Chinese Journal of Tissue Engineering Research ›› 2019, Vol. 23 ›› Issue (16): 2614-2624.doi: 10.3969/j.issn.2095-4344.1219
Meta-analysis of posterior cervical laminectomy titanium mini-plate versus lateral mass screw fixation for treating multilevel cervical spondylotic myelopathy
Wang Wei1, Ma Junfeng1, Cui Zijian2, Zhang Lilong2, Jiang Zehua2, Lu Yun3
- 1Tianjin Medical University, Tianjin 300070, China; 2Tianjin People’s Hospital, Tianjin 300121, China; 3Tianjin Hospital, Tianjin 300210, China
-
Online:2019-06-08Published:2019-06-08 -
Contact:Lu Yun, Professor, Chief physician, Tianjin Hospital, Tianjin 300210, China -
About author:Wang Wei, Master, Tianjin Medical University, Tianjin 300070, China
CLC Number:
Cite this article
Wang Wei, Ma Junfeng, Cui Zijian, Zhang Lilong, Jiang Zehua, Lu Yun. Meta-analysis of posterior cervical laminectomy titanium mini-plate versus lateral mass screw fixation for treating multilevel cervical spondylotic myelopathy [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(16): 2614-2624.
share this article

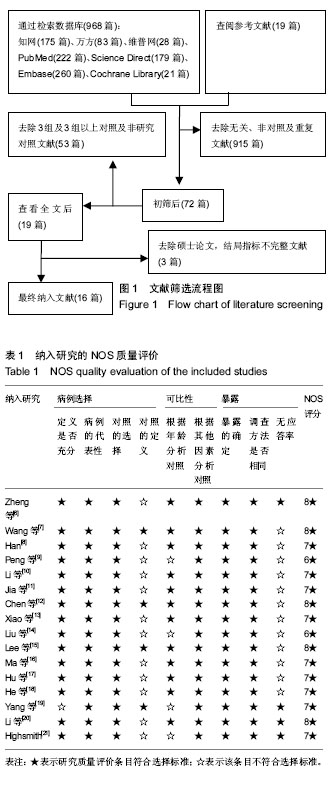
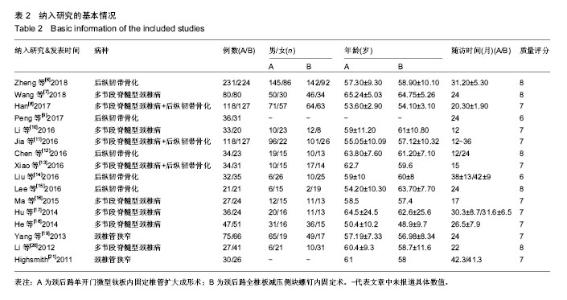
2.1 检索结果 在数据库中共检索出了968篇相关文献,从参考文献中检索出19篇相关文献。初筛去除无关、非对照及重复的文献后,剩下72篇。阅读全文后去除非此次研究相关对照试验及3组及3组以上对照试验,剩下19篇。根据纳入标准去除硕士论文及结局指标不完整文献。最终纳入16篇相关文献[6-21],其中包含4篇英文文献及12篇中文文献,文献检索程序见图1。采用纽卡斯尔-渥太华量表(Newcastle-Ottawa Scale,NOS)对纳入的16篇文献进行质量评价[5],其依据研究人群选择、可比性和暴露情况进行评分。结果显示,16篇文献评价结果均在6★以上,均为高质量研究。纳入研究质量评价见表1。"
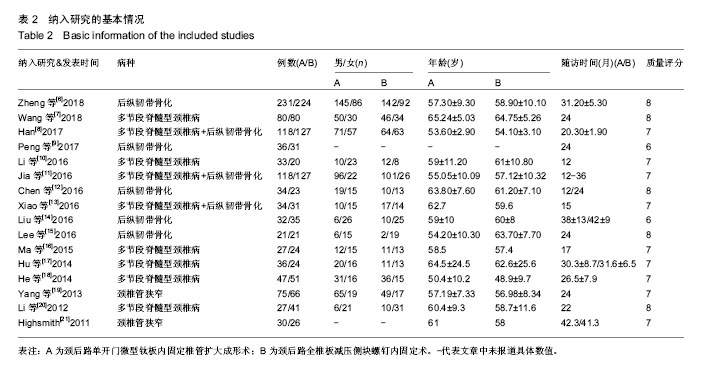
2.2 纳入研究的一般情况 最终纳入的16篇文献中[6-21],包括1 666例患者,其中838例患者行颈后路单开门钛板内固定椎管扩大成形术,828例患者行颈后路全椎板减压侧块螺钉内固定术。不同群体之间、年龄、性别、随访时间差异无显著性意义。纳入文献的基本特征见表2。"
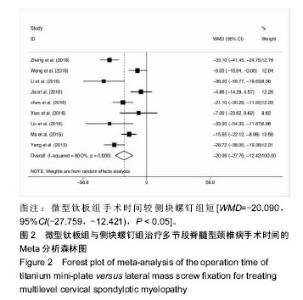
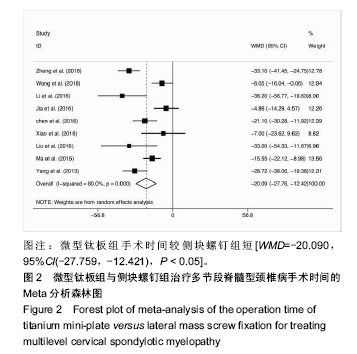
2.3 手术时间和术中出血量 9项研究报告了手术时 间[6-7,10-16,19](微型钛板组n=664,侧块螺钉组n=630),各研究间有异质性(P < 0.1,I2=80%),采用随机效应模型。Meta分析显示,与侧块螺钉组相比,微型钛板组手术时间短[WMD= -20.090,95%CI(-27.759,-12.421),P < 0.05],见图2。分别剔除各项研究进行敏感性分析,发现森林图结果方向均未发生改变,合并效应量结果仍均有统计学意义。"
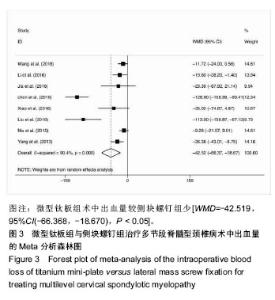
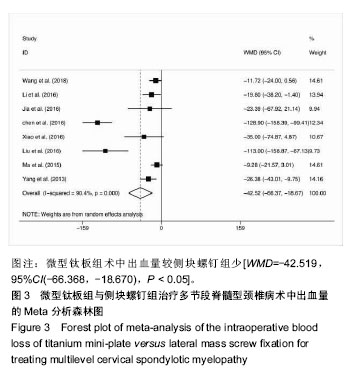
8项研究报告了术中出血量[7,10-14,16,19](微型钛板组 n=664,侧块螺钉组n=630),各研究间有异质性(P < 0.1,I2=90.4%),采用随机效应模型。Meta分析显示,与侧块螺钉组相比,微型钛板组术中出血量少[WMD=-42.519,95%CI(-66.368,-18.670),P < 0.05],见图3。分别剔除各项研究进行敏感性分析,发现森林图结果方向均未发生改变,合并效应量结果仍均有统计学意义。"

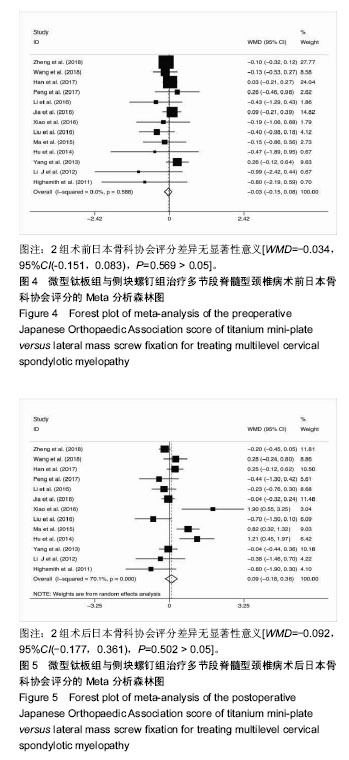
2.4 临床结果 13项研究报道了日本骨科协会评 分[6-11,13-14,16-17,19-21](微型钛板组n=736,侧块螺钉组n= 733)。2组术前日本骨科协会评分差异无显著性意义[WMD= -0.034,95%CI(-0.151,0.083),P=0.569 > 0.05],异质性(P=0.588,I2=0%),采用固定效应模型,见图4。术后日本骨科协会评分在2组间相似[WMD=-0.092,95%CI(-0.177,0.361),P=0.502 > 0.05],异质性:P < 0.1,I2=70.1%,采用随机效应模型,见图5。"

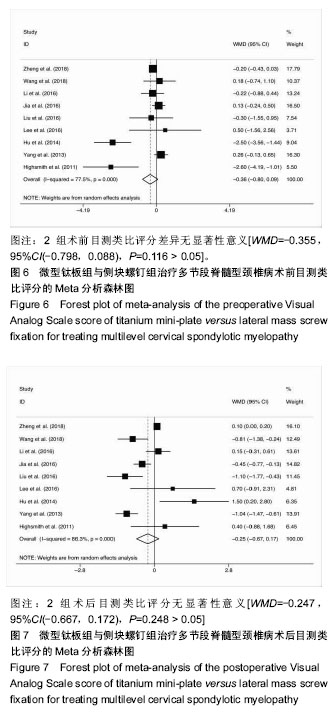
9项研究报道了目测类比评分[6-7,10-11,14-15,17,19,21](微型钛板组n=320,侧块螺钉组n=531)。2组术前目测类比评分差异无显著性意义[WMD=-0.355,95%CI(-0.798,0.088),P=0.116 > 0.05],异质性(P < 0.1,I2=77.5%),采用随机效应模型,见图6。术后目测类比评分在2组间相似[WMD=-0.247,95%CI(-0.667,0.172),P=0.248 > 0.05],异质性:P < 0.1,I2=86.3%,采用随机效应模型,见图7。"

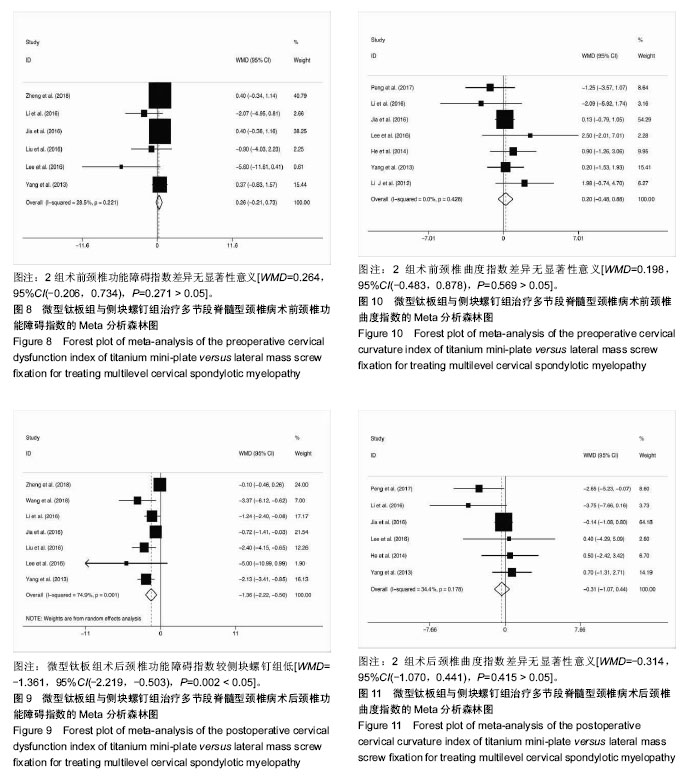
6项研究报道了颈椎功能障碍指数[6,10-11,14-15,19](微型钛板组n=435,侧块螺钉组n=427)。2组术前颈椎功能障碍指数差异无显著性意义[WMD=0.264,95%CI(-0.206,0.734),P=0.271 > 0.05],异质性(P=0.221 > 0.1,I2= 28.5%),采用固定效应模型,见图8。术后颈椎功能障碍指数2组差异有显著性意义[WMD=-1.361,95%CI (-2.219,-0.503),P=0.002 < 0.05],异质性:P=0.001 < 0.1,I2=74.9%,采用随机效应模型,见图9。分别剔除各项研究进行敏感性分析,发现森林图结果方向均未发生改变,合并效应量结果仍均有统计学意义。 7项研究报道了颈椎曲度指数[9-11,15,18-20](微型钛板组n=477,侧块螺钉组n=484)。2组术前颈椎曲度指数差异无显著性意义[WMD=0.198,95%CI(-0.483,0.878),P= 0.569 > 0.05],异质性(P=0.428 > 0.1,I2 = 0%),采用固定效应模型,见图10。术后颈椎曲度指数在2组间相似[WMD=-0.314,95%CI(-1.070,0.441),P=0.415 > 0.05],异质性:P=0.178 > 0.1,I2=34.4%,采用固定效应模型,见图11。"

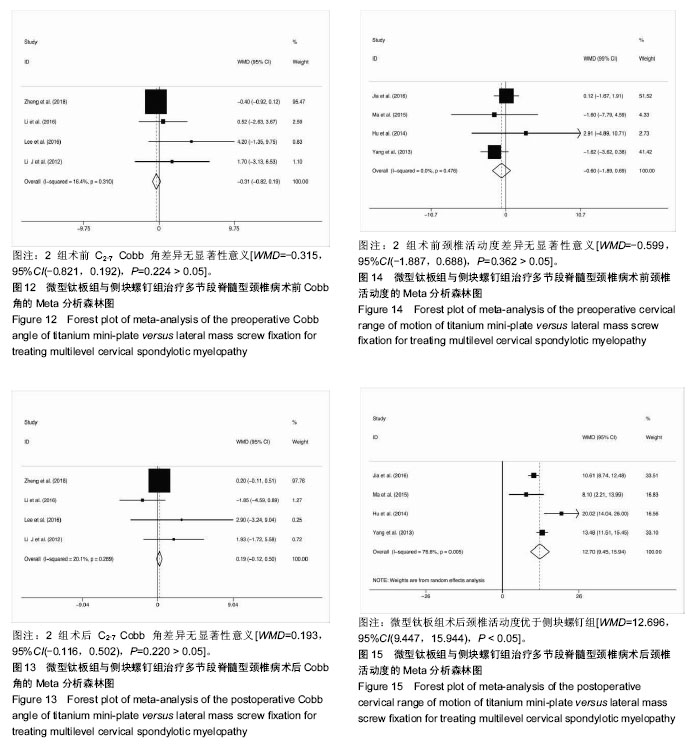
4项研究报道了C2-7 Cobb角[6,10,15,20](微型钛板组n= 312,侧块螺钉组n=306)。2组术前C2-7 Cobb角比较差异无显著性意义[WMD=-0.315,95%CI(-0.821,0.192),P=0.224 > 0.05],异质性(P=0.310 > 0.1,I2 =16.4%),采用固定效应模型,见图12。术后C2-7 Cobb角在2组间相似[WMD= 0.193,95%CI(-0.116,0.502),P=0.220 > 0.05],异质性:P=0.289 > 0.1,I2=20.1%,采用固定效应模型,见图13。 4项研究报道了颈椎活动度[11,16-17,19](微型钛板组 n,侧块螺钉组n=175)。2组术前颈椎活动度差异无显著性意义[WMD=-0.599,95%CI(-1.887,0.688),P= 0.362 > 0.05],异质性(P=0.476 > 0.1,I2 = 0%),采用固定效应模型,见图14。术后颈椎活动度微型钛板组优于侧块螺钉组,差异有显著性意义[WMD=12.696,95%CI(9.447,15.944),P < 0.05],异质性:P = 0.005 < 0.1,I2=76.6%,采用随机效应模型,见图15。分别剔除各项研究进行敏感性分析,发现森林图结果方向均未发生改变,合并效应量结果仍均有统计学意义。=181"

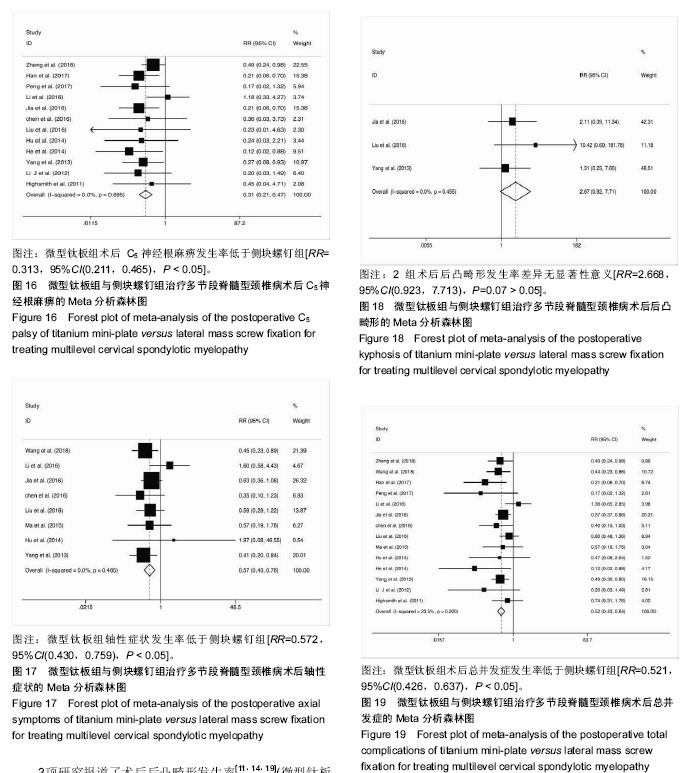
2.5 并发症 12项研究报道了术后C5神经根麻痹发生 率[6,8-12,14,17-21](微型钛板组n=676,侧块螺钉组n=672)。Meta分析显示,微型钛板组术后C5神经根麻痹发生率低于侧块螺钉组[RR=0.313,95%CI(0.211,0.465),P < 0.05],异质性:P=0.695,I2=0%,采用固定效应模型,见图16。 8项研究报道了术后轴性症状发生率[7,10-12,14,16-17,19](微型钛板组n=360,侧块螺钉组n=333)。Meta分析显示,微型钛板组轴性症状发生率低于侧块螺钉组[RR=0.572,95%CI (0.430,0.759),P < 0.05],异质性:P=0.485,I2=0%,采用固定效应模型,见图17。 3项研究报道了术后后凸畸形发生率[11,14,19](微型钛板组n=150,侧块螺钉组n=162)。Meta分析显示,2组术后后凸畸形发生率差异无显著性意义[RR=2.668,95%CI (0.923,7.713),P=0.07 > 0.05],异质性:P=0.455,I2= 0%,采用固定效应模型,见图18。 14项研究报道了术后总并发症发生率[6-12,14,16-21](微型钛板组n=783,侧块螺钉组n=776)。Meta分析显示,微型钛板组术后总并发症发生率低于比侧块螺钉组[RR= 0.521,95%CI(0.426,0.637),P < 0.05],异质性:P= 0.200,I2 = 23.5%,采用固定效应模型,见图19。 "

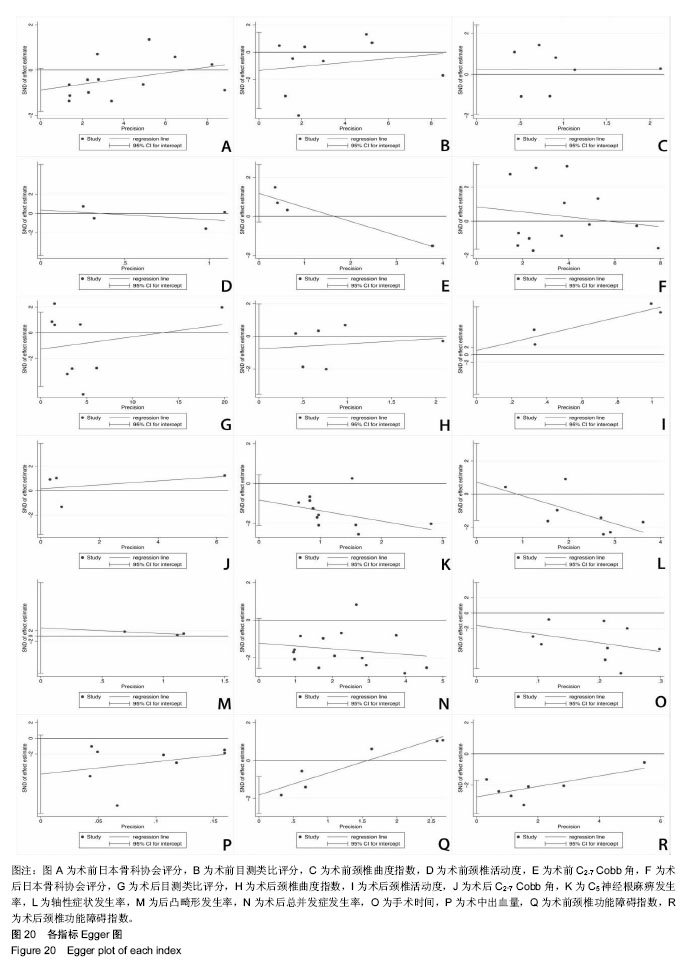
2.6 发表偏倚 共纳入16篇文献,日本骨科协会评分、目测类比评分、颈椎曲度指数、C5神经根麻痹发生率、轴性症状发生率、后凸畸形发生率及总并发症发生率等指标的Egger图P均> 0.05,见图20,表明存在发表偏倚的可能性较小。术后颈椎功能障碍指数Egger图P < 0.05,表明存在相关发表偏倚。尽管如此,进行敏感性分析时对各项研究依次剔除1次,剩余研究进行合并分析,仍都具有统计学意义且森林图结果方向均未发生改变。"
| [1] Xiao SW , Jiang H , Yang LJ , et al. Anterior cervical discectomy versus corpectomy for multilevel cervical spondylotic myelopathy: a meta-analysis. Eur Spine J. 2015;24(1):31-39.[2] Phan K, Scherman DB, Xu J, et al. Laminectomy and fusion vs laminoplasty for multi-level cervical myelopathy: a systematic review and meta-analysis. Eur Spine J. 2016;26(1):1-10.[3] Liu FY, Yang SD, Huo LS, et al. Laminoplasty versus laminectomy and fusion for multilevel cervical compressive myelopathy. Medicine. 2016; 95(23):e3588.[4] Lee CH, Lee J, Kang JD, et al. Laminoplasty versus laminectomy and fusion for multilevel cervical myelopathy: a meta-analysis of clinical and radiological outcomes. J Neurosurg Spine. 2015;22(6):589-95.[5] Wells GA, Shea BJ, O'Connell D, et al. The NewcastleOttawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. Appl Eng Agric. 2002;18(6):727-734.[6] 郑博隆,郝定均,杨小彬,等.单开门椎板成形术和椎板切除并侧块螺钉内固定术治疗颈椎后纵韧带骨化症的疗效比较[J].脊柱外科杂志,2018,16(1):14-21.[7] 王艺伟,黄承,蒋毅. 颈后路两种不同术式治疗脊髓型颈椎病的疗效对比[J]. 颈腰痛杂志, 2018,39(3):366-367.[8] 韩智.多节段脊髓型颈椎病不同手术方法的临床效果对比[J]. 世界最新医学信息文摘, 2017,17(66):39-40.[9] 彭兵,程招军,胡炜,等. 颈后路单开门椎管成形术与全椎板减压术治疗长节段颈椎后纵韧带骨化症效果比较[J]. 山东医药, 2017,57(8):96-98.[10] 李程,王弘,徐宏光,等.多节段脊髓型颈椎病后路手术方法的选择[J]. 皖南医学院学报,2016,35(6):530-533.[11] 贾斌, 张传健, 周晓庆, 等 改良单开门椎板成形术与椎板减压融合内固定术治疗多节段脊髓型颈椎病的效果比较[J].中国医药导报, 2016, 13(12):69-73.[12] 陈刚,戴腾,施克勤. 后路单开门椎管成形术与全椎板切除减压术治疗颈椎后纵韧带骨化症的对比研究[J].中国矫形外科杂志,2016, 24(7):598-602.[13] 肖俊,肖俊,唐广满. 后路单开门微型钢板固定术和全椎板切除侧块螺钉固定术治疗多节段脊髓型颈椎病的对比研究[J].骨科, 2016, 7(3):168-171.[14] Liu X , Chen Y, Yang H , et al. Expansive open-door laminoplasty versus laminectomy and instrumented fusion for cases with cervical ossification of the posterior longitudinal ligament and straight lordosis. Eur Spine J. 2017;26(4):1-8.[15] Lee CH , Jahng TA , Hyun SJ, et al. Expansive laminoplasty versus laminectomy alone versus laminectomy and fusion for cervical ossification of the posterior longitudinal ligament: is there a difference in the clinical outcome and sagittal alignment? Clin Spine Surg. 2016;29(1):E9.[16] 马亮,许永涛,佘远举. 单开门与全椎板切除治疗多节段脊髓型颈椎病疗效比较[J]. 实用骨科杂志,2015,21(11):975-978. [17] 胡勇,赵红勇,董伟鑫,等.Centerpiece 单开门椎板成形术和椎板切除融合术治疗多节段颈脊髓病的临床疗效对比分析.脊柱外科杂志,2014,12(4): 226-230.[18] 贺建军,梁盾,陆兴. 多节段脊髓型颈椎病经颈后路不同术式治疗后C5神经根麻痹的观察对比[J]. 中国医师进修杂志, 2014, 37(12):40-43.[19] Yang L , Gu Y , Shi J , et al. Modified plate-only open-door laminoplasty versus laminectomy and fusion for the treatment of cervical stenotic myelopathy. Orthopedics. 2013;36(1):E79-E87.[20] 李君,王新伟,袁文,等. 颈椎管成形术与椎板切除内固定术后C5神经根麻痹比较[J]. 中华骨科杂志, 2012,32(5):415-419.[21] Highsmith JM. Treatment of cervical stenotic myelopathy: a cost and, outcome comparison of laminoplasty versus laminectomy, and lateral mass fusion. J Neurosurg Spine. 2011;14(5):619.[22] Hirabayashi K, Miyakawa J, Satomi K, et al. Operative results and postoperative progression of ossification among patients with ossification of cervical posterior longitudinal ligament. Spine. 1981;6(4):354.[23] O’Brien MF, Peterson D, Casey AT, et al. A novel technique for laminoplaety augmentation of spinal canal area using titanium miniplate stabilization:a computerized morphometric analysis. Spine. 1996;21(4):474-483.[24] Woods BI, Hohl J, Lee J, et al. Laminoplasty versus Laminectomy and Fusion for Multilevel Cervical Spondylotic Myelopathy. Clin Orthop Relat Res. 2011; 469(3):688-695.[25] Pal GP, Sherk HH. The vertical stability of the cervical spine. Spine. 1988; 13(5):447.[26] 周非非,孙宇,张凤山,等. 颈椎前路椎间盘切除、植骨融合内固定术治疗脊髓型颈椎病术后轴性症状的前瞻性研究[J]. 中国脊柱脊髓杂志, 2014, 24(6): 505-509.[27] Sakaura H, Hosono N, Mukai Y, et al. Preservation of muscles attached to the C2 and C7 spinous processes rather than subaxial deep extensors reduces adverse effects after cervical laminoplasty. Spine. 2010;35(16):782-786.[28] Chen H, Liu H, Li T, et al. Effect of penetration of mini-plate lateral mass screws into facet joint on axial symptoms in cervical laminoplasty. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013;27(11):1324-1330.[29] Fujibayashi S , Neo M , Yoshida M , et al. Neck muscle strength before and after cervical laminoplasty: relation to axial symptoms. J Spinal Disorders Tech. 2010;23(3):197.[30] Atsushi O , Yoshikazu T , Takuya N , et al. The relationship between the anatomy of the nuchal ligament and postoperative axial pain after cervical laminoplasty: cadaver and clinical study. Spine. 2012; 37(26):1607-1613.[31] 江泽华,程招军,方钊,等. C7棘突在颈椎后路椎管扩大成形术中对轴性症状的影响[J]. 中国中医骨伤科杂志, 2017,25(12):40-44.[32] 李亮,燕树义,于学忠,等.两种颈后路术式对颈椎曲度及椎间高度的中期影响[J].中国矫形外科杂志,2013,21(19): 1929-1936.[33] Sasai K , Saito T , Akagi S , et al. Preventing C5 palsy after laminoplasty. Spine. 2003;28(17):1972-1977. |
| [1] | Liu Jinyu, Ding Yu, Jiang Qiang, Cui Hongpeng, Lu Zhengcao. A finite element model of full endoscope lumbar fenestration and biomechanical characteristics [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(27): 4291-4296. |
| [2] | Chen Yuyue, Zou Xiaobao, Ma Xiangyang, Wang Binbin, Yang Haozhi, Ge Su, Zhang Shuang, Ni Ling, Xia Hong, Wu Zenghui. Comparison of cervical motion range and curvature after C3 laminectomy and mini-titanium plate fixation after single-door vertebroplasty [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(12): 1805-1809. |
| [3] | Jiang Qiang, Ding Yu, Liu Jinyu, Cao Shiqi, Lu Zhengcao. Finite element simulation and biomechanical analysis of fully endoscopic precisely laminectomy decompression [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(12): 1891-1896. |
| [4] | Chang Jianzhong, Xiao Wei, Jin Qi, Sun Chengjun, Zhou Yichi, Zhao Zufa, Mao Xiaobing. C3 laminectomy versus C3 laminoplasty for treating multi-segment cervical spondylotic myelopathy: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(16): 2608-2613. |
| [5] | Qiu Hao, Lu Min-peng, Dong Jing, Zhang Zhong-zu, Chu Tong-wei, Wang Qun-bo, Quan Zheng-xue, Jiang Dian-ming. Subtotal corpectomy and reconstruction with titanium mesh cage implantation and pedicle screw fixation through posterior approach in treatment of thoracolumbar burst fracture or thoracolumbar fracture dislocation [J]. Chinese Journal of Tissue Engineering Research, 2016, 20(53): 7932-7938. |
| [6] | Zhou Li, Yang Hong-lin, Cao Xiao-jian. Selective decompression of lumbar root canal and pedicle screw fixation after laminectomy for the treatment of elderly lumbar spinal stenosis: indications and prognosis [J]. Chinese Journal of Tissue Engineering Research, 2016, 20(35): 5195-5202. |
| [7] | Wang Yu-guang, Zhang Chao, Shen Wen, Zheng Chen, Yu Peng, Lu Yun. Effects of topical application of chlorogenic acid on epidural fibrosis and dural adhesion in rat models of laminectomy [J]. Chinese Journal of Tissue Engineering Research, 2015, 19(5): 704-709. |
| [8] | Jin Xin, Zhou Bin-bin, Li Bo-lin,Yang Cheng-cheng, Zhang Hong-sheng. The systematic evaluation of establishing spinal cord transection model in rats [J]. Chinese Journal of Tissue Engineering Research, 2015, 19(40): 6553-6560. |
| [9] | Song Ming-zhi, Dong Chao, Li Dan, Ma Kai. Construction of three-dimensional finite element model with lateral mass screw fixation following lower cervical three-segment laminectomy [J]. Chinese Journal of Tissue Engineering Research, 2014, 18(35): 5640-5646. |
| [10] | Liang Wei-zhi, Gao Jin-wei, Fu Lei, Cui Xiao-hu, Jia Jun-feng. Two kinds of decompression and implant internal fixation for the treatment of cervical spinal stenosis: C5 nerve root palsy and stability [J]. Chinese Journal of Tissue Engineering Research, 2013, 17(35): 6345-6350. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||