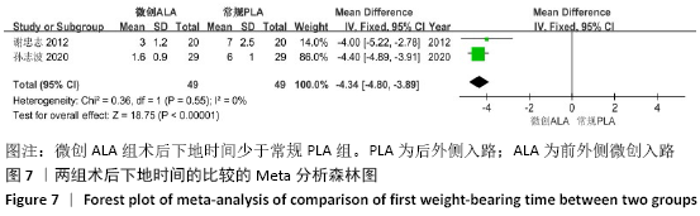
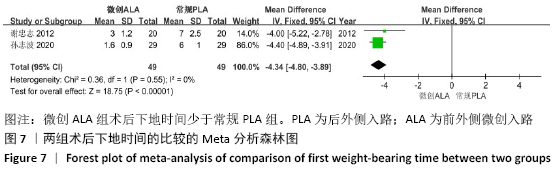
2.3.5 各组术后下地时间的比较 早期下床活动可减少卧床导致的下肢深静脉血栓、肺部及泌尿系感染等并发症,利于术后恢复。纳入的2篇文献对微创ALA组与常规PLA组术后下地时间进行了比较[11,24],此结局指标为连续性变量,用MD作为合并统计量。各研究结果间同质性良好(P=0.55,I2=0%),故采用固定效应模型分析。结果显示,微创ALA组术后下地时间少于常规PLA组(MD=-4.34,95%CI:-4.80至-3.89,P < 0.000 01),见图7。失效安全数Nfs0.05= 213.28,说明至少需要214篇阴性结果的文献才能使效应逆转。将固定效应模型更换为随机效应模型,结果无显著变化(MD=-4.34,95%CI:-4.80至-3.89,P < 0.000 01),表明结果稳定性良好。 "

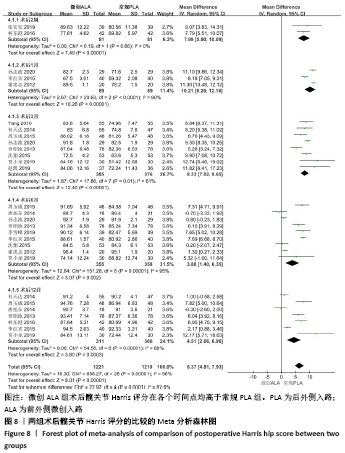
2.3.6 各组术后髋关节功能的比较 髋关节Harris评分采用标准的百分制评分,包括疼痛、功能、畸形和关节活动度4个方面,是目前国内外使用最广的髋关节评分方法。纳入的14篇文献都对微创ALA组与常规PLA组术后髋关节Harris评分进行了比较[11-24],此结局指标为连续性变量,用MD作为合并统计量。各研究结果间存在明显异质性(P < 0.000 01,I2=96%),根据术后具体时间不同划分亚组,见图8,采用随机效应模型分析。结果显示,微创ALA组术后髋关节Harris评分在各个时间点均高于常规PLA组(MD=6.37,95%CI:4.81-7.93,P < 0.000 01),见图8。亚组之间异质性较大(P=0.000 1,I2=82.6%),考虑是各纳入文献随访时间跨度较大,故而导致了亚组之间偏倚的潜在可能。逐一去除研究,术后1个月亚组分析去除1篇文献后[21],亚组内异质性明显下降,效应值无明显变化,总体异质性及效应值无明显变化;术后3个月亚组去除文献[18]时,亚组内异质性明显下降,效应值无明显变化,总体异质性及效应值无明显变化。将随机效应模型更换为固定效应模型,结果无显著变化(MD=6.44,95%CI:6.14-6.75,P < 0.000 01),表明结果稳定性良好。 "
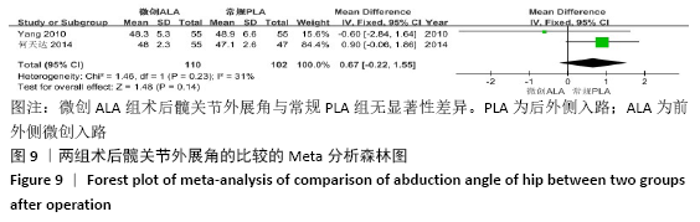
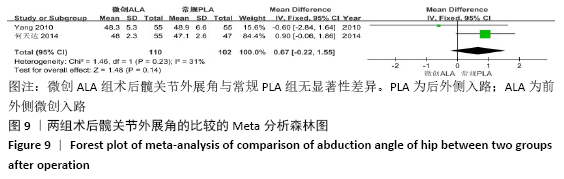
2.3.7 各组术后髋关节外展角的比较 髋关节外展角是影像学上评价全髋关节置换后疗效常用的指标,置入髋臼假体的角度不良会缩短假体寿命、导致术后髋关节不稳定并增加并发症发生率。纳入的2篇文献对微创ALA组与常规PLA组术后髋关节外展角进行了比较[18-19],此结局指标为连续性变量,用MD作为合并统计量。各研究结果间同质性良好(P=0.23,I2=31%),故采用固定效应模型分析。结果显示,微创ALA组术后髋关节外展角与常规PLA组比较无显著性差异(MD=0.67,95%CI:-0.22-1.55,P=0.14),见图9。失效安全数Nfs0.05=-1.34,说明至少需要2篇阳性结果的文献才能使效应逆转。将固定效应模型更换为随机效应模型,结果无显著变化(MD=0.50,95%CI:-0.79-1.80,P=0.45),表明结果稳定性良好。 "
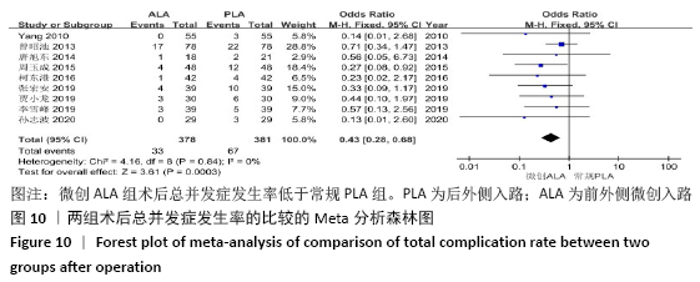
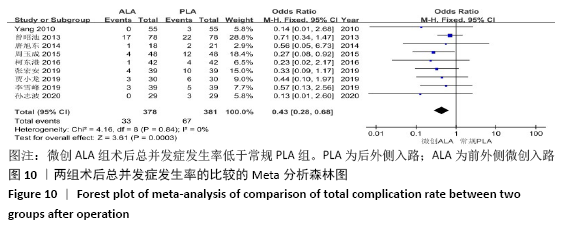
2.3.8 各组术后总并发症发生率的比较 术后总体并发症发生率能直观反映术后疗效,和患者术后生活质量息息相关,并发症严重时可能需行翻修手术。有9篇文献提及微创ALA组与常规PLA组术后并发症发生情况[11-12,14-15,17-18,20-22],此结局指标为分类变量,用OR作为合并统计量。各研究结果间同质性良好(P=0.84,I2=0%),故采用固定效应模型分析。结果显示,微创ALA组术后总并发症发生率低于常规PLA组(OR=0.43,95%CI:0.28- 0.68,P=0.000 3),见图10。将固定效应模型更换为随机效应模型,结果无显著变化(OR=0.45,95%CI:0.29-0.72,P=0.000 8),表明结果稳定性良好。 "
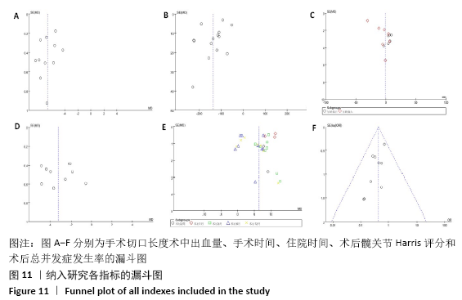
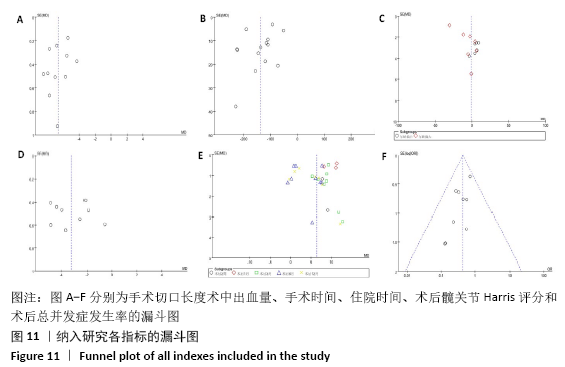
2.4 发表偏倚分析 漏斗图分析显示,纳入研究的手术切口长度、术中出血量、手术时间、住院时间、术后髋关节Harris评分和术后总并发症发生率指标的漏斗图基本对称,说明可能无发表偏倚,见图11。"
| [1] HARMAN C. Total hip arthroplasty after hip fracture. BMJ. 2016;353:i2217. [2] 卢钰,解京明,张颖,等.全髋关节置换微创手术入路的应用现状[J].山东医药,2018, 58(32):92-94. [3] 韩广弢,李皓桓.全髋关节置换不同手术入路的研究进展[J].疑难病杂志,2019,18(5): 537-540. [4] JONES RD. Bibliography Current World Literature. Curr Opin Orthop. 2005;16(1):38-44. [5] Rottinger H. Minimally invasive anterolateral surgical approach for total hip arthroplasty: early clinical results. Hip Int. 2006;16 Suppl 4: 42-47. [6] NAKAI T, LIU N, FUDO K, et al. Early complications of primary total hip arthroplasty in the supine position with a modified Watson-Jones anterolateral approach. J Orthop. 2014; 11(4):166-169. [7] JADAD AR, MOORE RA, CARROLL D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17(1):1-12. [8] WELLS GA, SHEA B, O’CONNNELL D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses. [2013-05-08]. https://xueshu.baidu. com/usercenter/paper/show? paperid=a4fb78f2f92ab7b34369c876030 d2026&site=xueshu_se. [9] 王珍,张永红,徐巧巧.几种发表性偏倚评估方法介绍[J].中国卫生统计,2009,26(5):539-541. [10] 麦劲壮,李河,方积乾,等.Meta分析中失安全系数的估计[J].循证医学,2006,6(5):297-300. [11] 孙志波,钱炜,李相伟,等.仰卧位微创前外侧入路人工全髋关节置换的疗效分析[J].局解手术学杂志,2020,29(2):107-110. [12] 李雪峰.微创前外侧入路下全髋置换治疗股骨颈骨折的临床效果[J].河南医学研究,2019, 28(17):3133-3134. [13] 沈翔,张淑云.前外侧小切口与常规后外侧切口全髋关节置换的疗效对比[J].现代诊断与治疗,2015,26(23):5378-5379. [14] 周玉成,李云华.不同手术入路全髋关节置换临床疗效分析[J].浙江创伤外科,2015, 20(2):219-221. [15] 唐旭东,陈安富,黄凯,等.前外侧微创入路与后外侧常规入路全髋关节置换的临床研究[J].实用医院临床杂志,2014,11(3):106-108. [16] 赵凯,袁宏伟.经前外侧入路微创小切口全髋关节置换治疗股骨颈骨折患者的短期临床研究[J].医药论坛杂志,2019(7):59-60. [17] 张宏安, 王飞.不同手术入路对全髋关节置换患者围术期指标、HSS评分及术后并发症的影响[J].中国伤残医学,2019,27(8):37-38. [18] YANG C, ZHU Q, HAN Y, et al. Minimally-invasive total hip arthroplasty will improve early postoperative outcomes: a prospective, randomized, controlled trial. Ir J Med Sci. 2010; 179:285-290. [19] 何天达.全髋关节置换采用前外侧入路小切口的效果观察[J].常州实用医学,2014,30(5): 289-291. [20] 曾昭池,郭中凯,朱志勇,等.微创与常规全髋关节置换的临床疗效比较[J].中国矫形外科杂志,2013,21(12):1173-1176. [21] 贾小龙.不同手术入路在全髋关节置换中的应用效果对比[J].现代医学与健康研究,2019, 3(6):54-55. [22] 柯东港,路坦.手术入路对人工全髋关节置换患者预后影响的2年随访观察[J].安徽医药, 2016,20(6):1140-1142. [23] 毕红宾,王永清,赵志辉,等.前外侧微创入路和传统后侧入路行全髋关节置换的疗效比较[J].中国中医骨伤科杂志,2015,23(2):44-46. [24] 谢忠志,梁斌,尹东,等.外侧小切口髋关节前入路初次人工全髋关节置换疗效分析[J].实用医学杂志,2012,28(4):603-605. [25] Organisation for Economic Co-operation and Development. OECD health data. 2017. http://dx.doi.org/10.1787/health-data-en (accessed Jul 20, 2020). [26] HOOPER G, LEE AJ-J, ROTHWELL A, et al. Current trends and projections in the utilisation rates of hip and knee replacement in New Zealand from 2001 to 2026. NZ Med J. 2014;127:82-93. [27] YOON PW, LEE YK, AHN J, et al. Epidemiology of hip replacements in Korea from 2007 to 2011. J Korean Med Sci. 2014;29:852-858. [28] 王俏杰,张先龙.人工髋关节置换的现状与热点[J].中华关节外科杂志(电子版),2015, 9(6):26-31. [29] PETIS S, HOWARD JL, LANTING BL, et al. Surgical approach in primary total hip arthroplasty: anatomy, technique and clinical outcomes. Can J Surg. 2015;58(2):128-139. [30] 徐峰,袁凯旋,陈圣宝,等.髋关节功能评分研究进展[J].国际骨科学杂志,2018,39(3): 141-144. |
| [1] | Hu Kai, Qiao Xiaohong, Zhang Yonghong, Wang Dong, Qin Sihe. Treatment of displaced intra-articular calcaneal fractures with cannulated screws and plates: a meta-analysis of 15 randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1465-1470. |
| [2] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Comparison of the short-term efficacy of extracorporeal shock wave therapy for middle-aged and elderly knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1471-1476. |
| [3] | Xu Feng, Kang Hui, Wei Tanjun, Xi Jintao. Biomechanical analysis of different fixation methods of pedicle screws for thoracolumbar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1313-1317. |
| [4] | Jiang Yong, Luo Yi, Ding Yongli, Zhou Yong, Min Li, Tang Fan, Zhang Wenli, Duan Hong, Tu Chongqi. Von Mises stress on the influence of pelvic stability by precise sacral resection and clinical validation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1318-1323. |
| [5] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [6] | Zhang Yu, Tian Shaoqi, Zeng Guobo, Hu Chuan. Risk factors for myocardial infarction following primary total joint arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1340-1345. |
| [7] | Wei Wei, Li Jian, Huang Linhai, Lan Mindong, Lu Xianwei, Huang Shaodong. Factors affecting fall fear in the first movement of elderly patients after total knee or hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1351-1355. |
| [8] | Wang Jinjun, Deng Zengfa, Liu Kang, He Zhiyong, Yu Xinping, Liang Jianji, Li Chen, Guo Zhouyang. Hemostatic effect and safety of intravenous drip of tranexamic acid combined with topical application of cocktail containing tranexamic acid in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1356-1361. |
| [9] | Xiao Guoqing, Liu Xuanze, Yan Yuhao, Zhong Xihong. Influencing factors of knee flexion limitation after total knee arthroplasty with posterior stabilized prostheses [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1362-1367. |
| [10] | Huang Zexiao, Yang Mei, Lin Shiwei, He Heyu. Correlation between the level of serum n-3 polyunsaturated fatty acids and quadriceps weakness in the early stage after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1375-1380. |
| [11] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [12] | Wang Haiying, Lü Bing, Li Hui, Wang Shunyi. Posterior lumbar interbody fusion for degenerative lumbar spondylolisthesis: prediction of functional prognosis of patients based on spinopelvic parameters [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1393-1397. |
| [13] | Lü Zhen, Bai Jinzhu. A prospective study on the application of staged lumbar motion chain rehabilitation based on McKenzie’s technique after lumbar percutaneous transforaminal endoscopic discectomy [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1398-1403. |
| [14] | Chen Xinmin, Li Wenbiao, Xiong Kaikai, Xiong Xiaoyan, Zheng Liqin, Li Musheng, Zheng Yongze, Lin Ziling. Type A3.3 femoral intertrochanteric fracture with augmented proximal femoral nail anti-rotation in the elderly: finite element analysis of the optimal amount of bone cement [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1404-1409. |
| [15] | Du Xiupeng, Yang Zhaohui. Effect of degree of initial deformity of impacted femoral neck fractures under 65 years of age on femoral neck shortening [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1410-1416. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||