Chinese Journal of Tissue Engineering Research ›› 2014, Vol. 18 ›› Issue (53): 8617-8622.doi: 10.3969/j.issn.2095-4344.2014.53.017
Previous Articles Next Articles
Minimally invasive decompression reamed bored external fixator in the repair of chronic sclerosing osteomyelitis of the femur: follow-up of 15 cases of bone healing
Sireyili•Saidula, Alimujiang•Abulaiti, Aihemaitijiang•Yusufu, Maihemuti•Yakufu
- Department of Microsurgical Reconstructive Surgery, First Affiliated Hospital, Xinjiang Medical University, Urumqi 830054, Xinjiang Uygur Autonomous Region, China
-
Revised:2014-11-18Online:2014-12-24Published:2014-12-24 -
Contact:Aihemaitijiang?Yusufu, Chief physician, Doctoral supervisor, Professor, Department of Microsurgical Reconstructive Surgery, First Affiliated Hospital, Xinjiang Medical University, Urumqi 830054, Xinjiang Uygur Autonomous Region, China -
About author:Sireyili?Saidula, Studying for master’s degree, Department of Microsurgical Reconstructive Surgery, First Affiliated Hospital, Xinjiang Medical University, Urumqi 830054, Xinjiang Uygur Autonomous Region, China
CLC Number:
Cite this article
Sireyili•Saidula, Alimujiang•Abulaiti, Aihemaitijiang•Yusufu, Maihemuti•Yakufu . Minimally invasive decompression reamed bored external fixator in the repair of chronic sclerosing osteomyelitis of the femur: follow-up of 15 cases of bone healing[J]. Chinese Journal of Tissue Engineering Research, 2014, 18(53): 8617-8622.
share this article
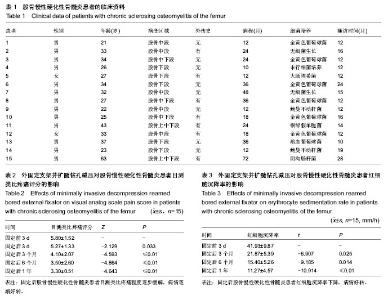
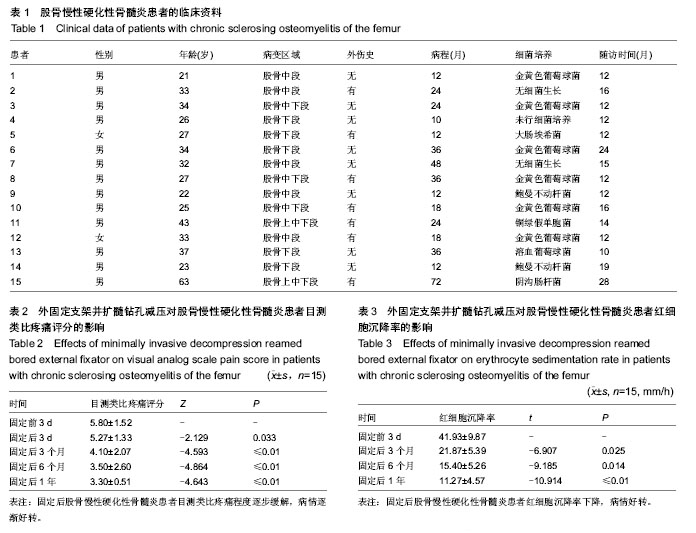
2.1 患者的数量分析及临床资料 15例患者均顺利完成修复治疗,15例患者均获得10-28个月不同时间的随访,平均随访15个月,按照意向性分析,15例患者随访数据均纳入结果分析。患者的临床资料见表1。 2.2 外固定支架并扩髓钻孔减压促进股骨慢性硬化性骨髓炎的骨愈合随访 15例患者均得到随访,平均随访15个月(10-28个月),外固定架取出时间平均3个月。按照疗效判断标准:其中10例愈合(相当于疗效评定标准中的治愈),愈合率67%;4例显效(相当于疗效评定标准中的显效),显效率28%;1例股骨硬化性骨髓炎患者无效(相当于疗效评定标准中的无效),无效率7%。1例膝关节,关节活动部分受限,但比固定前明显改善,4例股骨硬化性骨髓炎患者有一两个针道有不同程度的渗出物,对症治疗后治愈。 2.3 外固定支架并扩髓钻孔减压改善股骨慢性硬化性骨髓炎患者疼痛 与固定前相比,股骨慢性硬化性骨髓炎患者固定后目测类比疼痛评分明显降低(P < 0.05;表2)。 2.4 外固定支架并扩髓钻孔减压降低股骨慢性硬化性骨髓炎患者红细胞沉降率 与固定前3d相比,固定后患者的红细胞沉降率明显下降(P < 0.05;表3)。"
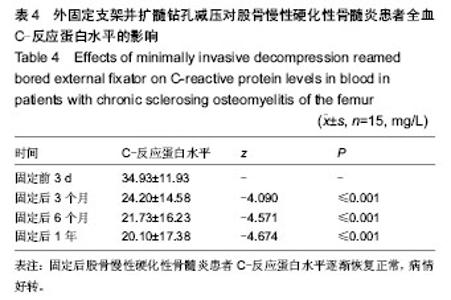
2.5 外固定支架并扩髓钻孔减压降低股骨慢性硬化性骨髓炎患者全血C-反应蛋白水平 与固定前3 d相比,固定后患者的全血C-反应蛋白水平明显下降(P < 0.05;表4)。"

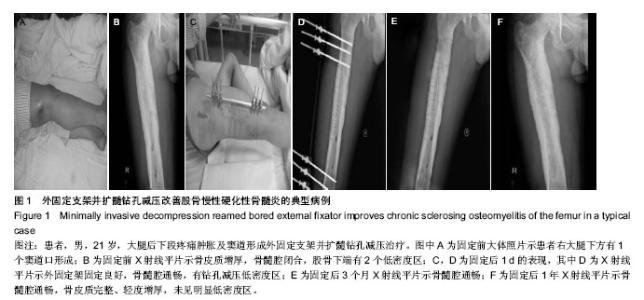
2.6 外固定支架并扩髓钻孔减压改善股骨慢性硬化性骨髓炎的典型病例 患者,男,21岁,无明显原因出现右大腿下段疼痛1年,疼痛逐渐加重,有窦道形成。X射线检查可见骨骨皮质局限性或广泛性肥厚,硬化,骨髓腔狭窄,部分骨髓腔消失。 患者右大腿下方有1个窦道形成,X射线平片示骨皮质增厚,骨髓腔闭合,股骨下端有2个低密度区。行扩髓、钻孔减压加外固定架治疗1 d骨髓腔通畅,有钻孔减压低密度区,1年后X射线平片示骨髓腔通畅,骨皮质完整、轻度增厚,未见明显低密度区(图1)。"

| [1] Canale ST, Beaty JH. Campbell’s Operative Orthopaedics. 11th ed. Philadelphia: Mosby Elsevier, 2007. [2] Lima AL, Oliveira PR, Carvalho VC, et al. Recommendations for the treatment of osteomyelitis. Braz J Infect Dis. 2014; 18(5):526-534. [3] Segev E, Hayek S, Lokiec F, et al. Primary chronic sclerosing (Garré's) osteomyelitis in children. J Pediatr Orthop B. 2001; 10(4):360-364. [4] Suei Y, Tanimoto K, Taguchi A, et al. Possible identity of diffuse sclerosing osteomyelitis and chronic recurrent multifocal osteomyelitis. One entity or two. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;80(4):401-408. [5] Baltensperger M, Grätz K, Bruder E, et al. Is primary chronic osteomyelitis a uniform disease? Proposal of a classification based on a retrospective analysis of patients treated in the past 30 years. J Craniomaxillofac Surg. 2004;32(1):43-50. [6] Schilling F, KesslerS. SAPHO syndrome: clinico- rheumatologic and radiologic differentiation and classification of a patient sample of 86 cases. Z Rheumatol. 2000;59(1): 1-28. [7] Tlougan BE, Podjasek JO, O'Haver J, et al. Chronic recurrent multifocal osteomyelitis (CRMO) and synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome with associated neutrophilic dermatoses: a report of seven cases and review of the literature. Pediatr Dermatol. 2009; 26(5):497-505. [8] Eyrich GK, Harder C, Sailer HF, et al. Primary chronic osteomyelitis associated with synovitis, acne, pustulosis, hyperostosis and osteitis (SAPHO syndrome). J Oral Pathol Med. 1999;28(10):456-464. [9] Urade M, Noguchi K, Takaoka K, et al. Diffuse sclerosing osteomyelitis of the mandible successfully treated with pamidronate: a long-term follow-up report. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114(4):e9-12. [10] Monsour PA, Dalton JB. Chronic recurrent multifocal osteomyelitis involving the mandible: case reports and review of the literature. Dentomaxillofac Radiol. 2010;39(3):184-190. [11] Colina M, La Corte R, Trotta F. Sustained remission of SAPHO syndrome with pamidronate: a follow-up of fourteen cases and a review of the literature. Clin Exp Rheumatol. 2009;27(1):112-115. [12] Jayakar BA, Abelson AG, Yao Q. Treatment of hypertrophic osteoarthropathy with zoledronic acid: case report and review of the literature. Semin Arthritis Rheum. 2011;41(2):291-296. [13] Otsuka K, Hamakawa H, Kayahara H, et al. Chronic recurrent multifocal osteomyelitis involving the mandible in a 4-year-old girl: a case report and a review of the literature. J Oral Maxillofac Surg. 1999;57(8):1013-1016. [14] Mäkitie AA, Törnwall J, Mäkitie O. Bisphosphonate treatment in craniofacial fibrous dysplasia--a case report and review of the literature. Clin Rheumatol. 2008;27(6):809-812. [15] Theologie-Lygidakis N, Schoinohoriti O, Iatrou I. Surgical management of primary chronic osteomyelitis of the jaws in children: a prospective analysis of five cases and review of the literature. Oral Maxillofac Surg. 2011;15(1):41-50. [16] Chun CS. Chronic recurrent multifocal osteomyelitis of the spine and mandible: case report and review of the literature. Pediatrics. 2004;113(4):e380-384. [17] Kuijpers SC, de Jong E, Hamdy NA, et al. Initial results of the treatment of diffuse sclerosing osteomyelitis of the mandible with bisphosphonates. J Craniomaxillofac Surg. 2011; 39(1): 65-68. [18] Lazzarini L, Lipsky BA, Mader JT. Antibiotic treatment of osteomyelitis: what have we learned from 30 years of clinical trials? Int J Infect Dis. 2005;9(3):127-138. [19] Weichert S, Sharland M, Clarke NM, et al. Acute haematogenous osteomyelitis in children: is there any evidence for how long we should treat? Curr Opin Infect Dis. 2008;21(3):258-262. [20] Llorca PM, Miadi-Fargier H, Lançon C, et al. Cost-effectiveness analysis of schizophrenic patient care settings: impact of an atypical antipsychotic under long-acting injection formulation. Encephale. 2005;31(2):235-246. [21] Bibbo C. Reverse sural flap with bifocal Ilizarov technique for tibial osteomyelitis with bone and soft tissue defects. J Foot Ankle Surg. 2014;53(3):344-349. [22] Nikomarov D, Zaidman M, Katzman A, et al. New treatment option for sclerosing osteomyelitis of Garré. J Pediatr Orthop B. 2013;22(6):577-582. [23] Schwartz AJ, Jones NF, Seeger LL, et al. Chronic sclerosing osteomyelitis treated with wide resection and vascularized fibular autograft: a case report. Am J Orthop (Belle Mead NJ). 2010;39(3):E28-32. [24] 陆维举.骨与关节感染[M].南京:江苏科学技术出版社,2007: 50-70. [25] 常向阳, 刘明娟, 张引法, 等.Pain Vision法评估分娩疼痛程度的可靠性:与VAS的比较[J].中华麻醉学杂志, 2013,33(11): 1349-1350. [26] 王新卫, 万明才, 刘继权.骨炎托毒丸治疗硬化性骨髓炎78例临床观察[C].中华中医药学会骨伤科分会2012学术年会论文集•骨病部分, 2012:440. [27] Syed KA, Kuzyk PR, Yoo DJ, et al. Changes in femoral cortical porosity after reaming and intramedullary canal preparation in a canine model. J Arthroplasty. 2013;28(2): 368-373. [28] Danielsson LG, Düppe H. Acute hematogenous osteomyelitis of the neck of the femur in children treated with drilling. Acta Orthop Scand. 2002;73(3):311-316. [29] Lew DP, Waldvogel FA. Osteomyelitis. N Engl J Med. 1997; 336(14):999-1007. [30] Richard S, Davidson MD. The MAC (multi-axial correcting) monolateral external fixation system (Biomet/EBI) technique: an easier way to correct deformity. Oper Tech Orthop. 2011; 21(2):113-124. [31] Harshwal RK, Sankhala SS, Jalan D. Management of nonunion of lower-extremity long bones using mono-lateral external fixator--report of 37 cases. Injury. 2014;45(3): 560-567. [32] 李高陵, 孙长英.开窗减压万古霉素骨水泥链珠填塞治疗硬化性骨髓炎[J].实用骨科杂志, 2014,20(7):662-664. [33] Hernigou P, Manicom O, Poignard A, et al.Core decompression with marrow stem cells. Oper Tech Orthop. 2004;14(2):68-74. |
| [1] | Li Dadi, Zhu Liang, Zheng Li, Zhao Fengchao. Correlation of total knee arthroplasty efficacy with satisfaction and personality characteristics [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1346-1350. |
| [2] | Wei Wei, Li Jian, Huang Linhai, Lan Mindong, Lu Xianwei, Huang Shaodong. Factors affecting fall fear in the first movement of elderly patients after total knee or hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1351-1355. |
| [3] | Lü Zhen, Bai Jinzhu. A prospective study on the application of staged lumbar motion chain rehabilitation based on McKenzie’s technique after lumbar percutaneous transforaminal endoscopic discectomy [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1398-1403. |
| [4] | Chen Xinmin, Li Wenbiao, Xiong Kaikai, Xiong Xiaoyan, Zheng Liqin, Li Musheng, Zheng Yongze, Lin Ziling. Type A3.3 femoral intertrochanteric fracture with augmented proximal femoral nail anti-rotation in the elderly: finite element analysis of the optimal amount of bone cement [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1404-1409. |
| [5] | Du Xiupeng, Yang Zhaohui. Effect of degree of initial deformity of impacted femoral neck fractures under 65 years of age on femoral neck shortening [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1410-1416. |
| [6] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [7] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Comparison of the short-term efficacy of extracorporeal shock wave therapy for middle-aged and elderly knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1471-1476. |
| [8] | Gao Yan, Zhao Licong, Zhao Hongzeng, Zhu Yuanyuan, Li Jie, Sang Deen. Alteration of low frequency fluctuation amplitude at brain-resting state in patients with chronic discogenic low back pain [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1160-1165. |
| [9] | Cai Qunbin, Zou Xia, Hu Jiantao, Chen Xinmin, Zheng Liqin, Huang Peizhen, Lin Ziling, Jiang Ziwei. Relationship between tip-apex distance and stability of intertrochanteric femoral fractures with proximal femoral anti-rotation nail: a finite element analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 831-836. |
| [10] | Zhao Zhongyi, Li Yongzhen, Chen Feng, Ji Aiyu. Comparison of total knee arthroplasty and unicompartmental knee arthroplasty in treatment of traumatic osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 854-859. |
| [11] | Zhang Nianjun, Chen Ru. Analgesic effect of cocktail therapy combined with femoral nerve block on total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 866-872. |
| [12] | Wu Gang, Chen Jianwen, Wang Shilong, Duan Xiaoran, Liu Haijun, Dong Jianfeng. Simple HyProCure subtalar stabilization in treatment of adolescent flexible flatfoot combined with painful accessory navicular bone [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 901-905. |
| [13] | Li Yan, Wang Pei, Deng Donghuan, Yan Wei, Li Lei, Jiang Hongjiang. Electroacupuncture for pain control after total knee arthroplasty: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 957-963. |
| [14] | Hua Haotian, Zhao Wenyu, Zhang Lei, Bai Wenbo, Wang Xinwei. Meta-analysis of clinical efficacy and safety of antibiotic artificial bone in the treatment of chronic osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 970-976. |
| [15] | Liu Jiangfeng. Nano-hydroxyapatite/polyamide 66 composite filling combined with locking plate in the treatment of fibrous dysplasia of femoral bone [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 542-547. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||