Chinese Journal of Tissue Engineering Research ›› 2016, Vol. 20 ›› Issue (26): 3946-3952.doi: 10.3969/j.issn.2095-4344.2016.26.022
Strategy and adjuvant therapy of internal fixation implant and external fixation stent for treating tibial fracture nonunion
Hong Fan, Xie Jia-bing, Ding Guo-zheng
- Department of Trauma Orthopedics, the First Affiliated Hospital of Wannan Medical College, Wuhu 241001, Anhui Province, China
-
Revised:2016-05-06Online:2016-06-24Published:2016-06-24 -
Contact:Ding Guo-zheng, Master’s supervisor, Chief physician, Department of Trauma Orthopedics, the First Affiliated Hospital of Wannan Medical College, Wuhu 241001, Anhui Province, China -
About author:Hong Fan, Studying for master’s degree, Physician, Department of Trauma Orthopedics, the First Affiliated Hospital of Wannan Medical College, Wuhu 241001, Anhui Province, China -
Supported by:the Science and Technology Project of Wuhu City of Anhui Province, No. 2008726; the Key Scientific Research Project of Wannan Medical College, No. WK2014ZF14
CLC Number:
Cite this article
Hong Fan, Xie Jia-bing, Ding Guo-zheng. Strategy and adjuvant therapy of internal fixation implant and external fixation stent for treating tibial fracture nonunion[J]. Chinese Journal of Tissue Engineering Research, 2016, 20(26): 3946-3952.
share this article
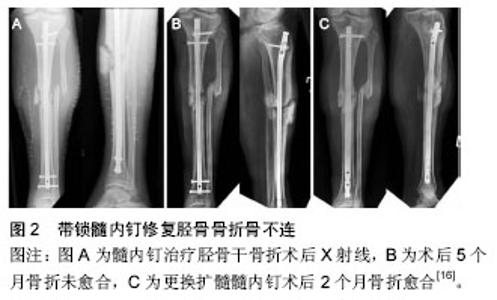
2.1 胫骨骨折骨不连发生的基本原因 胫骨骨折骨不连与很多因素有关。大部分骨不连都与最初的创伤有很大关系,还与患者伤后的健康状态和行为有关。被文献报道过的其他因素包括骨折端移位、骨质疏松、并发腓骨骨折、粉碎性骨折和感染。严重开放性骨折更易发生延迟愈合。创伤时的骨与软组织所吸收的能量直接影响着创伤的愈合,因此创伤本身对骨不连的发生起着决定性的作用[5-6]。 在结构因素中,创伤后胫骨血供的保留程度通常决定着胫骨骨折愈合概率。对胫骨血供的解剖结构已了解地很详细[7]。影响胫骨血供的3个主要血管系统分别是滋养血管系统、骨膜血管系统和骨骺血管系统。对于胫骨干骨折最重要的是滋养血管系统和骨膜血管系统。沿胫骨后方下降,在胫骨的中、上1/3交界处后方通过滋养孔进入胫骨,随后分成升、降支,升、降支再反复分支,分布于骨体,并与骨骺动脉相吻合,形成骨膜下血管网。滋养动脉从骨内为胫骨供血,占骨内皮质供血的90%。胫骨中1/3骨折时,骨内血供常常会被破坏。但骨不连概率在胫骨干上、中、下1/3的分布几乎是均等的。骨膜的血供部分来自周围软组织血管,但主要是由胫前动脉提供。尽管胫骨骨膜的后方与侧方有丰富的血供,但前内侧的的皮下骨膜血供却很匮乏。 多种患者自身因素也被证明与骨不连的发生有关。营养不良是其中一种因素,而这种因素常常被忽略。骨折的愈合需要充分的蛋白质和足够的热量,蛋白质的缺乏和热量摄取不足都将增加骨不连的发生率[8]。Pourfeizi等[9]的研究显示维生素D缺乏可导致骨不连。甲状旁腺功能亢进可导致维生素D的缺乏。由于甲状旁腺功能亢进的高发生率,其成为不名原因的胫骨骨折骨不连的一种可能原因[10]。吸烟也是一种导致胫骨骨折骨不连的可能原因。虽然没有充分证据,但香烟中的烟碱成分很可能会损害骨折端的血管及细胞的功能。 2.2 胫骨骨折骨不连的治疗 对胫骨骨折不恰当的处理措施同样会增加骨不连的发生率。不恰当的治疗对骨折端的干扰及对骨折端固定不牢固都会延长骨折愈合的时间。 2.2.1 修复方案制定 如果想要制定对胫骨骨折延迟愈合的最佳治疗方案,就要先对延迟愈合的生物及机械因素进行严格评估。骨折的定位和分型、开放骨折的分类以及任何过去的感染史和手术史都是患者病史必要的部分。体格检查可以了解软组织的状态、是否存在窦道以及足部神经血管的状态。影像学检查应该尽早拍摄来评估骨折端对位情况。骨质疏松是一种骨缺陷,限制了骨折的处理措施。因此患者应该尽早被确诊是否有骨质疏松。感染、软组织缺损及骨折端对线不良都会完全改变胫骨骨折延迟愈合的治疗选择。患处的生物问题和机械问题都要被解决才能完全被治愈。闭合无感染并且对线良好的延迟愈合,只需通过治疗来使骨折端愈合即可。后外侧植骨、闭合绞锁髓内钉和植骨或不植骨的加压钢板固定术都是可行的治疗方法。在延迟愈合由于感染而无法使用内固定及植骨时,可以先对患处彻底的清创并保证软组织的覆盖。 2.2.2 固定修复 髓内钉:髓内钉现在已经被广泛应用到无感染的胫骨骨折骨不连的治疗中。目前主要应用于胫骨骨折骨不连治疗的髓内钉有扩髓髓内钉和带锁髓内钉。髓内钉技术是目前不稳定的胫骨骨折治疗中最常见的固定方法[11-12]。因此,现在在临床上遇到的大部分胫骨骨折延迟愈合的患者已经进行过髓内钉固定。扩髓髓内钉治疗对已进行过髓内钉固定的胫骨骨不连有明显的效果。Hernández-Vaquero等[13]的研究证明应用扩髓髓内钉治疗骨不连是安全有效的。在无感染的胫骨骨折骨不连的治疗中,扩髓髓内钉的绞刀的自发成骨效应刺激骨折端愈合。带锁髓内钉联合植骨同样在胫骨骨折骨不连的治疗中取得了成功。王志勇等[14]对21例胫骨骨不连患者进行带锁髓内钉联合植骨治疗,其中18例取得了良好疗效。带锁髓内钉结合植骨治疗缺损较大的胫骨骨不连有显著疗效。在对缺损较严重的胫骨骨折骨不连进行带锁髓内钉治疗时,可联合植骨来提高成功率。Ding等[15]从2008年2月至2010年10月对18例胫骨骨折骨不连患者进行带锁髓内钉结合植骨治疗,其中男12例,女6例;患者年龄31-67岁,平均42岁;从受伤到进行骨不连手术的时间为6-18个月,平均8个月。Ding等对患者进行12-36个月的术后随访,平均18个月,未出现伤口感染及皮肤坏死,所有患者均未出现骨不连、感染、畸形及再骨折,骨不连愈合的时间4-8个月,平均6个月。与加压钢板固定相比,髓内钉的优势在于早期实现患肢的全部功能活动,包括负重及关节活动,见图2。在软组织损伤严重的病例中,髓内钉是更好的选择[16]。 "

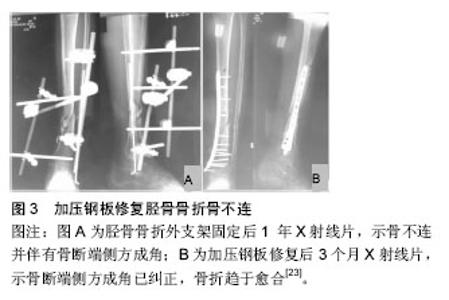
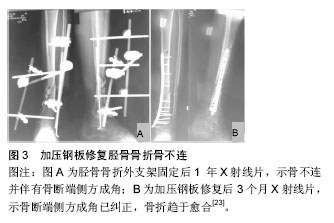
加压钢板:Muller最先提出使用加压钢板来治疗无感染的闭合性胫骨骨不连[17]。现在加压钢板已经被普遍应用在胫骨骨折骨不连的治疗当中,并取得了良好的疗效[18-19]。单独使用加压钢板治疗肥大型骨不连的成功率高,但对于萎缩型骨不连需要进行植骨治疗。加压钢板最常应用于未感染的成角型胫骨骨不连。钢板置于骨不连的张力侧时能够对骨折端进行调整,独立的张力牵拉装置增加了附加应力,进而构成了一个骨折重组的模型。随着加压钢板种类的不断更新与创新,越来越多的不同种类的钢板被应用到胫骨骨不连的治疗中,见图3。锁定加压钢板可以应用在行髓内钉治疗后的胫骨骨不连患者的治疗中。Ye等[20]对6例长骨骨折髓内钉治疗后骨不连的患者进行锁定加压钢板固定,所有患者骨折端正常愈合,并且未出现任何并发症。Ye等[20]认为是锁定加压钢板的操作便捷、创伤小、疗效好等优势使其取得了成功。近来章莹等[21]应用锁定加压钢板外置技术对11例胫骨感染性骨不连患者进行了治疗,其中男7例,女4例;年龄20-55岁,平均35.6岁;所有患者术后随访10-26个月,平均14.3个月。其中9例正常愈合,2例出现延迟愈合,疗效显著。锁定加压钢板外置相比外固定架的优势在于外形小,对患者的活动影响较小。该研究使得加锁定压钢板治疗感染性骨不连成为可能。对有较大缺损的胫骨骨不连患者,可应用锁定加压钢板联合植骨来治疗。Zhao等[22]从2011年1月至2012年12月应用锁定加压钢板结合植骨治疗12例胫骨骨不连患者,其中男8例,女4例;年龄20-69岁,平均47岁;从受伤到骨不连手术治疗时间为9个月到5年,平均19个月。所有患者术后4个月X射线均提示骨不连愈合迹象,3例患者术后6个月骨不连治愈,另外9例患者术后8-12个月治愈。"
外固定支架:支架外固定是胫骨骨折骨不连合并感染患者的首选固定方法。对于早期未接受内固定及无软组织损伤的Ⅱ,Ⅲ度开放性骨折患者,支架外固定术是最终的治疗方案。外固定架针脚有并发针眼窦道的可能,这可能与拆除或改动外固定支架有关,加强局部护理也许能够将这一并发症减小到最低。Ilizarov技术已被用于成角畸形愈合以及对位不良的骨折愈合的治疗。尽管频繁的术后随访以及针道问题的高发生率可能会使这项技术在非复杂性病例中的使用减少,但这种治疗方法仍然备受关注,此项技术对于合并软组织损伤的单纯成角骨折骨不连尤为有效。应用Ilizarov技术时应有周全的术前计划方案,而该方案被应用于患者时,也应由一名经验丰富熟悉这种技术的骨科医生主刀。Yu等[24]回顾性分析66例运用Ilizarov外固定支架治疗的感染性胫骨骨不连患者,其中男性患者62例,女性患者4例,平均年龄37.06岁;60例患者接受了术后18-46个月的随访,平均25.91个月,均获得了治愈,并且未发现感染复发。Yu等的研究结果显示应用Ilizarov技术治疗感染性的胫骨骨折骨不连在结构和功能上都取得了满意的疗效,而完全彻底的清创是控制感染的关键。Ilizarov技术对有较大缺损的感染性胫骨骨不连仍然有很好的疗效。Xu等[25]应用Ilizarov技术结合骨搬移技术治疗有较大缺损的感染性胫骨骨不连,取得了良好疗效。 2.2.3 加强胫骨骨折骨不连愈合的辅助治疗 骨移植:当胫骨骨折骨不连的机械问题被解决后,骨移植技术可用来解决骨不连的生物问题。骨形成是一个由骨发生、骨诱导以及骨传导构成的过程。自体骨移植通常从髂嵴取骨,它无病毒传播的风险,但取骨区的并发症问题仍然存在。关于植骨术治疗胫骨缺损方法的报道有很多。包括滑动嵌体移植,镶嵌移植,不带血管的腓骨移植,带血管蒂游离骨移植,以及一些其他的用于胫腓骨的技术。一系列的比较研究显示,皮质骨移植需要更长的时间才能达到骨愈合,并且它的相关并发症要多于松质骨移植[26]。松质骨移植替代治疗包括经皮注射骨髓,使用人骨形态发生蛋白,浓缩血小板以及人造骨移植。目前用于骨不连治疗的主要植骨材料有自体髂骨、同种异体骨和异种骨等。骨移植可结合各种固定技术来治疗不同类型的胫骨骨不连[15,18,25]。骨移植也可单独使用来治疗特殊的胫骨骨不连。Soldado等[27]报道了2例血管蒂的胫骨骨膜移植治疗儿童复杂性骨不连的病例,其中1例为骨缺损修复失败而导致的胫骨骨不连,患者是1个12岁的女孩;术后患者得到了快速的治愈。Soldado等[27]的临床研究证明,带血管蒂的胫骨骨膜移植可作为儿童复杂性胫骨骨不连的一种手术选择。Sugaya等[28]应用经皮自体红骨髓移植治疗胫骨骨折骨不连,获得了良好疗效。 电刺激:电刺激已被提倡作为一种非手术性方案用于骨折不愈合的治疗。相当多的实验室和临床证据表明,电刺激能够促进骨折愈合。尽管有一些证据表明应用电刺激后X射线显示延迟愈合的骨组织早期表现出愈合倾向,但其临床效应很难被证明[29]。 超声波治疗:超声波已被证实能够促进新鲜闭合性胫骨骨折的愈合,也可能对一些胫骨不连的治疗有效[30-31]。由于超声波尚未被证明对内固定治疗骨折有效,因而,它在胫骨骨折骨不连治疗中的作用地位可能会随之减小。 生物学辅助治疗:与其他现有的辅助治疗措施相比,骨形态发生蛋白在胫骨骨不连及骨延迟愈合的治疗中也许能发挥更加实质性的作用。一项关于122例胫骨骨不连病例的前瞻性随机对照研究证实重组人骨形态发生蛋白7可以促进骨不连的愈合[32]。重组人骨形态发生蛋白7已经被应用于临床,并取得了良好效果。Papanagiotou等[33]应用重组人骨形态发生蛋白7结合骨移植治疗长骨骨折骨不连,促进了80%患者的骨折愈合,提高了这些患者的生活质量。骨形态发生蛋白结合自体红骨髓有着广泛的来源,并且十分安全,是一种修复胫骨骨折骨不连的理想组合。Li等[34]从2004年1月至2010年12月对36例长骨骨折骨不连患者进行了骨形态发生蛋白化合物结合自体红骨髓移植的治疗,包括22例男性和14例女性,年龄22-68岁,平均36.8,其中13例为胫骨骨折;所有患者均得到了治愈,未出现免疫排斥反应及过敏反应。Li 等[34]的临床研究表明,骨形态发生蛋白化合物结合自体红骨髓能促进长骨骨折骨不连愈合。Ollivier等[35]不使用植骨材料,而是使用磷酸钙骨水泥结合重组人骨形态发生蛋白7对顽固性胫骨骨不连进行治疗,并证实这是一个安全有效的方法。"

| [1] 李崇鑫,常瑞龙,王国玉.胫骨骨折不愈合或延迟愈合的治疗进展[J].中国临床研究,2013,5(24):99-101.
[2] 吴作培,孙贵新.骨不连治疗的研究与技术应用进展[J].中国组织工程研究,2013,17(35):6333-6338.
[3] Yang JS, Otero J, McAndrew CM, et al.Can tibial nonunion be predicted at 3 months after intramedullary nailing? J Orthop Trauma.2013;27(11):599-603.
[4] LaVelle DG. Delayed union and nonunion of fractures. In: Canale TS editor. Campbell’s operative orthopaedics.9th ed.St.Louis: Mosby,1998: 2579-629.
[5] 郑金文,刘显东,王小兵, 等.下肢骨干骨折术后骨不连的原因分析及手术治疗[J].中国骨与关节损伤杂志, 2014, 29(12):1236-1238.
[6] 包岳丰,孙振中,顾三军,等. 四肢骨折内固定术后骨不连原因分析[J].中国骨与关节损伤杂志, 2013,28(10): 938-940.
[7] 裴丽霞.胫骨血供的临床解剖研究[J].现代预防医学, 2008, 35(9):1741-1744.
[8] Smith TK. Prevention of complications in orthopedic surgery secondary to nutritional depletion. Clin Orthop Relat Res. 1987;222:91-97.
[9] Pourfeizi HH,Tabriz A,Elmi A,et al. Prevalence of vitamin D deficiency and secondary hyperparathyroidism in nonunion of traumatic fractures. Acta Med Iran.2013;51(10):705-710.
[10] Lee JJ,Patel R,Biermann JS,et al.The musculoskeletal effects of cigarette smoking. J Bone Surg Am. 2013; 95(9):850-859.
[11] Kruppa CG,Hoffmann MF,Sietsema DL,et al.Outcomes After Intramedullary Nailing of Distal Tibial Fractures.J Orthop Trauma.2015;29(9):e309-315.
[12] Katsenis DL,Begkas D,Spiliopoulos G,et al.The results of closed intramedullary nailing for intra-articular distal tibial fractures.J Orthop Trauma.2014;28(2):108-113.
[13] Hernández-Vaquero D,Suárez-Vázquez A,Iglesias-Fernández S,et al.Dynamisation and early weight-bearing in tibial reamed intramedullary nailing:its safety and effect on fractureunion. Injury. 2012;43 Suppl 2:S63-67.
[14] 王志勇,王亚文. 带锁髓内钉加植骨治疗胫骨骨不连21例[J]. 临床骨科杂志,2012,15(1):69-70.
[15] Ding LZ,Xia NX.Pressure interlocking intramedullary nailing fixation and bone grafting for treatment of tibial fracture nonunion.Zhongguo Gu Shang.2012;25(4): 331-334.
[16] Phieffer LS, Goulet JA. Delayed unions of the tibia. J Bone Joint Surg. 2006;88(1):206-216.
[17] Muller ME. Treatment of nonunions by compression. Clin Orthop Relat Res. 1965;43:83-92.
[18] 纪红军,冯琼华.锁定加压钢板联合植骨治疗胫骨下段骨不连38例[J].临床骨科杂志,2011,14(6):718.
[19] 王子虎,尹芸生,李精敏,等.锁定加压钢板单骨皮质固定治疗长骨骨折髓内钉术后骨不连[J].中华创伤骨科杂志, 2009, 11(1):15-17.
[20] Ye J,Zheng Q.Augmentative locking compression plate fixation for the management of long bone nonunion after intramedullary nailing.Arch Orthop Trauma Surg. 2012;132(7):937-940.
[21] 章莹,朱昌荣,肖进,等.锁定加压钢板外置在胫骨感染性骨不连治疗中的应用[J].中华创伤骨科杂志,2013,15(7): 563-566.
[22] Zhao X,Wang PF,Zhang YT,et al.Advanced bone graft combined with locking compression plate for the treatment of middle and distal tibia nonunion. Zhongguo Gu Shang.2014;27(12): 1008-1011.
[23] 纪红军,冯琼华.锁定加压钢板联合植骨治疗胫骨下段骨不连38例[J].临床骨科杂志,2006,19(5):281-283.
[24] Yu P,Zhang Q,Mao Z,et al.The treatment of infected tibial nonunion by bone transport using the Ilizarov external fixator and a systematic review of infected tibial nonunion treated by Ilizarov methods.Acta Orthop Belg.2014;80(3):426-435.
[25] Xu K,Fu X,Li YM,et al.A treatment for large defects of the tibia caused by infected nonunion:Ilizarov method with bone segment extension.Ir J Med Sci.2014;183(3): 423-428.
[26] Holden CE.Bone-grafts in the treatment of delayed union of tibial shaft fractures.Injury.1972;4:175-179.
[27] Soldado F,Knörr J,Haddad S,et al. Vascularized tibial periosteal graft in complex cases of bone nonunion in children.Microsurgery. 2015;35(3):239-243.
[28] Sugaya H,Mishima H,Aoto K,et al. Percutaneous autologous concentrated bone marrow grafting in the treatment for nonunion.Eur J Orthop Surg Traumatol. 2014;24(5):671-678.
[29] 王占朝,侯树勋. 电刺激促进骨折愈合的研究现状[J].中国医刊,2005,40(7):51-53.
[30] Guerkov HH, Lohmann CH, Liu Y, et al. Pulsed electromagnetic fields increase growth factor release by nonunion cells. Clin Orthop Relat Res.2001;384: 265-279.
[31] Heckman JD, Ryaby JP, McCabe J, et al. Acceleration of tibial fracture-healing by non-invasive, low-intensity pulsed ultrasound. J Bone Joint Surg Am. 1994;76: 26-34.
[32] Friedlaender GE, Perry CR.Recombinant human bone morphogenetic protein-2 for treatment of open tibial fractures:a prospective,controlled,randomized study of four hundred and fifty patients. J Bone Joint Surg Am. 2002;84:2123-2134.
[33] Papanagiotou M,Dailiana ZH,Karachalios T,et al.RhBMP-7 for the treatment of nonunion of fractures of long bones.Bone Joint J.2015;97-B(7):997-1003.
[34] Li G,Liu Z.Treatment of long bone fracture nonunion in limbs by bone morphogenetic protein compounds combined withautologous red bone marrow graft. Zhongguo Gu Shang.2013;26(4):277-280.
[35] Ollivier M,Gay AM,Cerlier A,et al.Can we achieve bone healing using the diamond concept without bone grafting for recalcitrant tibial nonunions? Injury. 2015; 46(7):1383-1388. |
| [1] | Shi Bin, An Jing, Chen Long-gang, Zhang Nan, Tian Ye . Influencing factors for pain after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 993-997. |
| [2] | Wang Xian-xun. Impact of local compression cryotherapy combined with continuous passive motion on the early functional recovery after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 998-1003. |
| [3] | Yuan Wei, Zhao Hui, Ding Zhe-ru, Wu Yu-li, Wu Hai-shan, Qian Qi-rong. Association between psychological resilience and acute mental disorders after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1015-1019. |
| [4] | Chen Guang-dong, Cao Tong-jun, Li Jian. New bone fixation plate for the repair of avulsion fracture of the tibial attachment of the posterior cruciate ligament: study protocol for a prospective, open-label, self-controlled, clinical trial [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1020-1024. |
| [5] | Chen Qun-qun, Qiao Rong-qin, Duan Rui-qi, Hu Nian-hong, Li Zhao, Shao Min. Acu-Loc®2 volar distal radius bone plate system for repairing type C fracture of distal radius [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1025-1030. |
| [6] | Huang Xiang-wang, Liu Hong-zhe. A new low elastic modulus of beta titanium alloy Ti2448 spinal pedicle screw fixation affects thoracic stability: biomechanical analysis [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1031-1035. |
| [7] | Xie Qiang. Three-dimensional finite element model for biomechanical analysis of stress in knee inversion and external rotation after posterior cruciate ligament rupture [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1036-1040. |
| [8] | He Ze-dong, Zhao Jing, Chen Liang-yu, Li Ke, Weng Jie. Multilevel finite element analysis on the biological tribology damage of water on bone tissue [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1041-1045. |
| [9] | Li Jing, Yang Long, Wang Jian-ji, Liu Qin, Zou Qiang, Sun Yu, Ma Min-xian, Ye Chuan. Three-dimensional reconstruction based on DICOM data and its application for orthopedic implants [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1046-1051. |
| [10] | Jiang Zi-wei, Huang Feng, Cheng Si-yuan, Zheng Xiao-hui, Sun Shi-dong, Zhao Jing-tao, Cong Hai-chen,Sun Han-qiao, Dong Hang. Design and finite element analysis of digital splint [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1052-1056. |
| [11] | Wang Fei, Liu Zhi-bin, Tao Hui-ren, Zhang Jian-hua, Li Chang-hong, Cao Qiang, Zheng Jun, Liu Yan-xiong, Qu Xiao-peng. Clinical efficacy of preoperative osteotomy designs using paper-cut technology versus photoshop software for ankylosing spondylitis with kyphosis [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1057-1063. |
| [12] | Li Hui, Ma Jun-yi, Ma Yuan, Zhu Xu . Establishment of a three-dimensional finite element model of ankylosing spondylitis kyphosis [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1069-1073. |
| [13] | Ling Guan-han, Ou Zhi-xue, Yao Lan, Wen Li-chun, Wang Guo-xiang, Lin Heng-feng. Establishment of simulating three-dimensional model of China-Japan Friendship Hospital Classification for L type osteonecrosis of the femoral head [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1074-1079. |
| [14] | Fu Wei-min, Wang Ben-jie. Assessing the degree of necrotic femoral head, and association of blood supply with pathlogical changes: study protocol for a diagnostic animal trial [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1086-1091. |
| [15] | Zhang Wen-qiang, Ding Qian, Zhang Na. Associations between alpha angle and herniation pit on oblique axial magnetic resonance imaging in asymptomatic hip joints of adults [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1098-1103. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||