Chinese Journal of Tissue Engineering Research ›› 2014, Vol. 18 ›› Issue (4): 645-650.doi: 10.3969/j.issn.2095-4344.2014.04.026
Previous Articles Next Articles
Periprosthetic femoral fractures after total hip arthroplasty
Miao Shao-gang1, Lu Ning1, Yang Yang1, Chen Lei-jie1, Bassam A. Masri2
- 1Department of Orthopedics, the Second Affiliated Hospital of Kunming Medical University, Kunming 650101, Yunnan Province, China; 2Department of Orthopedics, University of British Columbia, Vancouver, Canada
-
Revised:2013-11-03Online:2014-01-22Published:2014-01-22 -
Contact:Yang Yang, Master’s supervisor, Department of Orthopedics, the Second Affiliated Hospital of Kunming Medical University, Kunming 650101, Yunnan Province, China -
About author:Miao Shao-gang, Studying for master’s degree, Department of Orthopedics, the Second Affiliated Hospital of Kunming Medical University, Kunming 650101, Yunnan Province, China
CLC Number:
Cite this article
Miao Shao-gang, Lu Ning, Yang Yang, Chen Lei-jie, Bassam A. Masri. Periprosthetic femoral fractures after total hip arthroplasty[J]. Chinese Journal of Tissue Engineering Research, 2014, 18(4): 645-650.
share this article

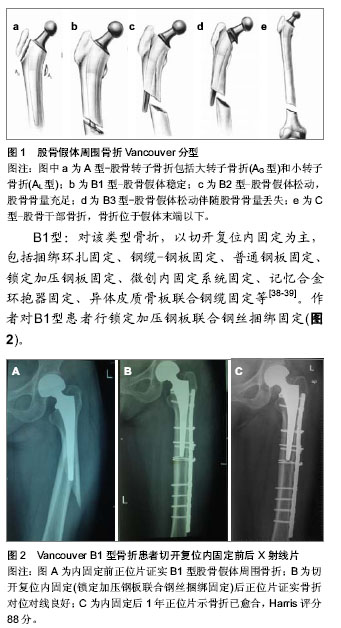
2.1 发病率 全髋关节置换一个潜在的严重并发症是股骨假体周围骨折,人工髋关节置换人数增多,人口老龄化和相应并发症如骨溶解和无菌性松动,翻修人数增多等因素,造成人工髋关节假体周围骨折的发生率正在增加[1-3]。所报道的发病率有所不同介于0.1%-2.1%[4]。Mayo临床关节置换数据库根据大宗病例报道,确定在初次髋关节置换中发生率为1%(238例/23 980例)和髋关节翻修(252例/6 349例)为4%[5]。在瑞典,股骨假体周围骨折已成为全髋关节翻修的第三大原因[3]。 2.2 危险因素 股骨假体周围骨折发病率与多种因素有关。目前公认的危险因素包括年龄、性别、创伤、固定方式、假体松动、翻修、骨溶解、术前疾病、骨质疏松、假体类型和手术技术等[5-6]。 年龄是股骨假体周围骨折的危险因素。老年人特别是女性,常伴有骨质疏松或内科疾病等,且行动迟缓、易摔倒,这些因素均增加了股骨假体周围骨折的风险[7]。Franklin等[8]研究报道,发生股骨假体周围骨折患者平均年龄为65.6岁,然而未发生骨折组为52.6岁。Lindahl等[9]通过对瑞典关节登记中心的资料分析,发现年龄每增加1岁,发生骨折的风险率即增加1.01。 股骨假体周围骨折患者以女性居多,报道显示占股骨假体周围骨折总数的52%-70%,因此很多学者认为女性是股骨假体周围骨折的一个危险因素,主要与绝经后雌激素减少造成骨质疏松有关[10]。瑞典关节登记中心的资料显示,年轻患者中男性和女性的比例基本相等,高龄(80岁以上)女性明显多于高龄男性[8]。骨质疏松是公认的危险因素。骨质疏松可降低骨的机械力,易导致低能量骨折。此外,绝大多数患者在全髋关节置换前均经长期非手术治疗,患者因疼痛而活动量少,已存在废用性骨质疏松。 创伤,尤其是占绝大多数的微小创伤,如摔倒、扭伤等是导致置换后股骨假体周围骨折最常见的原因。Lindahl等[11]报道术后发生股骨假体周围骨折75%由低能量创伤例如自站立或坐立高度跌倒所致。Beals等[12]报道,置换后发生股骨假体周围骨折66%是在室内摔倒所致,18%是在室外摔倒所致,8%为自发性骨折。高能量的创伤所造成的股骨假体周围骨折的病例<10%[13],多见于年轻人,主要与活动量大有关。 人工关节固定方式不同,发病率也有所差别。一般来说,生物型假体术中发病率较骨水泥高。为获得假体的早期稳定, 生物型固定需紧密压配,增加了发生股骨假体周围骨折的风险, 导致发病率升高[14]。Berry[15]回顾Mayo临床中心的资料,发现20 859例行全髋关节置换骨水泥固定者术中股骨假体周围骨折发病率为0.3%, 3 121例行生物型固定者发病率为5.4%。Tsiridis等[16]报道,全髋关节翻修采用骨水泥固定者术中股骨假体周围骨折发病率为6.3%,行生物型固定者为17.6%。 人工关节无菌性松动常由骨溶解所致,两者相互促进。无菌性松动常伴骨质吸收,松动的假体末端撞击外侧骨皮质,使局部应力增加,在轻微外力下即可造成骨折。骨溶解后假体的稳定性受到破坏,局部微动加剧。二者相互促进,进一步发展则可发生股骨假体周围骨折。 全髓关节翻修患者常有骨量不足,这可能导致假体固定困难,且取出假体及骨水泥困难时常需皮质开窗,从而会引起皮质损伤,降低股骨强度。翻修过程中髓腔准备不充分、骨水泥在髓腔内残留等均易导致骨折的发生。因此,翻修亦是股骨假体周围骨折的一大危险因素。Lewallen等[17]报道,初次全髋关节置换后股骨假体周围骨折发病率为0.4%-0.6%,而全髓关节翻修后高达1.5%-2.8%。 2.3 预防 目前全髋关节置换后股骨假体周围骨折发生率及复杂性均在增加,而且治疗股骨假体周围骨折手术创伤大,术后卧床时间长,出现假体松动,骨折延迟愈合及不愈合并发症的概率高,所以必须重视对股骨假体周围骨折的预防。 置换前:在进行全髋置换前需要对某些可能导致股骨假体周围骨折发生的因素进行分析,例如患者年龄、骨质质量、假体类型、假体固定方式等,任何降低骨强度的全身和局部因素均可引起术后股骨假体周围骨折,应引起重视。术前应拍摄双髋关节正位片,其中包括有股骨中上段侧位片,了解骨量情况、股骨中上段有无畸形,经测量后准确选择与之相匹配的假体[18-19]。 置换过程中:术中充分松解股骨周围软组织,切忌强行牵拉、扭转股骨近端。在行髋关节脱位时,可切断部分阔筋膜张肌、臀大肌止点和臀中肌后缘的紧张部,必要时大转子截骨。插入股骨的髓腔锉或髓腔钻,应靠向大转子,保持与股骨干平行,防止发生股骨皮质穿透骨折。打入髓腔锉、试模或假体遇到阻力时必须仔细检查,切忌强行锤入而引起股骨骨折。针对翻修术,在术中应仔细对骨水泥予以分离清理,切忌强力打出假体[20-21]。 置换后:置换后应指导患者进行正确的功能锻炼,避免摔伤。高龄是假体周围骨折的一大危险因素[8],所以对高龄,特别是合并有骨质疏松的患者,应考虑到骨折发生的可能性,故术后应正确地、科学地指导患者进行肌肉训练和关节活动度的训练,负重时应进行步态训练和协调性训练。Harris等[22]研究显示假体松动组比良好固定组发生骨折危险性大,因此临床上对未骨折而有假体松动和(或)骨溶解的高危人群的随访尤为重要,尽可能在骨折发生之前采取干预措施。Franklin[8]报道认为股骨假体周围骨折的关键预防措施为术后定期随访,常规进行影像学检查。 2.4 Vancouver分型 全髋关节置换后股骨假体周围骨折分型的目的是为了评估病情、选择正确的治疗方案及避免可能的并发症,主要有 Mayo分型、AAOS分型、Vancouver分型等。AAOS 分型方法[23]:Ⅰ型骨折位于转子间线的近端。Ⅱ型骨折垂直劈裂,但不超过小转子下缘。Ⅲ型骨折延伸至小转子下缘以下,但不超过假体柄的中下1/3交界处。Ⅳ型骨折位于假体柄末端处,Ⅳa螺旋型,Ⅳb横断型。Ⅴ型严重粉碎的Ⅲ型或Ⅳ型骨折,涉及假体柄远端以下。Ⅵ型骨折位于假体远端。目前普遍多采用Vancouver分型[24]。 Vancouver分型根据骨折位置、假体稳定性、骨量情况来确定[25](图1)。Vancouver分型把股骨分为3个解剖区域:A:转子部位,B:转子间以下至假体末端,C:假体末端远侧。 A型:A型分为AG型(大转子骨折)和AL型(小转子骨折)。 B型:B型根据股骨假体的稳定性及可利用的骨量分为B1型(股骨假体稳定)、B2(股骨假体松动,无明显股骨骨量丢失)、B3(股骨假体松动,股骨骨量丢失)。B2型与B3型的区别在B2型无明显骨量丢失。 C型:C型骨折位于假体远端,不影响假体稳定性。 Naqvi等[26]采用统计学方法分析此分型的有效性、可靠性。结果平均κ值为0.69(κ值为0.61-0.80为优良),显示针对全髋关节置换后股骨假体周围骨折的Vancouver分型,具有良好的有效性且可靠性、可重复性强。Masri等[27]也得出同样结果,平均κ值为0.77。 2.5 治疗 首先确定股骨假体周围骨折的分型:摄标准的双髋关节前后位片、假体侧的股骨全长正、侧位片。评价的内容包括:骨折位置、假体是否松动及骨量是否有丢失。对不同类型的骨折,应根据骨折的类型选择不同的治疗方法。另外患者年龄、性别、身体状况、经济情况等因素也是必须考虑的因素[28-29]。治疗目标是获得稳定的假体、促进骨折愈合、早期功能锻炼、恢复髋关节功能[30]。 Vancouver A型:该类型骨折的发生率约为4%[31]。骨折发生于股骨大转子或小转子,一般骨折移位小且假体稳定,多采用非手术治疗。AG型骨折通常是稳定的,患者可以行外展位卧床牵引、避免负重、限制活动6-12周等保守治疗[32]。Pritchett[33]报道移位少于2 cm的大转子骨折采用该方法得以愈合。当大转子移位超过2.5 cm或不愈合导致疼痛、不稳定或外展肌乏力时要考虑内固定。AL骨折较少见,一般较轻微,如果骨折累及较大的股骨距,使内侧壁缺少支撑影响假体的稳定,则需要内固定,如钢丝、钢缆环扎、特殊钢板固定等[34]。Mont等[35]通过对26篇文献487例病例进行分析,证明稳定的A型骨折应用保守治疗预后良好。 Vancouver B型:B型为临床最常见类型,发生率为80%,保守治疗有很高并发症,Lindahl等[11]统计采用非手术治疗的假体松动翻修率达19%-100%,骨折不愈合率25%-42%,畸形愈合率达45%。因此,学者建议早期根据骨折的部位、假体的稳定性和骨质量,选择恰当的治疗方式,是治疗股骨假体周围骨折Vancouver B型的关键[36-37]。"

B2型:该类型骨折治疗重点在于首先恢复假体的稳定性,其次是骨折坚强内固定,因此股骨假体翻修是手术治疗关键。目前常规用加长柄进行翻修治疗,推荐使用广泛涂层生物型加长柄假体,不仅提供了骨折断端之间的髓内连接,增加髓内稳定性,同时远端骨长入的生物学固定模式为假体以及骨组织提供了长期稳定性[40]。Springer等[41]认为广泛涂层非骨水泥假体在术后生存率、稳定性和骨折的不愈合发生率等临床指标上均优于近端涂层假体及骨水泥假体。预期寿命有限的高龄患者,尤其伴有明显骨折疏松者,可选用长柄骨水泥假体联合钢缆、钢板、异体皮质骨板植骨等治疗B2型骨折,争取早期骨折愈合、尽早下地负重行走、恢复髋关节功能。Corten等[42]最近报道对31例平均年龄为82岁的B2型骨折患者采用骨水泥柄翻修,8例患者在骨折愈合前(翻修后6个月)死亡,16例患者生存期超过1年。33个月随访中,患者翻修后早期在助行器帮助下完全负重行走并未感觉疼痛,髋关节功能恢复良好,翻修后1年Harris评分平均77.5分,无再次翻修或者影像学提示假体松动征象的病例。作者对B2型患者也应用长柄骨水泥假体翻修,随访效果良好(图3)。 B3型:B3型骨折多发生于全髋关节置换后晚期,假体柄松动且柄周围或股骨近端出现较广泛的溶骨性骨缺损,治疗难点在于骨量严重缺失下既要恢复假体的稳定性,又要达到骨折断端间的牢固固定[43]。 股骨骨量的重建是治疗关键,这类骨折的骨皮质变薄、硬化,不易使用骨水泥型假体,非骨水泥长柄翻修假体结合同种异体皮质骨板移植是目前常用的方法。Howell等[44]研究发现钢缆钢板结合异体皮质骨板植骨治疗股骨假体周围骨折的效果明显优于单独使用这2种方法,其固定强度随钢缆的数量增多而增加,同时指出术中应注意对股骨骨膜的保护以降低骨折不愈合率。Maury等[45]报道采用部分结构植骨和近端股骨置换治疗B3型骨折,Young等[46]报道采用远端带内锁钉的长柄股骨假体治疗B3型骨折,都取得良好效果。 Masri教授提供了1例B3型骨折患者的X射线附于该文稿(The professor Masri offers the X-rays of Vancouver B3 fracture) (图3)。"


Vancouver C型:C型骨折位于假体远端,不影响假体稳定性,可以单独处理,骨折近端仍有足够距离使用螺钉固定,常规行切开复位内固定,常用方法包括普通钢板、LISS钢板、股骨髁钢板等。 2.6 随访结果 Mukundan等[47]最近报道72例股骨假体周围骨折患者治疗后平均随访2年的情况,79%为优良,21%发生骨不连、松动、脱位或感染等并发症而再次手术。Bryant等[48]报道19例股骨假体周围B1型骨折患者采用切开复位内固定,内固定后平均随访17周(12-27周),全部都获得愈合,没有发生需要行翻修手术的严重并发症。Agarwal等[49]报道16例B1型骨折治疗后至少随访1年的情况,2例发生深部感染,1例骨折不愈合,1例髋部术后持续疼痛,其余12例都恢复良好、获得愈合。Rayan等[50]报道26例B2型和B3型骨折,所有患者使用生物型柄翻修、异体皮质骨板、钢板-钛缆系统、骨移植等治疗,所有骨折的在临床和影像学上都证实愈合,治疗后Harris 评分平均为83.04分。"

| [1] Duwelius PJ, Schmidt AH, Kyle RF,et al. A prospective, modernized treatment protocol for periprosthetic femur fractures. Clin Orthop North Am. 2004;35(4):485-492.[2] Lindahl H. Epidemiology of periprosthetic femur fracture around a total hip arthroplasty. Injury. 2007;38(6): 651-654.[3] Lindahl H, Garellick G, Regner H, et al. Three hundred and twenty-one periprosthetic femoral fractures. J Bone Joint Surg Am. 2006;88(6): 1215-1222.[4] Masri BA, Meek RM, Duncan CP. Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res. 2004;420: 80-95.[5] Masri BA, Duncan CP, O’Brien PJ, et al. Principles of Treatment for Periprosthetic Femoral Shaft Fractures Around Well-fixed Total Hip Arthroplasty. J Am Acad Orthop Surg. 2009;17(11):677-688.[6] 张纪,周一新,周乙雄. 髋关节置换术中股骨假体周围骨折危险因素的分析[J].中华关节外科杂志:电子版,2010,4(4):488-493.[7] 陈炜平,王祥华.股骨假体周围骨折的危险因素[J].国际骨科学杂志,2008,29(1):16-18.[8] Franklin J. Malchau H. Risk factors for periprosthetic femoral fracture. Injury. 2007;38(6):655-660.[9] Lindahl H, Eisler T, Oden A, et al. Risk factors associated with the late periprosthetic femoral fracture. In: Lindahl H,editor. The periprosthetic femur fracture: a study from the Swedish National Hip Arthroplasty Register. Goteberg:Goteberg University, 2006:16-19.[10] 张占岭,陈长安.全髋关节置换术后并发假体周围骨折相关因素分析[J].现代预防医学,2012,39(15):3961-3963.[11] Lindahl H, Malchau H, Herberts P, et al. Periprosthetic femoral fractures: classifi¬cation and demographics of 1049 periprosthetic femoral fractures from the Swedish National Hip Arthroplasty Rosier. J Arthroplasty. 2005;20(7):857-865.[12] Beals RK, Tower SS. Periprosthetic fractures of the femur. An analysis of 93 fractures.Clin Othop. 1996;327:238-246.[13] Cooke PH, Newman JH. Fractures of the femur in relation to cemented hip prostheses. J Bone Joint Surg Br. 1988;70(3): 386-389.[14] 熊高鑫,黄彰,江华.人工髋关节置换术中股骨假体周围骨折影响因素及相关分析[J].实用医学杂志,2012,28(9):1504-1506.[15] Berry DJ. Epidemiology: hip and knee. Clin Orthop North Am. 1999;30(2):183-189.[16] Tsiridis E, Haddad FS, Gie GA. The management of periprosthelic femoral fractures around hip replacements. Injury. 2003;34(2):95-105.[17] Lewallen DG, Berry DJ. Periprosthetic fracture of the femur after total hip arthroplasty: treatment and results to date. Instr Course Lect. 1998;47:243-249.[18] 唐广满,孔建中.全髋置换术后股骨侧假体周围骨折的手术治疗进展[J].创伤外科杂志,2011,13(4):364-367.[19] 周印.人工髋关节置换术中发生假体周围骨折的原因及防治措施[J].中国医药指南,2012,10(36):134-135.[20] 黄峰,陈允震.股骨粗隆间骨折的治疗进展[J].中国骨与关节损伤杂志,2009,24(6):570-572.[21] 万仑,刘仲前,吕波.人工髋关节置换术并发股骨假体周围骨折的治疗[J].四川医学,2009,30(8):259-1260.[22] Harris B, Owen JR, Wayne JS, et al. Does femoral component loosening predispose to femoral fracture? Clin Orthop. 2010;468(2):497-503.[23] 郑东.人工髋关节置换后股骨假体周围骨折[J].中国组织工程研究,2012,16(30):5662-5669.[24] Ninan TM, Costa ML, Krikler SJ. Classification of femoral periprosthetic fractures.Injury. 2007;38(6):661-668.[25] Brady OH, Masri BA, Duncan CP, et al. Classification of the hip. Clin Orthop North Am. 1999;30(2):215-220.[26] Naqvi GA, Baig SA, Awan N, et al. Interobserver and intraobserver reliability and validity of the Vancouver classification system of periprosthetic femoral fractures after hip arthroplasty.J Arthroplasty. 2012;27(6):1047-1050.[27] Brady OH, Garbuz DS, Masri BA, et al. The reliability and validity of the Vancouver classification of femoral fractures after hip replacement. J Arthroplasty. 2000;15(1):59-62 .[28] 赵建宁,周利武,郭亭, 等.股骨假体周围骨折的治疗[J].中国创伤杂志,2004,20(11):660-663.[29] 杨波,吴杰,喻飞,等.人工髋关节置换术后股骨假体周围骨折的治疗体会[J].中国骨与关节外科,2011,4(2):110-113. [30] Berry DJ. Management of periprosthetic fractures: the hip. J Arthro plasty. 2002;17(4):11-13.[31] Duncan CP,Masri BA. The role of antibiotic - loaded cement in the treatment of an infection after a hip replacement. Instr Course Lect. 1995;44:305-313.[32] 丛锐军,刘伟,李晓华, 等.全髋置换术后股骨假体周围骨折的治疗[J].中国骨与关节外科,2009,2(6):435-437.[33] Pritchett JW. Fractures of the greater trochanter after hip replacement. Clin Orthop. 2001;390:221 -226.[34] 张炅,王毅,杨庆铭,等.股骨假体周围骨折手术治疗策略[J]. 中华关节外科杂志:电子版,2009,3(5):558-564.[35] Mont MA,Maar DC. Fractures of the ipsilateral femur after hip ar¬throplasty. A statistic alanalysis of outeome based on 487 patients. J Arthroplasty. 1994;9(5):511 -519.[36] 李展春,臧危平,程光齐,等. Vancouver B型股骨假体周围骨折的手术治疗分析[J].实用骨科杂志,2011,17(6):516-518.[37] 司刚,蒋建农,王勇,等. Vancouver B型股骨假体周围骨折的治疗[J].中国骨与关节损伤杂志,2010,25(12):1106-1108.[38] 汤冀强. Vancouver B1型股骨假体周围骨折的手术治疗[J].实用骨科杂志,2011,17(12):1111-1113.[39] 胡忠伟,何伟涛,项叶丹,等. AO锁定钢板结合线缆系统微创内固定治疗Vancouver B1型股骨假体周围骨折[J]. 中国骨与关节损伤杂志,2013,28(2):150-151.[40] 丛宇,赵建宁.全髋关节置换术中假体周围骨折的研究进展[J]. 中国骨伤,2011,24(2):178-181.[41] Springer BD,Berry DJ,Lewallen DG, et al. Treatment of periprosthetic femoral fractures following total hip arthroplasty with femoral component revision. J Bone Joint Surg Am. 2003; 85(11):2156 -2162.[42] Corten K, Macdonald SJ, McCalden RW, et al. Results of cemented femoral revisions for periprosthetic femoral fractures in the elderly. J Arthroplasty. 2012;27(2):220-225 .[43] 胡金艮,林向进.全髓关节置换术后股骨假体周围骨折治疗进展[J].国际骨科学杂志,2010,31(4):227 -228.[44] Howell JR, Masri BA, Garbuz DS, et al. Cable plate and onlay allgraft in periprosthetic femoral fractures after hip replacement:laboratory and clinical observation. Instr Course Letc. 2004;53:99-110.[45] Maury AC,Pressman A,Cayen B, et al. Proximal femoral allogrart treatment of Vancouver type- B3 periprosthetic femoral fracture after total arthroplasty. J Bone Jiont Surg Am. 2006;88(5):953-958.[46] Young SW,Pandit S, Munro JT,et al. Periprosthetic femoral fracture after total arthroplasty. ANZJ Surg. 2007;77(6): 424-428.[47] Mukundan C, Rayan F, Kheir E, et al. Management of late periprosthetic femur fractures: a retrospective cohort of 72 patients. Orthop Int. 2010;34(4):485-489.[48] Bryant GK, Morshed S, Agel J, et al. Isolated locked compression plating for Vancouver Type B1 periprosthetic femoral fractures. Injury. 2009,40(11):1180-1186.[49] Agarwal S, Andrews CM, Bakeer GM. Outcome Following Stabilization of Type B1 Periprosthetic Femoral Fractures. J Arthroplasty. 2005;20(1):118-121.[50] Rayan F, Konan S, Haddad FS.Uncemented revision hip arthroplasty in B2 and B3 periprosthetic femoral fractures-A prospective analysis. Hip Int. 2010;20(1):38-42. |
| [1] | Wei Wei, Li Jian, Huang Linhai, Lan Mindong, Lu Xianwei, Huang Shaodong. Factors affecting fall fear in the first movement of elderly patients after total knee or hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1351-1355. |
| [2] | Wang Jinjun, Deng Zengfa, Liu Kang, He Zhiyong, Yu Xinping, Liang Jianji, Li Chen, Guo Zhouyang. Hemostatic effect and safety of intravenous drip of tranexamic acid combined with topical application of cocktail containing tranexamic acid in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1356-1361. |
| [3] | Xiao Guoqing, Liu Xuanze, Yan Yuhao, Zhong Xihong. Influencing factors of knee flexion limitation after total knee arthroplasty with posterior stabilized prostheses [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1362-1367. |
| [4] | Huang Zexiao, Yang Mei, Lin Shiwei, He Heyu. Correlation between the level of serum n-3 polyunsaturated fatty acids and quadriceps weakness in the early stage after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1375-1380. |
| [5] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [6] | Chen Xinmin, Li Wenbiao, Xiong Kaikai, Xiong Xiaoyan, Zheng Liqin, Li Musheng, Zheng Yongze, Lin Ziling. Type A3.3 femoral intertrochanteric fracture with augmented proximal femoral nail anti-rotation in the elderly: finite element analysis of the optimal amount of bone cement [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1404-1409. |
| [7] | Du Xiupeng, Yang Zhaohui. Effect of degree of initial deformity of impacted femoral neck fractures under 65 years of age on femoral neck shortening [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1410-1416. |
| [8] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [9] | Cai Qunbin, Zou Xia, Hu Jiantao, Chen Xinmin, Zheng Liqin, Huang Peizhen, Lin Ziling, Jiang Ziwei. Relationship between tip-apex distance and stability of intertrochanteric femoral fractures with proximal femoral anti-rotation nail: a finite element analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 831-836. |
| [10] | Zhao Zhongyi, Li Yongzhen, Chen Feng, Ji Aiyu. Comparison of total knee arthroplasty and unicompartmental knee arthroplasty in treatment of traumatic osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 854-859. |
| [11] | Liu Shaohua, Zhou Guanming, Chen Xicong, Xiao Keming, Cai Jian, Liu Xiaofang. Influence of anterior cruciate ligament defect on the mid-term outcome of fixed-bearing unicompartmental knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 860-865. |
| [12] | Zhang Nianjun, Chen Ru. Analgesic effect of cocktail therapy combined with femoral nerve block on total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 866-872. |
| [13] | Yuan Jun, Yang Jiafu. Hemostatic effect of topical tranexamic acid infiltration in cementless total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 873-877. |
| [14] | Liu Lihua, Sun Wei, Wang Yunting, Gao Fuqiang, Cheng Liming, Li Zirong, Wang Jiangning. Type L1 steroid-induced osteonecrosis of the femoral head through femoral head and neck junction decompression by fenestration: a single-center prospective clinical study [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 906-911. |
| [15] | Li Yan, Wang Pei, Deng Donghuan, Yan Wei, Li Lei, Jiang Hongjiang. Electroacupuncture for pain control after total knee arthroplasty: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 957-963. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||