Chinese Journal of Tissue Engineering Research ›› 2026, Vol. 30 ›› Issue (16): 4219-4228.doi: 10.12307/2026.710
Previous Articles Next Articles
Network meta-analysis of robot-assisted gait training interventions on lower limb motor function in stroke patients
Gao Zan1, Liu Yixuan2, Zhang Lichen1, Hou Bing1, Tang Yalei1, Li Shumei1, Che Pengcheng1, Dou Na1
- 1College of Nursing and Rehabilitation, 2School of Emergency Management and Safety Engineering, North China University of Science and Technology, Tangshan 063210, Hebei Province, China
-
Received:2025-07-29Accepted:2025-08-27Online:2026-06-08Published:2025-11-28 -
Contact:Dou Na, MS, Associate professor, College of Nursing and Rehabilitation, North China University of Science and Technology, Tangshan 063210, Hebei Province, China Co-corresponding author: Che Pengcheng, Professor, College of Nursing and Rehabilitation, North China University of Science and Technology, Tangshan 063210, Hebei Province, China -
About author:Gao Zan, MS candidate, College of Nursing and Rehabilitation, North China University of Science and Technology, Tangshan 063210, Hebei Province, China Liu Yixuan, School of Emergency Management and Safety Engineering, North China University of Science and Technology, Tangshan 063210, Hebei Province, China Gao Zan and Liu Yixuan contributed equally to this work. -
Supported by:Hebei Provincial Medical Science Research Project in 2024, No. 20240161 (to DN); Hebei Provincial Key Laboratory of Rehabilitation Engineering and Regenerative Medicine, No. SZX202327 (to CPC); Hebei Provincial “Robot+” Application “Best Candidate” Project (to CPC)
CLC Number:
Cite this article
Gao Zan, Liu Yixuan, Zhang Lichen, Hou Bing, Tang Yalei, Li Shumei, Che Pengcheng, Dou Na. Network meta-analysis of robot-assisted gait training interventions on lower limb motor function in stroke patients[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(16): 4219-4228.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
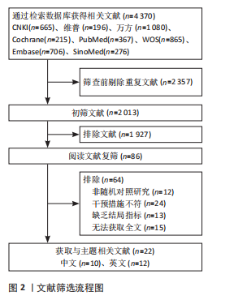
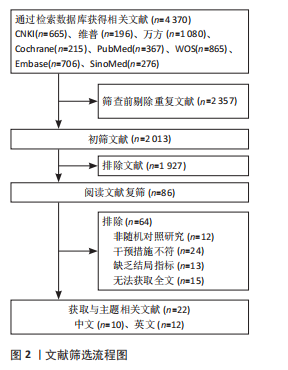
2.1 文献检索结果 初步检索中文数据库得到中国知网665篇、维普196篇和万方1 080篇;英文数据库:Cochrane Library 215篇、PubMed 367篇、Web of Science 865篇和Embase 706篇以及SinoMed 276篇,经过层层筛选,最终纳入22项研究[14-35]。具体筛选流程图见图2。"
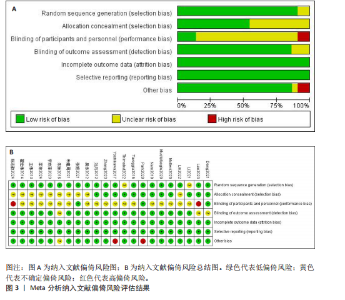
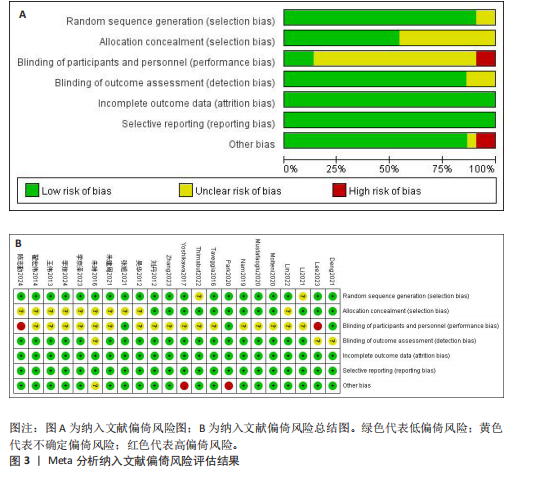
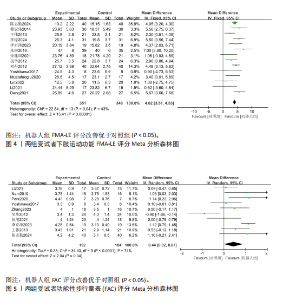
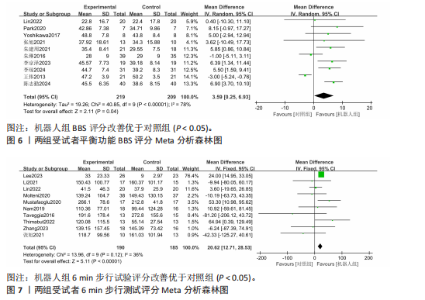
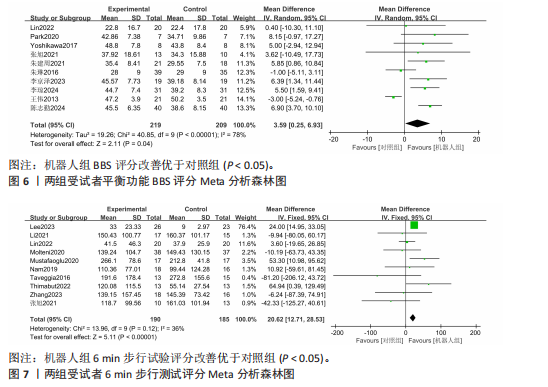
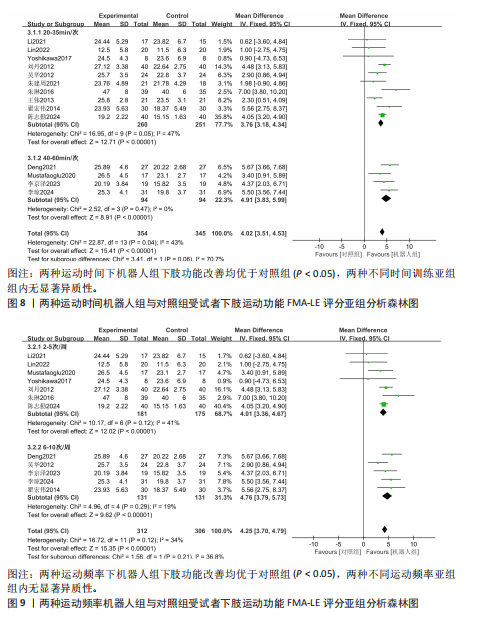
2.2 文献纳入质量评估结果 图3偏倚风险评估结果,随机序列生成、分配隐藏、对受试者和研究人员的盲法、对结果评估者的盲法、结果数据完整性、选择性报告和其他偏倚7个方面均可能有一定偏倚风险,其中随机序列生成、对结果评估者的盲法、不完整的结局数据和选择性报告主要为低偏倚风险;随机序列生成、分配隐藏、对结果评估者的盲法有不确定偏倚风险;对受试者和研究人员的盲法及其他偏倚有不确定和高偏倚风险。 2.3 Meta分析结果 2.3.1 FMA-LE评分 FMA-LE展示评分结果见图4,共纳入14项研究[14-15,18,22-26,28-31,34-35],机器人组351例,对照组348例(P=0.04,I2= 43%),异质性小,采用固定效应模型。结果分析显示,FMA-LE评分机器人组改善优于对照组(MD=4.02,95%CI:3.51-4.53,P < 0.05)。 2.3.2 FAC评分 FAC展示评分结果见图5。共纳入10项研究[15,17,19-20,22-25,28,33], 机器人组192例,对照组184例(P < 0.000 1,I2=74%),异质性大,采用随机效应模型。结果分析显示,FAC评分机器人组改善优于对照组(MD=0.44,95%CI:0.02-0.87,P < 0.05)。 2.3.3 BBS评分 BBS展示评分结果见图6,共纳入10项研究[14-15,17,20,23-24,28,30-31,34],机器人组219例,对照组209例(P < 0.000 1,I2=78%),异质性大,采用随机效应模型。结果分析显示,BBS评分机器人组改善优于对照组(MD=3.59,95%CI:0.25-6.93,P < 0.05)。 2.3.4 6 min步行试验评分 6 min步行试验展示评分结果如图7,共纳入10项研究[16-19,21-22,27,32-34],机器人组190例,对照组185例(P=0.12,I2=36%),异质性小,采用固定效应模型。结果分析显示,6 min步行试验评分机器人组改善优于对照组(MD=20.62,95%CI:12.71-28.53,P < 0.05)。 2.4 亚组分析 机器人组根据运动处方、患者病程和机器人类型进行亚组分析。①按照运动时间不同分为2个亚组:20-35 min/次训练组和40-"
"

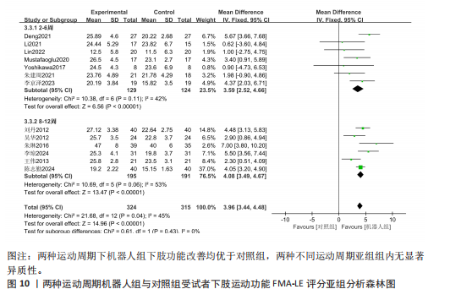
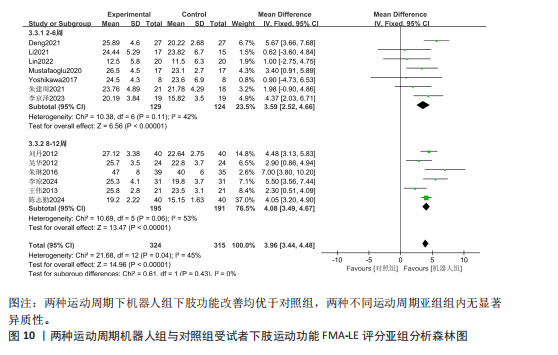
60 min/次训练组;②按照运动频率不同分为2个亚组:2-5次/周组和6-10次/周组;③按照运动周期不同分为2个亚组:2-6周组和8-12周组;④按照病程分为2个亚组:病程< 6个月组和病程> 6个月组;⑤将机器人的类型分为2种:减重机器人组和地面行走机器人组。由于FAC、BBS和6 min步行试验评分的研究数量较少和样本量较小,仅对FMA-LE评分进行了亚组分析。 2.4.1 运动时间对脑卒中患者FMA-LE评分的影响 每个亚组运动时间的FMA-LE评分见图8。有10项研究[14-15,22-23,25-26,28,31,34-35],展示了运动时间为20-35 min/次运动,结果为:P=0.05,I2=47%,采用固定效应模型进行分析。有4项研究[18,24,29-30],展示了运动时间为40-60 min/次运动,结果为:P=0.47,I2=0%,采用固定效应模型进行分析。结果表明两种运动时间下机器人组下肢功能改善优于对照组(P < 0.05),亚组分析组内无显著异质性。 2.4.2 运动频率对脑卒中患者FMA-LE评分的影响 每个亚组运动评频率的FMA-LE评分见图9。有7项研究[14-15,18,22,28,34-35],展示了运动频率为2-5次/周,结果为:P=0.12,I2=41%,采用固定效应模型进行分析。有5项研究[24-26,29-30],展示运动时间为6-10次/周,结果为:P=0.29,I2=19%,采用固定效应模型进行分析。结果表明两种运动频率下机器人组下肢功能改善均优于对照组(P < 0.05),亚组分析组内无显著异质性。 2.4.3 运动周期对脑卒中患者FMA-LE评分的影响 每个亚组运动周期的FMA-LE评分见图10。有7项研究[18,22,24,28-29,31,34],展示了运动周期为2-6周,结果为:P=0.11,I2=42%,采用固定效应模型进行分析。有6项研究[14-15,23,25,30,35],展示了运动周期为8-12周,结果为:P=0.06,I2=53%,采用固定效应模型进行分析。结果表明两种运动周期下机器人组下肢功能改善均优于对照组,亚组分析组内无显著异质性。"

"
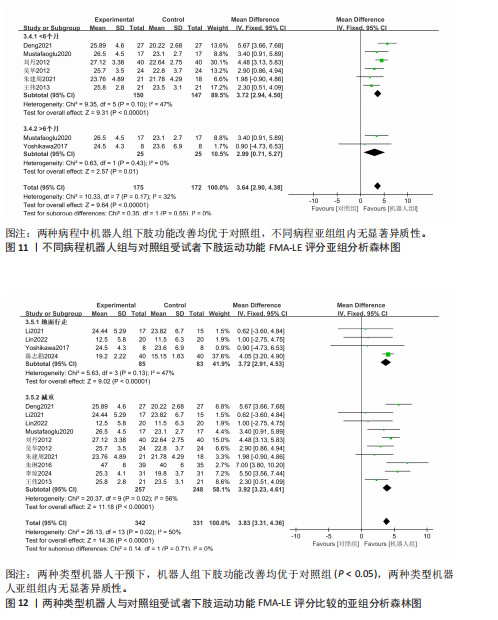
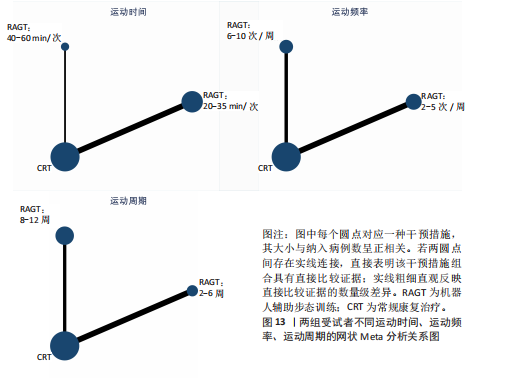
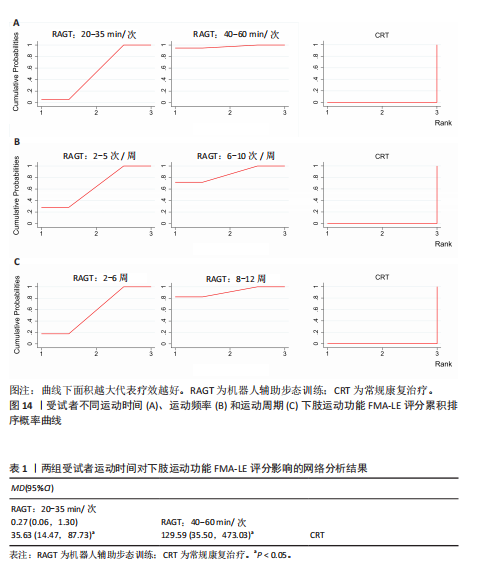
2.4.4 病程对脑卒中患者FMA-LE评分的影响 基于患者病程每个亚组的FMA-LE评分见图11。有6项研究[18,23,25,29,31,35],展示了病程< 6个月,结果为:P=0.10,I2=47%,采用固定效应模型进行分析。有2项研究[18,28],展示了病程> 6个月,结果为:P=0.43,I2=0%,采用固定效应模型进行分析。结果表明两种病程中机器人组下肢功能改善均优于对照组,亚组分析组内无显著异质性。 2.4.5 机器人类型对脑卒中患者FMA-LE评分的影响 基于机器人类型每个亚组的FMA-LE评分见图12。有4项研究[15,22,28,34],展示了地面行走机器人,结果为:P=0.13,I2=47%,采用固定效应模型进行分析。有10项研究[14,18,22-23,25,29-31,34-35],展示了减重机器人,结果为:P=0.02,I2=56%,采用随机效应模型进行分析。结果表明两种类型机器人干预下,机器人组下肢功能改善均优于对照组(P < 0.05),亚组分析组内无显著异质性。 2.5 Meta分析网络证据图 采用与亚组分析指标FMA-LE一致的方式进行网络荟萃分析,绘制网络证据图。在FMA-LE评分的网状Meta分析中,各干预措施之间的关系通过节点和连线进行了直观展示,每个节点代表一种特定的干预措施,节点的大小与参与该干预的受试者人数呈正比。节点之间的实线连接反映了直接比较这些干预措施的研究数量,其中粗线表示较多研究支持,反之较少,见图13。由于研究网络中不存在闭环结构,因此无需进行不一致性检验。 2.6 基于运动处方进行分组的累计概率 不同运动时间、运动频率和运动周期FMA-LE评分网络分析的累积概率见图14 。运动时间曲线下面积、累积排序概率曲线(SUCRA)、曲线下面积的大小通常反映治疗效果的不同。曲线下面积越大,表明治疗效果越显著。 2.6.1 FMA-LE评分运动时间网状Meta分析结果 机器人辅助步态训练20-35 min/次(MD=35.63, 95%CI:14.47-87.73) 和机器人辅助步态训练"

"
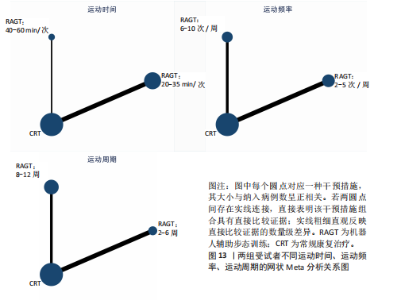
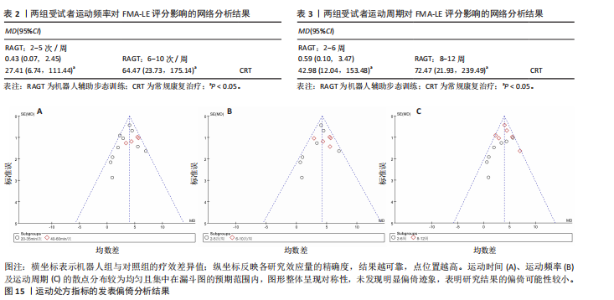
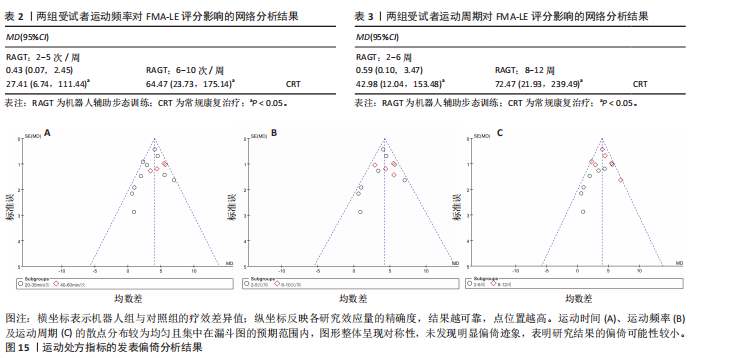
40-60 min/次(MD=129.59,95%CI:35.50-473.03) 与常规康复治疗相比均能改善FMA-LE评分 (P < 0.05),机器人辅助步态训练20-35 min/次与机器人辅助步态训练40-60 min/次相比差异无显著性意义 (P > 0.05),见表1。 受试者运动时间曲线下面积显示训练时间效果排序为:机器人辅助步态训练40-60 min/次> 机器人辅助步态训练20-35 min/次> 常规康复。表明训练40-60 min/次是最佳训练时间,见图14A。 2.6.2 FMA-LE 评分运动频率网状Meta分析结果 机器人辅助步态训练2-5次/周(MD=27.41,95%CI:6.74-111.44) 和6-10次/周(MD=64.47,95%CI:23.73-175.14) 与常规康复治疗相比均能改善FMA-LE评分的运动频率(P < 0.05),机器人辅助步态训练2-5次/周与6-10次/周相比差异无显著性意义 (P > 0.05),见表2。 受试者运动频率曲线下面积显示运动频率效果排序为:机器人辅助步态训练6-10次/周> 机器人辅助步态训练2-5次/周> 常规康复。表明训练6-10次/周是最佳训练频率,见图14B。 2.6.3 FMA-LE 评分运动周期网状Meta分析结果 机器人辅助步态训练2-6周(MD=42.98,95%CI:12.04-153.48) 和8-12周(MD= 72.47,95%CI:21.93-239.49) 与常规康复治疗相比均能改善运动周期的FMA-LE评分(P < 0.05),机器人辅助步态训练2-6周与8-12周相比差异无显著性意义 (P > 0.05),见表3。 受试者运动周期曲线下面积显示运动周期效果排序为:机器人辅助步态训练8-12周> 机器人辅助步态训练2-6周> 常规康复。表明训练8-12周是最佳训练周期,见图14C。 2.7 发表偏倚 为评估运动处方指标的发表偏倚,采用漏斗图进行了分析。结果显示:运动时间、运动频率及运动周期的散点分布较为均匀且集中在漏斗图的预期范围内,图形整体呈现对称性,未发现明显偏倚迹象,这表明研究结果的稳定性较高,见图15。"

"
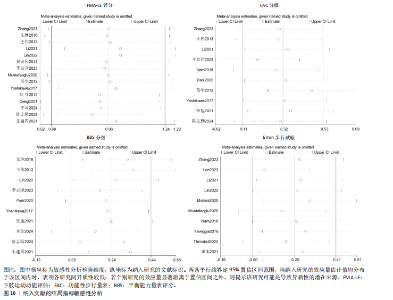
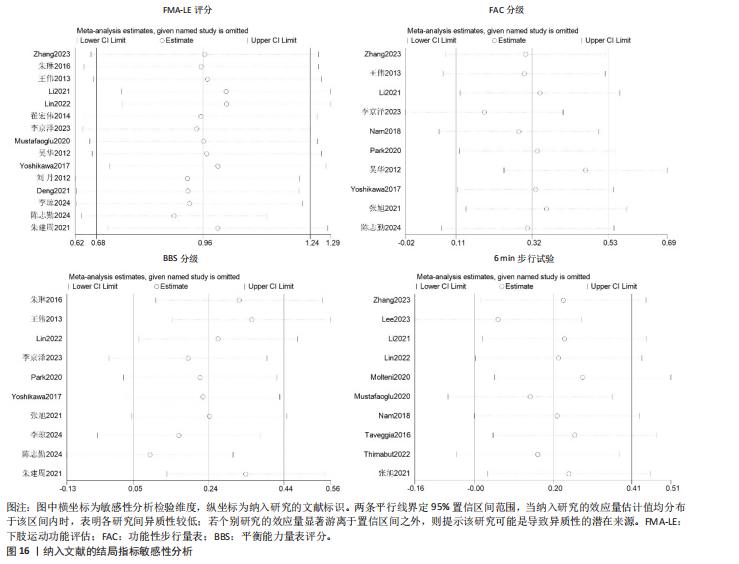
2.8 结局指标敏感性分析 以FMA-LE评分、FAC分级、BBS分级及6 min步行试验距离为结局指标的分析显示,研究间未发现显著异质性。图16敏感性分析进一步验证了临床疗效的稳定性,表明研究结果具有较高的可靠性。"
"
| [1] FEIGIN VL, OWOLABI MO. Pragmatic solutions to reduce the global burden of stroke: a World Stroke Organization-Lancet Neurology Commission. Lancet Neurology. 2023;22(12):1160-1206. [2] BATCHELOR FA, WILLIAMS SB, WIJERATNE T, et al. Balance and Gait Impairment in Transient Ischemic Attack and Minor Stroke.J Stroke Cerebrovasc Dis. 2015;24(10): 2291-2297. [3] HENDRICKS HT, VAN LIMBEEK J, GEURTS AC, et al. Motor recovery after stroke: a systematic review of the literature. Arch Phys Med Rehabil. 2002;83(11):1629-1637. [4] POURNAJAF S, CALABRò RS, NARO A, et al. Robotic versus Conventional Overground Gait Training in Subacute Stroke Survivors: A Multicenter Controlled Clinical Trial. J Clin Med. 2023;12(2):439. [5] LANGHORNE P, BERNHARDT J, KWAKKEL G. Stroke rehabilitation.Lancet. 2011; 377(9778):1693-1702. [6] MARíN-MEDINA DS, ARENAS-VARGAS PA, ARIAS-BOTERO JC, et al. New approaches to recovery after stroke. Neurol Sci. 2024; 45(1):55-63. [7] TANG Z, ZHAO Y, SUN X, et al. Evidence that robot-assisted gait training modulates neuroplasticity after stroke: An fMRI pilot study based on graph theory analysis. Brain Res. 2024;1842:149113. [8] YOO M, CHUN MH, HONG GR, et al. Effects of Training with a Powered Exoskeleton on Cortical Activity Modulation in Hemiparetic Chronic Stroke Patients: A Randomized Controlled Pilot Trial. Arch Phys Med Rehabil 2023;104(10):1620-1629. [9] TORTORA S, TONIN L, SIEGHARTSLEITNER S, et al. Effect of Lower Limb Exoskeleton on the Modulation of Neural Activity and Gait Classification. IEEE Trans Neural Syst Rehabil Eng. 2023;31:2988-3003. [10] 胡坤, 刘辉辉, 张晓武. 下肢智能康复机器人对脑卒中偏瘫患者下肢运动功能的影响[J].神经损伤与功能重建,2019, 14(1):22-25. [11] BARICICH A, BORG MB, BATTAGLIA M, et al. High-Intensity Exercise Training Impact on Cardiorespiratory Fitness, Gait Ability, and Balance in Stroke Survivors: A Systematic Review and Meta-Analysis. J Clin Med. 2024;13(18):5498. [12] BOYNE P, BILLINGER SA, REISMAN DS, et al. Optimal Intensity and Duration of Walking Rehabilitation in Patients With Chronic Stroke: A Randomized Clinical Trial. JAMA Neurol. 2023;80(4):342-351. [13] 曾进胜, 蒲传强. 我国各类主要脑血管病诊断要点演变与更新[J].中华神经科杂志,2019,52(9):681-683. [14] 朱琳, 宋为群, 刘霖, 等. 下肢康复机器人联合任务导向训练对卒中后步行能力的康复作用[J]. 中国脑血管病杂志,2016, 13(5):240-248. [15] 陈志勤, 王芳, 王锐.下肢康复机器人辅助训练对脑梗死偏瘫患者恢复情况的影响[J]. 机器人外科学杂志(中英文),2024, 5(6):1105-1110. [16] TAVEGGIA G, BORBONI A, MULé C, et al. Conflicting results of robot-assisted versus usual gait training during postacute rehabilitation of stroke patients: a randomized clinical trial.Int J Rehabil Res. 2016;39(1):29-35. [17] 张旭, 邱模炎, 权范善, 等.步行机器人训练对慢性期脑卒中偏瘫患者步行能力的影响[J].中华物理医学与康复杂志, 2021,43(1):30-33. [18] MUSTAFAOGLU R, ERHAN B, YELDAN I, et al. Does robot-assisted gait training improve mobility, activities of daily living and quality of life in stroke? A single-blinded, randomized controlled trial. Acta Neurol Belg. 2020;120(2):335-344. [19] NAM YG, LEE JW, PARK JW, et al. Effects of Electromechanical Exoskeleton-Assisted Gait Training on Walking Ability of Stroke Patients: A Randomized Controlled Trial. Arch Phys Med Rehabil. 2019;100(1):26-31. [20] PARK C, OH-PARK M, DOHLE C, et al. Effects of innovative hip-knee-ankle interlimb coordinated robot training on ambulation, cardiopulmonary function, depression, and fall confidence in acute hemiplegia. NeuroRehabilitation. 2020;46(4):577-587. [21] THIMABUT N, YOTNUENGNIT P, CHAROENLIMPRASERT J, et al. Effects of the Robot-Assisted Gait Training Device Plus Physiotherapy in Improving Ambulatory Functions in Patients With Subacute Stroke With Hemiplegia: An Assessor-Blinded, Randomized Controlled Trial. Arch Phys Med Rehabil. 2022;103(5):843-850. [22] LI Y, FAN T, QI Q, et al. Efficacy of a Novel Exoskeletal Robot for Locomotor Rehabilitation in Stroke Patients: A Multi-center, Non-inferiority, Randomized Controlled Trial. Front Aging Neurosci. 2021;13:706569. [23] 王伟, 李岩, 吴华, 等. 下肢康复机器人训练对急性脑卒中患者下肢运动功能的影响[J].中华物理医学与康复杂志,2013, 35(6):464-467. [24] 李京泽, 邢靖松, 吕福现, 等.肢康复机器人训练对脑卒中偏瘫患者步行功能的影响[J].机器人外科学杂志(中英文), 2023,4(6):512-516. [25] 吴华, 顾旭东, 傅建明, 等. 下肢康复机器人系统对卒中偏瘫患者运动功能的影响[J].中华医学杂志,2012,92(39):2628-2631. [26] 翟宏伟, 陈伟, 孙洁, 等.下肢康复机器人对脑卒中偏瘫患者运动功能恢复及体感诱发电位的影响[J].中华物理医学与康复杂志,2014,36(10):784-786. [27] MOLTENI F, GUANZIROLI E, GOFFREDO M, et al. Gait Recovery with an Overground Powered Exoskeleton: A Randomized Controlled Trial on Subacute Stroke Subjects. Brain Sci. 2021;11(1):104. [28] YOSHIKAWA K, MIZUKAMI M, KAWAMOTO H, et al. Gait training with Hybrid Assistive Limb enhances the gait functions in subacute stroke patients: A pilot study. NeuroRehabilitation. 2017;40(1):87-97. [29] YU D, YANG Z, LEI L, et al. Robot-Assisted Gait Training Plan for Patients in Poststroke Recovery Period: A Single Blind Randomized Controlled Trial. Biomed Res Int. 2021;2021: 5820304. [30] 李琼, 杨勇, 李晓婷, 等.下肢康复机器人辅助步态训练对脑卒中下肢运动功能障碍的运动功能与运动生物力学变化研究[J]. 中国临床实用医学,2024,15(1):51-56. [31] 朱建周, 袁华, 毛利, 等. 末端驱动型下肢机器人对脑卒中患者步态的影响[J].中华物理医学与康复杂志,2021,43(7):631-634. [32] LEE YH, KO LW, HSU CY, et al. Therapeutic Effects of Robotic-Exoskeleton-Assisted Gait Rehabilitation and Predictive Factors of Significant Improvements in Stroke Patients: A Randomized Controlled Trial. Bioengineering (Basel). 2023;10(5):585. [33] ZHANG H, LI X, GONG Y, et al. Three-Dimensional Gait Analysis and sEMG Measures for Robotic-Assisted Gait Training in Subacute Stroke: A Randomized Controlled Trial. Biomed Res Int. 2023; 2023:7563802. [34] LIN YN, HUANG SW, KUAN YC, et al. Hybrid robot-assisted gait training for motor function in subacute stroke: a single-blind randomized controlled trial. J Neuroeng Rehabil. 2022;19(1):99. [35] 刘丹, 李建民, 赵雅宁, 等. Lokomat康复训练机器人对脑卒中患者步态及下肢关节角度的影响[J]. 中国老年学杂志,2012, 32(20):4371-4372. [36] CALABRÒ RS, SORRENTINO G, CASSIO A, et al. Robotic-assisted gait rehabilitation following stroke: a systematic review of current guidelines and practical clinical recommendations. Eur J Phys Rehabil Med. 2021;57(3):460-471. [37] MEHRHOLZ J, THOMAS S, KUGLER J, et al. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev. 2020;10(10):Cd006185. [38] MEHRHOLZ J, THOMAS S, KUGLER J, et al. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev. 2017;5(5):CD006185. [39] VAN NUNEN MP, GERRITS KH, KONIJNENBELT M, et al. Recovery of walking ability using a robotic device in subacute stroke patients: a randomized controlled study. Disabil Rehabil Assist Technol. 2015;10(2):141-148. [40] 王寒明, 杨傲然, 王欢, 等.机器人辅助步态训练联合综合康复训练对脑卒中患者步态及生活质量的影响[J]. 中国实用神经疾病杂志,2021,24(20):1793-1801. [41] DE LEON RD, HODGSON JA, ROY RR, et al. Locomotor capacity attributable to step training versus spontaneous recovery after spinalization in adult cats. J Neurophysiol. 1998;79(3):1329-1340. [42] NOCCHI F, GAZZELLINI S, GRISOLIA C, et al. Brain network involved in visual processing of movement stimuli used in upper limb robotic training: an fMRI study. J Neuroeng Rehabil. 2012;9:49. [43] HORNBY TG, STRAUBE DS, KINNAIRD CR, et al. Importance of specificity, amount, and intensity of locomotor training to improve ambulatory function in patients poststroke.Top Stroke Rehabil. 2011;18(4):293-307. [44] Rose DK, Nadeau SE, Wu SS, et al. Locomotor Training and Strength and Balance Exercises for Walking Recovery After Stroke: Response to Number of Training Sessions. Phys Ther. 2017;97(11):1066-1074. [45] ZHANG Y, ZHAO W, WAN C, et al. Exoskeleton rehabilitation robot training for balance and lower limb function in sub-acute stroke patients: a pilot, randomized controlled trial. J Neuroeng Rehabil. 2024; 21(1):98. [46] 周莉,李江东,刘景隆.脑卒中患者开始康复时间和康复持续时间与运动功能的恢复[J].中国临床康复,2005,9(17):1-3. [47] BIERNASKIE J, CHERNENKO G, CORBETT D. Efficacy of rehabilitative experience declines with time after focal ischemic brain injury. J Neurosci.2004;24(5):1245-1254. [48] MOLTENI F, GASPERINI G, CANNAVIELLO G, et al. Exoskeleton and End-Effector Robots for Upper and Lower Limbs Rehabilitation: Narrative Review. PM R. 2018;10(9 Suppl 2): S174-S188. [49] LI S, CARMICHAEL ST. Growth-associated gene and protein expression in the region of axonal sprouting in the aged brain after stroke. Neurobiol Dis.2006;23(2):362-373. [50] CASSIDY JM, CRAMER SC. Spontaneous and Therapeutic-Induced Mechanisms of Functional Recovery After Stroke. Transl Stroke Res. 2017;8(1):33-46. [51] WATANABE H, MARUSHIMA A, KADONE H, et al. Efficacy and Safety Study of Wearable Cyborg HAL (Hybrid Assistive Limb) in Hemiplegic Patients With Acute Stroke (EARLY GAIT Study): Protocols for a Randomized Controlled Trial. Front Neurosci. 2021;15:666562. [52] UÇAR DE, PAKER N, BUĞDAYCI D. Lokomat: a therapeutic chance for patients with chronic hemiplegia. NeuroRehabilitation. 2014; 34(3):447-453. [53] BALLESTER BR, MAIER M, DUFF A, et al. A critical time window for recovery extends beyond one-year post-stroke. J Neurophysiol. 2019;122(1):350-357. |
| [1] | Liu Jinlong, Abuduwupuer·Haibier, Bai Zhen, Su Danyang, Miao Xin, Li Fei, Yang Xiaopeng. Efficacy of different nonsurgical treatments for adolescent idiopathic scoliosis: a systematic review and network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(9): 2370-2379. |
| [2] | Cao Xinyan, Yu Zifu, Leng Xiaoxuan, Gao Shiai, Chen Jinhui, Liu Xihua. Effect of repetitive transcranial magnetic stimulation and transcranial direct current stimulation on motor function and gait in children with cerebral palsy: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(6): 1539-1548. |
| [3] | Zheng Yin, Wu Zhenhua, Zhang Cheng, Ruan Kexin, Gang Xiaolin, Ji Hong. Safety and efficacy of immunoadsorption therapy for rheumatoid arthritis: a network meta-analysis and systematic review [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(5): 1260-1268. |
| [4] | Leng Xiaoxuan, Zhao Yuxin, Liu Xihua. Effects of different neuromodulatory stimulation modalities on non-motor symptoms in Parkinson’s patients: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(5): 1282-1293. |
| [5] | Yang Yuanyuan, Zhou Shanshan, Cheng Xiaofei, Feng Luye, Tang Jiqin. Network meta-analysis of non-invasive brain stimulation in the treatment of lower limb motor dysfunction after stroke [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(4): 1008-1018. |
| [6] | Leng Xiaoxuan, Yu Zifu, Cao Xinyan, Gao Shiai, Chen Jinhui, Liu Xihua. Balance function and its influencing factors in patients with post-stroke hemiplegia [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(18): 4611-4617. |
| [7] | Chen Jinhui, Yu Zifu, Gao Shiai, Cao Xinyan, Leng Xiaoxuan, Liu Xihua. Effects of central and peripheral rehabilitation therapies on upper extremity function and activities of daily living in stroke patients: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(17): 4457-4471. |
| [8] | Xu Feng, Gu Dongyang, Zhu Zihao, Li Qiujie, Wan Xianglin. Relationship between spatio-temporal gait characteristics and fall risk in stroke patients [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(16): 4038-4044. |
| [9] | Guo Yuqi, Li Jiacheng, Lu Bowen, Zhang Jiahao, Li Gang. Network meta-analysis of core decompression combined with various therapies for early and mid-stage osteonecrosis of the femoral head [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(15): 3993-4009. |
| [10] | Chen Ping, Du Jinchao, Wang Hongying, Zhang Hui, Wang Haixia. Different inspiratory muscle training methods improve exercise and cardiopulmonary function of patients after cardiac surgery: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(12): 3134-3144. |
| [11] | Cheng Le, Zhu Caifeng, Zhou Bingyuan, Gao Dahong, Cui Xiaoya, Li Jing, Wang Xuewei, Yang Gaoshang, Chen Xiyang. Mechanisms of stroke therapy targeting inflammatory cytokines: a big data analysis based on the IEU Open GWAS [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(12): 3198-3216. |
| [12] | Gao Shiai, Yu Zifu, Chen Jinhui, Cao Xinyan, Leng Xiaoxuan, Liu Xihua. Efficacy of non-invasive neuromodulation techniques on autism spectrum disorder: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(10): 2550-2559. |
| [13] | Zhang Xinxin, Gao Ke, Xie Shidong, Tuo Haowen, Jing Feiyue, Liu Weiguo. Network meta-analysis of non-surgical treatments for foot and ankle ability and dynamic balance in patients with chronic ankle instability [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(9): 1931-1944. |
| [14] | Wang Juan, Wang Guanglan, Zuo Huiwu. Efficacy of exercise therapy in the treatment of anterior cruciate ligament reconstruction patients: #br# a network meta-analysis #br# [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(8): 1714-1726. |
| [15] | Li Zhe, Li Ping, Zhang Chao, Guo Guangling. A network meta-analysis of efficacy of mesenchymal stem cells from different sources in treatment of premature ovarian failure animal models [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(36): 7898-7908. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||