Chinese Journal of Tissue Engineering Research ›› 2013, Vol. 17 ›› Issue (44): 7791-7796.doi: 10.3969/j.issn.2095-4344.2013.44.022
Previous Articles Next Articles
Research and application of urethral sling placement on neurogenic incontinence
Ding Liu-cheng, Huang Yi, Wei Zhong-qing
- the Second Affiliated Hospital of Nanjing Medical University, Nanjing 210000, Jiangsu Province, China
-
Online:2013-10-29Published:2013-10-31 -
Contact:Wei Zhong-qing, M.D., Chief physician, Professor, the Second Affiliated Hospital of Nanjing Medical University, Nanjing 210000, Jiangsu Province, China weizq1@163.com -
About author:Ding Liu-cheng★, Master, Physician, the Second Affiliated Hospital of Nanjing Medical University, Nanjing 210000, Jiangsu Province, China lancet110@gmail.com -
Supported by:National Natural Science Foundation of China, No. 81300572*; Natural Science Foundation of Jiangsu Province, No. SBK201123829*
CLC Number:
Cite this article
Ding Liu-cheng, Huang Yi, Wei Zhong-qing . Research and application of urethral sling placement on neurogenic incontinence[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(44): 7791-7796.
share this article
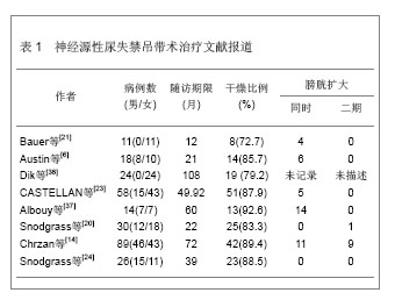
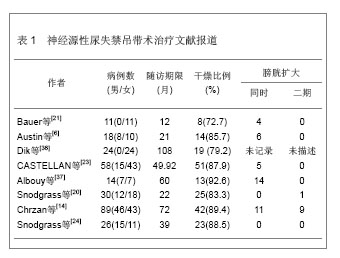
2.1 尿道吊带材料 理想的吊带材料应该具备如下特性:组织相容性好,异物反应小,容易缝合,抗感染效果好,无致癌性,无机械张力[5]。目前吊带材料主要包括自体与异体移植物,自体移植物主要是大腿阔筋膜、腹直肌筋膜、阴道壁组织等;异体移植物如牛阔筋膜、猪小肠黏膜下组织等。近20年合成材料也逐渐得到发展,如聚丙烯聚乙烯吊带在成人无张力吊带手术中得到广泛应用,为尿失禁材料提供了更多的治疗选择[6-7]。 2.2 尿道吊带置入治疗适应证 尿道吊带悬吊置入该疗法理想的适应证是膀胱出口关闭不全的女性患者,同时,留有足够长的尿道长度,行间歇导尿而膀胱状态良好。其中,特别是尿道固有括约肌功能不全的Ⅲ型压力性尿失禁, 更加适合此类手术。一般来说,膀胱尿道造影提示膀胱颈口明显张开,同时尿动力学检查测得(腹压漏尿点压)VLPP小于2.94 kPa的情况下,建议行改善膀胱出口关闭状况的手术。 2.3 尿动力学对患者尿道吊带置入治疗的选择 清楚理解尿失禁症状产生的病理生理机制是制定治疗方法的基础,从功能上判断尿失禁症状是由于膀胱功能异常(反射亢进,顺应性降低,小容量)还是括约肌功能异常导致引起抑或是两者皆有。神经源性膀胱尿道功能障碍的患者通常伴随着膀胱功能异常,因此,术前影像尿动力学评估膀胱顺应性、容量、逼尿肌不稳定收缩对于神经源性尿失禁诊断治疗具有重要的意义[8]。McGuire[9]认为影像尿动力学过程中,腹压漏尿点压(又称为Valsalva漏尿点压)对于评估膀胱颈口的关闭及置入治疗选择上具有重要的意义。各种各样置入治疗方式的前提必须保证低压储尿及保护上尿路功能,避免泌尿系统的损害是基本原则,尿道阻力和膀胱顺应性是重要的参考指标。 在术前,根据患者病情,还应该根据影像尿动力学的评估结果,考虑是否决定行膀胱出口关闭加自体膀胱扩大。某些神经源性膀胱患者尽管膀胱出口阻力低,但用膀胱扩大就能治愈尿失禁,尤其是男性患儿,随着前列腺的发育,膀胱出口关闭功能逐渐改善。另一方面,治疗前行尿动力学评估的同时,若用一定的方法使膀胱出口闭合后,检查结果提示膀胱稳定,容量和顺应性良好,则用吊带提供膀胱颈部支撑足以终止漏尿,两种治疗是否同时进行,还是先做一种仍然还有争议[4,10-11]。Decter[12]发现两种治疗同时进行的患者与单纯行膀胱颈悬吊而未作膀胱扩大的患者治疗后漏尿率明显提高,但这也可能导致了一部分患者做不必要的膀胱扩大[13]。Chrzan等[14]认为患者治疗前膀胱容量为正常70%时的膀胱压< 1.96 kPa可进行吊带悬吊。神经源性膀胱尿失禁患者的尿道压大于2.45-2.94 kPa时,仅行膀胱扩大术似乎已足以保证患者的控尿功能[15]。Perez等[16]复习文献及自身经验发现约70%神经源性尿失禁患者同时行膀胱扩大术及吊带术,并认为尿道压在1.96-3.92 kPa可以考虑进一步行膀胱扩大术。目前对于膀胱颈悬吊术同时行膀胱扩大术的适应证仍然充满争议,作者建议合并有逼尿肌不稳定收缩、膀胱容量减少同时伴随着压力性尿失禁的患者可考虑同时行膀胱扩大术。 2.4 尿道吊带置入方式 2.4.1 膀胱颈筋膜吊带 治疗方式常用长6-10 cm 宽1.5-2.0 cm腹直肌筋膜做吊带,也可选用阔筋膜,但与自体筋膜相比感染和侵蚀的可能性明显增加。膀胱颈悬吊前,患者尿培养必须为阴性,围手术期间应用广谱抗生素。采用阴道前壁正中纵形或弧形切口,切口起自尿道外口近端1.5 cm处延长至膀胱颈近端1 cm处,膀胱颈位置可借助导尿管球囊来判断,将阴道黏膜从其下方的尿道周围筋膜分离开,显露膀胱尿道交界 [12, 17-18]。目前,对于神经源性膀胱伴随尿失禁的患者,这是一种十分有效的手术方式[19]。 吊带置入的方式:吊带置入的方式主要是围绕膀胱颈和近端尿道以U/X形式,360°环包[20],张力以松弛[6]、适中[21]、紧张[20],也有仅仅单纯依靠膀胱逼尿肌漏尿点压增加0.98-1.47 kPa判断手术成效,而并不管吊带置入的形式[19, 22-23]。理论上膀胱颈环包法比悬吊法更容易进行导尿,因为环绕的力量可以 相对均匀地围绕膀胱颈分布,避免了尿道的折曲,不会引起尿道侵蚀。通过吊带悬吊可以提高尿道闭合能力,同时环绕尿道吊带悬吊可以均匀的压迫在膀胱颈周围,并能够有效的提高尿道闭合能力,从而保证患者的控尿。Snodgrass等[24] 采用腹直肌筋膜环绕膀胱颈的环包,然后用聚丙烯缝线将筋膜固定在耻骨膜上,膀胱顶部固定在腹直肌右侧近脐部,这样增加了逼尿肌漏尿点压,约增加了1.176 kPa,虽达到了控尿的目的,但可能继发引起上尿路的损害。 筋膜吊带张力的控制:为了获得理想的吊带张力,对于进行间歇导尿的神经源性膀胱患者,不用担心尿潴留,但应该避免吊带过紧,张力过大会引起尿道侵蚀和尿道萎缩。Decter[12]建议,对于男性神经源性尿失禁患者,由于前列腺两侧叶的存在,为了达到理想的抬高和压迫尿道的目的,缝合张力需比女性患者的大。对于吊带张力的控制,术中常根据尿道压测定与增加腹压观察尿道漏尿情况来判断,即在保持膀胱适当容量的基础上,提高逆行最大尿道压0.98-1.47 kPa,咳嗽时尿液从尿道外口溢出一两滴尿作为悬带张力适度的指标[2]。 2.4.2 经闭孔无张力尿道中段悬吊 经闭孔无张力尿道中段悬吊术为瑞典妇产科医师Ulmsten设计,使90%患者尿失禁症状显著改善,治愈率和有效率高、并发症少、治疗简单而微创[25],目前,已经成为治疗单纯性女性压力性尿失禁的黄金标准[26]。经闭孔无张力尿道中段悬吊的原理是利用无组织反应的Prolene聚丙稀网带,轻巧地支撑尿道中段及球海绵体肌,使其回复到正常位置且无张力,从而修复和加强盆底筋膜、阴道尿道悬筋膜及尿道旁结缔组织。在身体静止时,这支撑带并不会产生任何张力,但是在运动及压力下,它便可以提供有效的尿道闭锁功能。Hamid 等[27]予以压力性尿失禁合并神经源性膀胱的患者经阴道无张力尿道中段悬吊,悬吊张力确定:以咳嗽时尿液从尿道外口溢出一两滴尿作为悬带张力适度的指标,后来又将通过控制32Ch Hegar可置入于吊带与阴道之间作为判定标准。 2.4.3 男性耻骨后骨锚尿道悬吊 治疗方式同前列腺摘除术后患者类似,治疗前予以广谱抗生素,取过度截石位,留置尿管以手指可以触及尿道,取会阴部3 cm正中切口,仔细分离浅层软组织至球海绵体肌及尿道,侧面分离至近耻骨下支内上侧,固定骨螺钉,将一侧耻骨下支上的3条合成线穿过吊网两角分别结扎固定,并固定于耻骨下支,并采用prolene骨缝线穿过裁剪好的补片打结,然后以适宜的松紧度固定另一端吊带,使膀胱颈的悬吊满意,悬吊结束后均匀平坦舒展补片,缝合关闭,留置导尿管[28]。悬吊张力确定:逆向漏尿点压,以咳嗽动作和逆行膀胱灌注来检测悬吊张力,标记悬吊材料帮助缝合固定,逆行灌注括约肌测压尿管置于海绵体部尿道球部尿道水平定为零点,缓慢升高灌水袋,目标:5.88-6.37 kPa [29-30],国内何恢绪通过逆行最大尿道压测定与增加腹压观察尿道漏尿情况判断,即在保持膀胱适当容量的基础上,提高逆行最大尿道压为0.981-1.47 kPa,咳嗽时尿液从尿道外口溢出一两滴尿作为悬带张力适度的指标[31]。 2.5 尿道吊带置入效果和并发症 治疗后尿失禁判定以24 h尿垫使用量为依据,在三四小时内清洁间歇导尿,1 d内尿垫使用数量作为判断治疗成功的标准。多数研究显示控尿率大于80%,其中更多选择的是女性患者,一些研究者显示女性控尿率85%明显高于男性的69%。Kurzrock等[32]认为性别间吊带治疗效果差异可能与男性前列腺存在有关,其导致关闭和抬高近端尿道更困难。Decter[12]报道悬吊过紧容易导致尿道侵蚀,一旦出现即需要移除吊带。Dave等[33]认为膀胱出口关闭不全患者吊带置入后,膀胱扩大术势在必行,并且认为如果不行膀胱扩大,治疗后膀胱功能恶化是不可避免的。但Snodgrass等[24]通过将尿道吊带置入同时行膀胱扩大和单纯sling悬吊两种方式观察治疗后尿失禁控制率的差异,治疗后尿失禁控制率未见明显差异,但同时行吊带及自体筋膜悬吊的患者留置尿管时间延长,抗胆碱能药物量明显降低,两组患者生活独立、社会交际方面明显提高[34],并通过尿动力学方法观察逼尿肌顺应性改变,39个月随访发现膀胱功能稳定,膀胱颈悬吊未行膀胱扩大患者治疗后长期随访发现患者膀胱顺应性良好,治疗后1年的膀胱逼尿肌的不稳定收缩的程度提示仅需要服用抗胆碱能药物而不是行膀胱扩大术,这点与Austin研究一致[24, 35]。神经源性尿失禁吊带治疗文献报道见表1。"

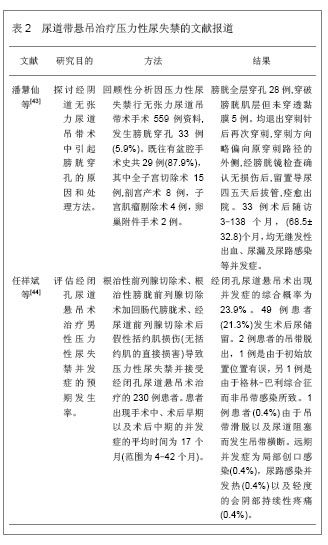
Hamid等[27]报道经闭孔无张力尿道中段悬吊治疗在女性压力性尿失禁合并神经源性膀胱的患者的使用,通过长达10年的随访发现中段尿道悬吊治疗手术简单有效,创伤小,尿失禁控制率高[38]。Xu 等[39]报道经闭孔无张力尿道中段悬吊在轻中度男性尿失禁患者的应用,可以提供有效的尿道闭锁功能,但重度尿失禁患者不建议使用。 治疗中、治疗后并发症Abouassaly报道并发尿潴留6.2%,膀胱穿孔5.8%,阴道出血及后腹膜血肿1.90%,感染0.4%,治疗中出血2.5%[40]。如果,术后出现长期的尿痛、漏尿、反复的感染和排尿困难时,应该警惕是否存在未发现的膀胱损伤[41],甚至还会引起坏死性感染,为临床治疗带来巨大困扰[42]。 文献报道见表2。 Madjar, Jacoby首次报道前列腺术后男性耻骨后骨锚尿道悬吊治疗尿失禁发现控尿成功率: 87.5% (0-1 pads) [45],Daneshmand及何恢绪使用该技术治疗神经源性膀胱,通过36个月的随访发现,患者控尿率达83%,且没有严重的并发症,同时此类手术也并没有明显的学习曲线[46],提示成年男性神经源性尿失禁予以耻骨前列腺尿道吊带悬吊术是治疗神经元尿道括约肌功能低下的有效安全的选择[17],但需要注意的是耻骨后骨锚尿道悬吊带与人工尿道括约肌360°环形压迫尿道不同。仅压迫尿道球部腹侧,保留尿道背面及两侧血运不受干扰。球海绵体肌像一个缓冲垫衬在尿道与悬带之间,减少尿道糜烂坏死的危险,但聚丙烯悬带与自体或尸体筋膜不同,不可吸收,也不能伸展或沿尿道纵向撕裂,形成对尿道腹侧的持续压迫,用于儿童神经源性括约功能障碍性尿失禁,随着患儿生长发育,固定的人工悬带是否会不适应机体发育而导致对尿道压力的改变,甚至出现并发症?目前多用于轻中度尿失禁患者,重度尿失禁患者多考虑行人工尿道括约肌扩张或重建,因此必须从严掌握治疗指征,治疗中按照低压有效原则调整悬带张力,治疗后严密长期随访,对自觉症状,上尿路功能、形态,排尿情况,膀胱容量,膀胱剩余尿等进行动态监测,必要时配合间歇清洁导尿。 结论:膀胱颈腹直肌筋膜吊带是重建外科的一种有价值的补充,由于不需要外来材料,使他成为多种膀胱出口关闭不全患者的引人瞩目的选择,但长期疗效不清楚,目前对于膀胱颈悬吊是否需要同时行膀胱扩大目前尚没有定论,需要前瞻性多中心的循证医学研究证实。尽管聚丙烯、聚乙烯人工合成吊带(经阴道无张力尿道中段悬吊骨锚尿道悬吊)在治疗压力性尿失禁及前列腺术后尿失禁患者中广泛应用[47],但此方法在神经源性尿失禁的疗效还有待于后续应用证实。 "
| [1]McGuire, EJ, Wang, CC, Usitalo H,et al.Modified pubovaginal sling in girls with myelodysplasia. J Urol.1986;135:94. [2]Venn SN, Greenwell TJ, Mundy AR.The long-term outcome of artificial urinary sphincters. J Urol. 2000;164: 702. [3]Simeoni J, Guys JM, Mollard P, et al. Artificial urinary sphincter implantation for neurogenic bladder: a multi-institutional study in 107 children. Br J Urol. 1996;78: 287. [4]Kryger JV, Gonzalez R, Banhold JS.Surgical management of urinary incontinence in children with neurogenic sphincteric incompetence.J Urol.2000;163: 256-263. [5]Cosson M,Debodinance P,Boukerrou M,et al.Mechanical properties of synthetic implants used in the repair of prolapse and urinary incontinence in women: which is the ideal material? IntUrogynecol J Pelvic Floor Dysfunct. 2003; 14:169-178 [6]Austin PF, Westney OL, Leng WW,et al. Advantages of rectus fascial slings for urinary incontinence in children with neuropathic bladder.J Urol. 2001;165:2369-2372. [7]Godbole P, Mackinnon AE.Expended PTFE bladder neck slings for incontinence in children: the long-term outcome. BJU Int.2004;93:139-141. [8]Woodside JR, Borden TA.Pubovaginal sling procedure for the management of urinary incontinence in a myelodysplastic girl. J Urol. 1982;127: 744. [9]MeGuire EJ.Editorial comment. J Urol.1989;142: 301. [10]Clemens JQ,Bushman W,Schaeffer AJ.Questionnaire based results of the bulbourethral sling procedure. J Urol.1999; 162: 1972-1976. [11]Comtter CV. The male sling for stress urinary incontinence: a prospective study. J Urol.2002;167; 597-601. [12]Decter RM. use of the fascial sling for neurogenic incontinence:lesson learned. J Urol.1993; 150; 683-686. [13]Kreder KJ, Webster G.Management of the bladder outlet in patients requiring enterocystoplasty. J Urol.1992;147; 38-41. [14]Chrzan R,Dik P,Klijn AJ,et al.Sling suspension of the bladder neck for pediatric urinary incontinence.J Pediatr Urol.2009;5:82-86. [15]Cher ML, Allen TD.Continence in the myelodysplastic patient following enterocystoplasty. J Urol. 1993;149: 1103. [16]Perez LM, Smith EA, Broecker BH, et al. Outcome of sling cystourethropexy in the pediatric population: a critical review. J Urol.1996; 156(2 Pt 2):642-646. [17]Daneshmand S,Ginsberg DA,Bennet JK,et al.Puboprostatic sling repair for treatment of urethral incompetence in adult neurogenic incontinence.J Urol.2003;V169N1:199-202. [18]Corcos J, Schick E.Evaluation and Treatment of the Neurogenic Bladder (Hardback). Informa Healthcare.2004. [19]Athanasopoulos A, Gyftopoulos K, McGuire EJ. Treating stress urinary incontinence in female patients with neuropathic bladder: the value of the autologous fascia rectus sling. Int Urol Nephrol. 2012; 44(5):1363-7. [20]Snodgrass WT, Elmore J, Adams R. Bladder neck sling and appendicovesicostomy without augmentation for neurogenic incontinence in children. J Urol 2007;177:1510. [21]Bauer SB, Peters CA, Colodny AH, et al. The use of rectus fascia to manage urinary incontinence.J Urol.1989;142: 516. [22]McGuire EJ, Wang CC, Usitalo H, et al.Modified pubovaginal sling in girls with myelodysplasia. J Urol.1986;135:94. [23]Castellan M, Gosalbez R, Labbie A, et al.Bladder neck sling for treatment of neurogenic incontinence in children with augmentation cystoplasty: long-term follow-up. J Urol.2005; 173:21-28. [24]Snodgrass W, Barber T. Cost N.Detrusor compliance changes after bladder neck sling without augmentation in children with neurogenic urinary incontinence. J Urol.2010;183; 2361- 2366. [25]Ulmsten U, Henriksson L, Johnson P, et al. An ambulatory surgical procedure under local anesthesia for treatment of female urinary incontinence. IntUrogynecol J Pelvic Floor Dysfuct.1996;7:81-85. [26]Cox A, Herschorn S, Lee L. Surgical management of female SUI: is there a gold standard? Nat Rev Urol. 2013; 10(2): 78-89. [27]Hamid R,Khastgir J, Arya M,et al.Experience of tension-free vaginal tape for the treatment of stress incontinence in females with neuropathic bladders.Spinal Cord.2003; 41: 118-121. [28] Chau VR, Maxson PM, Joswiak ME, et al. Male sling procedures for stress urinary incontinence. Urol Nurs. 2013; 33(1):9-14. [29] Dean GE,Kunkle DA.Outpatient perineal sling in adolescent boys with neurogenic incontinence.;J Urol.2009;182 Suppl: 1792-1796. [30]Zafirakis H,Wang R,Westney OL.Combination therapy for male erectile dysfunction and urinary incontinence; Asian J Androl.2008;10:149-54. [31]何恢绪,胡卫列,黄孝庭,等.Invance悬带术治疗儿童神经原性括约功能障碍性尿失禁(附二例报告)[J].中华泌尿外科杂志,2010,6(25):418-421. [32]Kurzrock EA,Lowe P,Hardy BE.Bladder wall pedicle wraparound sling for neurogenic urinary incontinence in children.J Urol.1996;155:305-308. [33]Dave S, Pippe Salle JL, Lorenzo AJ, et al.Is long-term bladder deterioration inevitable following successful isolated bladder outlet procedures in children with neuropathic bladder dysfunction? J Urol.2008; 179: 1991. [34]Snodgrass W,Keefover-HicksA,PrietoJ,et al.Comparing outcomes of slings with versus without enterocystoplasty for neurogenic urinary incontinence; J Urol.2009;V181N6: 2709-2714; discussion 2714-2716. [35]Austin PF, Westney OL, Leng WW,et al: Advantages of rectus fascial slings for urinary incontinence in children with neuropathic bladders. J Urol.2001; 165: 2369. [36]Dik P, Klijn AJ, van Gool JD, et al. Transvaginal sling suspension of bladder neck in female patients with neurogenic sphincter incontinence.J Urol 2003;170:580e1. [37]Albouy B, Grise P,SambuisC;Pfister C,et al.Pediatric urinary incontinence: evaluation of bladder wall wraparound sling procedure.J Urol.2007; 177:716-719. [38]Abdul-Rahman A, Attar KH, Hamid R, et al.Long-term outcome of tension-free vaginal tape for treating stress incontinence in women with neuropathic bladders; BJU Int.2010;106:827-830. [39]Xu YM, Zhang XR, Sa YL, et al.Bulbourethral composite suspension for treatment of male-acquired urinary incontinence. EurUrol.2007;51(6):1709-1714. [40]Abouassaly R, Steinberg JR, Lemieux M, ,et al. Complications of tension-free vaginal tape surgery; a multiinstitutional review. BJU Int. 2004;94(1):110-113. [41]Ga?czyński K, Futyma K, Bar K, et al. Bladder injury during sling operation in the treatment of SUI--review of literature and case report. Ginekol Pol. 2012; 83(10):784-788. [42]Mahal AS, Bradley CS. Necrotizing postsurgical infection complicating midurethral sling procedure with unrecognized cystotomy. Female Pelvic Med Reconstr Surg. 2012; 18(3): 183-185. [43]潘慧仙,吕坚伟,冷静,等.经阴道无张力尿道吊带术引起膀胱穿孔的原因分析及处理[J].中国微创外科杂志,2012,(5):422-424. [44]任祥斌.经闭孔悬吊术治疗男性压力性尿失禁的并发症[J].泌尿外科杂志:电子版,2010/02. [45]Madjar S, Jacoby K, Giberti C,et al. Bone anchored sling for the treatment of post-prostatectomy incontinence. J Urol. 2001;165:72-76. [46]Zuckerman JM, Henderson K, McCammon K. Transobturator male sling: is there a learning curve? Can J Urol. 2013; 20(3): 6768-6772. [47]Godbole P,Mackinnon AE.Expanded PTFE bladder neck slings for incontinence in children: the long-term outcome. BJU Int.2004;93:139-141. |
| [1] | Zheng Pei, Xing Xinyang, Huo Hongfeng. Exercises for activating foot valgus muscle: reciprocal inhibitory effects on antagonistic muscle elasticity, tension and hardness [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(8): 1149-1153. |
| [2] | Guo Wen, Leng Jun, Liu Huimin, Zhang Chen, Fang Xiaolei, Wei Fangyue. Visual analysis of literature regarding post-stroke urinary incontinence in the past 10 years [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(35): 5676-5681. |
| [3] | Bai Fuyu, Wang Mengqi, Xue Feng, Li Zhenrui, Yan Qinghao, Zhang Zhiyi, Wang Feng. Characteristics of randomized controlled trials on acupuncture for stress urinary incontinence in women [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(32): 5197-5203. |
| [4] | Ren Tengzhou, Chen Jie, Zhao Wei, Chen Zhiwei, Zhang Teng, Wang Yan. Applicability of stem cells in the treatment of stress urinary incontinence [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(25): 4058-4064. |
| [5] | Cui Tiantian, Yi Lan, Ouyang Hougan, Wu Huiting, Ouyang Yanchu, Chen Chu. Effect of thermosensitive moxibustion in a rat model of pelvic inflammation based on trifocal focal membrane theory [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(20): 3168-3172. |
| [6] | Zhang Yicen, Wang Peixin, Liu Zhicheng. Ultrasound-guided injection of hyaluronic acid and corticosteroid for treating plantar fasciitis: evaluation of pain, fascia thickness and ankle-foot function [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(11): 1670-1674. |
| [7] | Yang Yinhui, Yang Fan, Fan Xu, Xu Fengrui, Zheng Liang, Liu Wei, He Mingwu. Long-term histological changes of diced cartilage grafts wrapped in advanced platelet-rich fibrin membrane [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(34): 5486-5492. |
| [8] |
Liu Huimin, Leng Jun, Guo Wen, Fang Xiaolei, Zhang Chen, Wei Fangyue.
The rules of acupoint selection in the treatment of neurogenic bladder after spinal cord injury with acupuncture and moxibustion: based on data mining technology [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(26): 4237-4242. |
| [9] | Wu Huiting, Cui Tiantian, Ouyang Hougan, Ouyang Yanchu, Yi Lan, Chen Chu. Effect of different courses of heat-sensitive moxibustion on the morphology of surrounding connective tissue and spinal cord in a rat model of osteoporosis [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(20): 3135-3139. |
| [10] | Liang Long, Yu Jie, Wei Xu, Zhou Shuaiqi, Yin Xunlu, Liu Guangwei, Xie Rui, Xie Rong, Zhuang Minghui, Zhu Liguo, Feng Minshan. Establishment and evaluation of a cadaveric model of chronic strain-induced upper cervical spine instability based on fascia-bone theory [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(20): 3152-3156. |
| [11] | Zhou Xuetian, Ma Yong, Guo Yang, Si Yuhao, Zong Yonggang, Zhong Chao. Application status and mechanism of musculoskeletal ultrasound in orthopedic diagnosis [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(16): 2573-2578. |
| [12] | Li Wenhui. Junctophilin and excitation-contraction coupling in skeletal muscles [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(11): 1799-1804. |
| [13] | Mo Fei, Shen Hong-chun, Xu Ya-hong, Li Jian, Zhao Qi-hua, Luo Shun-wen, Lu Yi, Liu Yang, Jia Zhi-gang. Transurethral injection of autologous adipose-derived stem cells for urinary incontinence after radical prostatectomy [J]. Chinese Journal of Tissue Engineering Research, 2018, 22(5): 717-722. |
| [14] | Wang Tian-xing1, Chen Yue-lai2, Yin Ping3, Xu Shi-fen3, Zheng Hui-min3 . Animal models of stress urinary incontinence: selection of appropriate construction methods of research objective-related animal models [J]. Chinese Journal of Tissue Engineering Research, 2018, 22(28): 4557-4561. |
| [15] | Wang Li-xin, Ji Jun, Gao Jia-shuo, Xiao Hong. Uroflowmeter calibration device: standard water flow and its stability [J]. Chinese Journal of Tissue Engineering Research, 2018, 22(22): 3569-3574. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||