Chinese Journal of Tissue Engineering Research ›› 2019, Vol. 23 ›› Issue (23): 3754-3759.doi: 10.3969/j.issn.2095-4344.1324
Previous Articles Next Articles
Dextrose prolotherapy induces the proliferation of new cells to repair soft tissue and to alleviate pain: current status and problems
Yang Dan, Zhou Jing
- (Hubei University of Chinese Medicine, Wuhan 430061, Hubei Province, China)
-
Received:2019-03-23Online:2019-08-18Published:2019-08-18 -
Contact:Zhou Jing, Master, Associate chief physician, Hubei University of Chinese Medicine, Wuhan 430061, Hubei Province, China -
About author:Yang Dan, Master candidate, Hubei University of Chinese Medicine, Wuhan 430061, Hubei Province, China
CLC Number:
Cite this article
Yang Dan, Zhou Jing. Dextrose prolotherapy induces the proliferation of new cells to repair soft tissue and to alleviate pain: current status and problems[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(23): 3754-3759.
share this article
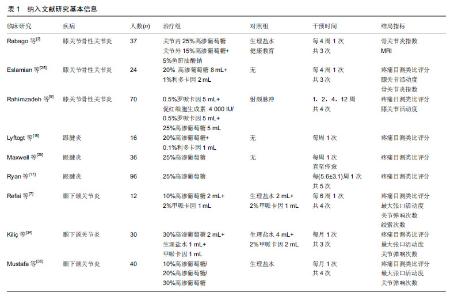
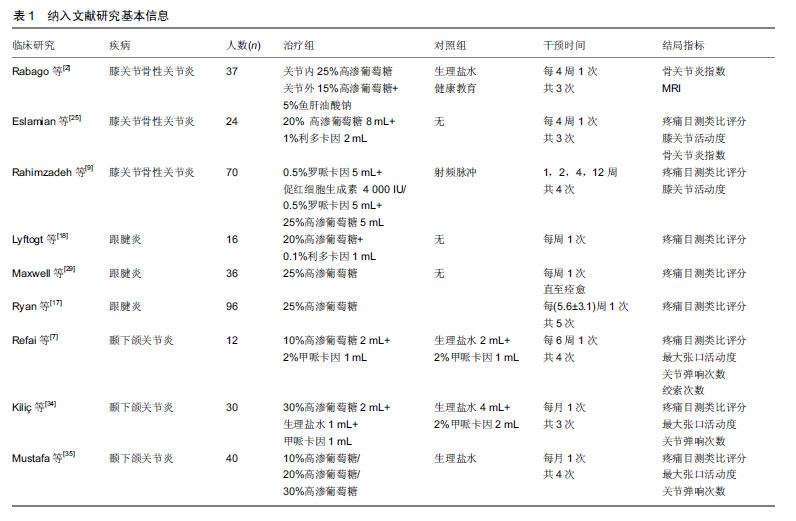
2.1 概念与源流 早在公元前5世纪,Hippocrates(公元前460-370年)就提出“通过刺激或伤害来模拟愈合”的概念。在此期间,他尝试通过铁棒戳扎韧带来治疗不稳定的关节[8]。虽然这个过程只是初步试验性的,但Hippocrates认为继发的炎症会促使局部结缔组织自我修复。到20世纪40年代,美国俄亥俄州的创伤外科医生George S. Hacket, MD引申了韧带损伤、肌腱松弛与慢性肌肉骨骼疼痛的关系[9]。他首次提出“增生治疗(prolotherapy)”的概念[10],其来源于拉丁文“proli-”,意思是后代,即为增殖新细胞。据统计目前此疗法在欧美国家及中国台湾地区正在得到更多的关注[11-13]。 2.2 机制研究进展 2.2.1 直接促进软骨修复 高渗葡萄糖溶液所产生的反应可能对动物模型中骨关节炎的进展和软骨再生有一定的影响。有研究结果表明:高渗葡萄糖是通过组织渗透压和葡萄糖利用率的增加,从而导致软骨细胞增殖及细胞外基质的产生[7]。另外一项临床研究在注射前后关节镜检查和活检的基础上[14],观察了在严重膝关节关节腔内注射高渗葡萄糖可以引起透明和纤维样软骨增生。可聚蛋白多糖在软骨和椎间盘的结构与功能中发挥着重要作用,关节软骨中可聚蛋白多糖降解是早期膝骨性关节炎的一个重要环节,有实验研究通过培养小鼠软骨细胞株ATDC5发现[15],葡萄糖可以通过PKCα-p38- miR141-3p信号通路介导增加ATDC5细胞中可聚蛋白多糖的表达进而促进软骨细胞增殖、分化。 2.2.2 炎症反应释放细胞因子促进纤维化 早期研究结果表明使用高渗葡萄糖糖治疗2周后,在大鼠模型中跟腱的大小和强度会增加[16]。高渗葡萄糖通过包括细胞渗透休克、炎症递质的趋化吸引或宿主细胞抗原性的增加等途径,导致白细胞和巨噬细胞浸润。炎症产生的生长因子(内源性或外源性)会导致新的成纤维细胞生长和胶原沉积[17],从而修复和加强损伤松弛的韧带,增强关节稳定性。 2.2.3 神经血管效应 以目前研究机制来看,高渗、低渗葡萄糖均能在神经病理性疼痛中发挥作用,但在新生血管的增加与减少方面存在争议。 高渗葡萄糖注射导致的炎症反应可能通过减少不适当的新生血管和伴随的神经生长而改善疼痛[18]。此外,还可以沿关节表面进行高渗葡萄糖注射,这种操作技术以浅层神经末梢为靶点,因此被称为神经周注射疗法。在病理学研究中,浅表神经与神经源性炎症有关,这种炎症可以激活1型瞬时电位感受器而导致慢性疼痛和软组织功能障碍。有机制研究发现高渗葡萄糖溶液通过开放钾通道使神经去极化,从而减少伤害性疼痛纤维的传递[19]。有研究表明在这些神经周围注射5%葡萄糖能稳定神经功能,减轻神经源性炎症[20]。此外,低渗溶液被认为是通过阻断1型瞬时电位感受器(一种允许Na+和Ca2+内流的阳离子膜通道)起作用的[21]。钠离子内流可以引发动作电位和伤害性感觉,而钙离子则会导致P物质和降钙素基因相关肽的释放。因此,阻断2种阳离子的内流,理论上可以将神经病理疼痛、水肿和肌间室压力降至最低[22]。相关研究还表明高浓度葡萄糖能上调人滑膜成纤维细胞中血管内皮生长因子A的表达[13],而血管生成对膝骨性关节炎发生发展起重要作用。即软骨下骨的新生血管侵入钙化软骨层及非钙化软骨,激活软骨下骨及骨小梁的重塑过程,进而引发关节软骨的退变[23]。低浓度葡萄糖可以通过上调可聚蛋白多糖表达恢复软骨功能,高浓度葡萄糖通过诱导血管生成促进膝骨性关节炎的形成[24]。 2.3 临床研究进展 2.3.1 高渗葡萄糖注射治疗膝骨性关节炎 膝骨性关节炎的主要病理改变是关节软骨的进行性破坏,软骨下骨质失去软骨的保护而逐渐裸露,从而导致关节的疼痛和运动功能障碍。软骨组织无血管及淋巴,所以损伤软骨的修复和再生能力微乎其微[25]。据报道,高渗葡萄糖治疗因其安全性高,在治疗膝骨性关节炎上具有潜在的治疗作用而倍受关注[25]。Rabago等[25]将37例诊断为膝骨性关节炎的患者随机分为治疗组和对照组,分别在膝关节腔内注射25%葡萄糖,关节外注射15%葡萄糖,并于第13,17周选择性注射5%鱼肝油酸钠。对照组:采用注射生理盐水或给予健康指导。上述2组均每4周注射1次,共治疗3次。2组治疗后的骨关节炎指数(WOMAC)以及在第52周MRI评估的软骨体积值均较治疗前有改善,但治疗组总体疗效优于对照组。Eslamian等[26]观察了24例诊断为膝骨性关节炎的女性患者进行高渗葡萄糖局部注射的疗效,即膝关节内注射20%葡萄糖(8 mL),1%利多卡因(2 mL),每隔4周注射1次,共治疗3次。治疗后患者疼痛目测类比评分(VAS)、膝关节活动度评分、骨关节炎指数(WOMAC)均得到有效改善。Rahimzadeh等[9]将70例诊断为膝骨性关节炎的患者随机分为3组,第1组:关节内注射5 ml罗哌卡因(0.5%)和4 000 IU促红细胞生成素;第2组:关节内注射5 mL 0.5%罗哌卡因+ 5 mL葡萄糖(25%)。第3组:射频脉冲;第1组的疗效在第2,4,12周治疗结束后的疼痛目测类比评分、膝关节活动度评分均高于第2,3组。 综上,高渗葡萄糖增生疗法在治疗膝骨性关节炎可以发挥有效作用。但上述研究样本量小,研究设计不完善,且高渗葡萄糖注射浓度、次数、疗程异质性很大,仅有一项研究测量了软骨体积与功能改善之间的关系。因此关于高渗葡萄糖治疗膝骨性关节炎的临床疗效及安全性评价还需更多高质量的循证医学证据。 2.3.2 高渗葡萄糖注射治疗慢性跟腱炎 无力的韧带和肌键是导致慢性和反复性骨骼肌肉疼痛的重要原因之一,高渗葡萄糖增生疗法则是一种加固和治愈这种无力韧带和肌键的有效方法[27]。Lyftogt等[28]对16例非插入性跟腱炎患者进行了前瞻性研究,以评价高渗葡萄糖治疗慢性跟腱炎的疗效。即皮下注射1 mL(20%葡萄糖+ 0.1%利多卡因),每周注射1次,并随访3个月。有14例患者在治疗结束时疼痛目测类比评分明显下降。Maxwell等[29]观察了36例诊断为慢性跟腱炎的患者在彩色多普勒超声引导下进行25%高渗葡萄糖注射治疗的临床疗效。每6周治疗1次,直至症状缓解或痊愈。研究结果表明治疗结束后的静息疼痛目测类比评分、日常活动疼痛目测类比评分、运动期间疼痛目测类比评分较治疗前明显下降。而在超声评估下,跟腱厚度增加、无回声区范围缩小,但有11条肌腱并未发现新生血管减少。有3例为插入性跟腱炎,超声下评估跟腱附着处皮质不规则,内膜钙化。有1例患者在接受注射过程中无回声区扩大,后转至外科治疗。最终发现高渗葡萄糖疗法可以有效缓解非插入性跟腱疼痛,而治疗插入性跟腱炎疗效不明显。高渗葡萄糖增生疗法缓解疼痛的原因并不局限于新生血管的减少,另外,注射时导致的隐匿性撕裂值得临床关注。Ryan等[30]收集96例病程>6个月的慢性跟腱炎(插入或非插入性)患者,给予25%高渗葡萄糖注射治疗,共治疗5次,每次间隔时间为(5.6±3.1)周,治疗后患者疼痛目测类比评分较前明显下降,超声观察治疗后跟腱低回声区减小、撕裂严重程度降低,新生血管增多。 综上,高渗葡萄糖增生疗法可以有效缓解慢性跟腱炎带来的疼痛不适,提高生活质量。且彩色多普勒超声评估证据表明经高渗葡萄糖治疗后跟腱增厚及低回声区减小,但高渗葡萄糖新生血管效应有待深入研究,以及操作时引起的隐匿性跟腱撕裂,提示超声下引导局部注射是安全性的保证,更是精准医疗的必然要求。 2.3.3 高渗葡萄糖注射治疗颞下颌关节炎 Schultz[31]于1937年首次提出使用高渗葡萄糖治疗颞下颌关节半脱位的方法,因其可以加强颞下颌关节囊和韧带的纤维连接,从而抑制髁突的异常活动,减轻疼痛等不适。虽然目前已经有一些关于高渗葡萄糖治疗颞下颌关节紊乱的临床研究,但主要为个案报道,队列研究,仅有3篇关于高渗葡萄糖与生理盐水为对比的随机对照试验,且研究设计没有达到1级证据的水平[32]。Refai等[33]将12例患者随机分为治疗组和对照组。治疗组采用10%高渗葡萄糖2 mL和2%的甲哌卡因1 mL混合溶液,对照组采用生理盐水(2 mL)和2%甲哌卡因(1 mL)混合溶液,每隔6周注射1次,共注射4次。注射部位分别为:关节囊在乳突窝外侧缘附着处(0.8 mL);关节囊于在髁颈附着处(0.8 mL);颞下颌关节囊内(0.4 mL);上关节间隙抵达颅窝顶与骨膜,与前磨牙相距1 cm(1 mL)。分别于治疗前,每次治疗后,以及随访3个月后进行疼痛目测类比评分、最大张口活动度、关节弹响次数和绞索次数。4次治疗结束后每组患者的疼痛目测类比评分、最大张口活动度、绞索次数均有明显改善,而关节弹响次数无改善。治疗组除最大张口活动度外,其他结局指标在与对照组相比差异无统计学意义。最后得出10%葡萄糖即可有效治疗颞下颌关节紊乱,但仍需大样本研究和长期随访以评价其疗效。Kiliç等[34]为探讨30%高渗葡萄糖增生疗法治疗颞下颌关节紊乱的临床疗效,将30例随机分为试验组和对照组,治疗组30%葡萄糖(2 mL)+生理盐水 (1 mL)+2%阿替卡因或甲哌卡因(1 mL),对照组采用生理盐水(4 mL)+2%阿替卡因或甲哌卡因(2 mL)。每月治疗1次,共治疗3次。2组治疗后疼痛目测类比评分、最大张口活动度、关节弹响次数较治疗前均较前改善,组间对比时,治疗组最大张口活动度改善更明显,但其他结局指标两组差异无统计学意义。最后得出葡糖糖增生疗法在治疗颞下颌关节紊乱并不比安慰剂更有效的结论。Mustafa等[35]将40例患者随机分为10%葡萄糖注射组、20%葡萄糖注射组,30%葡萄糖注射组,生理盐水注射组,每月治疗1次,共治疗4次。各组治疗后颞下颌关节疼痛目测类比评分、最大张口活动度、关节弹响次数均明显下降。此外,在随访过程中无患者出现关节绞索情况,但生理盐水组与各葡萄糖注射组疗效差异无统计学意义,且不同浓度之间疗效差异无统计学意义。另外Refai等[7]观察了用10%高渗葡萄糖治疗61例颞下颌关节紊乱的临床疗效,并随访4年,研究结果表明高渗葡糖糖增生疗法可显著改善由于颞下颌关节紊乱造成的疼痛和相关症状,而不改变X射线下颌关节髁突或关节骨成分的形态。 综上,高渗葡萄糖增生疗法治疗颞下颌关节紊乱的临床疗效不一,仍需大样本的随机对照试验来验证疗效。纳入文献研究细节见表1。 2.4 注意事项、相关禁忌证与不良反应 在注射前3 d,患者应避免服用非类固醇类抗炎药物(如布洛芬、萘普生)。因为增生疗法的目的是引起炎症,促进愈合,而非类固醇类抗炎药物能阻止炎症[2]。一般在50%葡萄糖中加入局部麻醉剂和无菌水或生理盐水,稀释成5%-25%的浓度。注射点数取决于围绕该关节的韧带和肌键的损伤范围,以体格检查为依据。采用23-25号小针头,向组织内缓慢推进,抵达骨面时开始注射,每个注射点注射体积一般不超过1 mL[23]。注射深度为韧带或肌腱抵于骨膜连接处或关节腔内。每次注射间隔时间为2-8周,根据患者症状体征决定治疗疗程,在注射间隔时间内可以配合适当功能锻炼[36]。 高渗葡萄糖增生疗法的禁忌证包括非肌肉骨骼性疼痛、转移癌、化脓性关节炎、蜂窝织炎、脊柱先天结构异常、病理性肥胖、出血障碍、痛阈过低或不明性质的疼痛[3]。 高渗葡萄糖增生疗法不良反应为[37]:可能在12- 96 h内,注射局部出现暂时性疼痛、僵硬感、淤青、隐匿性肌腱撕裂等。其他可能出现的不良反应包括头痛,或对药物有轻微过敏反应。罕见报道不良反应包括硬膜外脓肿、肺塌陷、椎间盘损伤、脑膜炎、出血和神经损伤[23]。另外有学者提出在糖尿病患者中,局部葡萄糖浓度过高会导致某些细胞蛋白质的非酶促糖基化[37],影响细胞代谢功能的假说。"
| [1]Fullerton BD.Prolotherapy for the Thoracolumbar Myofascial System. Phys Med RehabilClin N Am.2018, 29(1):125-138.[2]Rabago D,Nourani B.Prolotherapy for Osteoarthritis and Tendinopathy: a Descriptive Review. Curr Rheumatol Rep. 2017; 19(6):34.[3]Sanderson LM, Bryant A. Effectiveness and safety of prolotherapy injections for management of lower limb tendinopathy and fasciopathy: a systematic review. J Foot Ankle Res. 2015 ;8:57. [4]Nourani B,Rabago D. Prolotherapy for Knee Osteoarthritis: A Descriptive Review. Curr Phys Med Rehabil Rep.2016; 4(1):42-49.[5]Derakhshan P . What is the role of erythropoietin prolotherapy on pain relief of knee osteoarthritis?. J Res Med Sci. 2018 6;23:50.[6]Ryu K, Ko D, Lim G,et al.Ultrasound-Guided Prolotherapy with Polydeoxyribonucleotide for Painful Rotator Cuff Tendinopathy. Pain Res Manag. 2018;2018:8286190..[7]Refai H.Long-term therapeutic effects of dextrose prolotherapy in patients with hypermobility of the temporomandibular joint: a single-arm study with 1-4 years’ follow up. Br J Oral Maxillofac Surg. 2017;55(5):465-470.[8]Rabago D, Slattengren A, Zgierska A. Prolotherapy in Primary Care Practice. Prim Care. 2010;37(1):65-80.[9]Rahimzadeh P, Imani F, Faiz SH, et al. Investigation the efficacy of intra-articular prolotherapy with erythropoietin and dextrose and intra-articular pulsed radiofrequency on pain level reduction and range of motion improvement in primary osteoarthritis of knee. J Res Med Sci. 2014;19(8):696-702.[10]Park YS, Lim SW, Lee IH, et al. Intra-articular injection of a nutritive mixture solution protects articular cartilage from osteoarthritic progression induced by anterior cruciate ligament transection in mature rabbits: a randomized controlled trial. Arthritis Res Ther. 2007;9(1):R8.[11]Jensen KT, Rabago DP, Best TM, et al. Early inflammatory response of knee ligaments to prolotherapy in a rat model. J Orthop Res. 2008;26(6):816-823.[12]Chan O, Havard B, Morton S, et al. Outcomes of prolotherapy for intra-tendinous Achilles tears: a case series. Muscles Ligaments Tendons J. 2017 ;7(1):78-87.[13]Wu TJ,Fong YC,Lin CY,et al.Glucose enhances aggrecan expression in chondrocytes via the PKCα/p38-miR141-3p signaling pathway. J Cell Physiol. 2018;233(9):6878-6887.[14]Derby B M ,Reichensperger J , Chambers C , et al. Early Growth Response Factor-1: Expression in a Rabbit Flexor Tendon Scar Model. Plast Reconstr Surg. 2012;129(3):435e-442e. [15]Hoksrud A,Ohberg L,Alfredson H,et al.Ultrasound-guided sclerosis of neovessels in painful chronic patellar tendinopathy: a randomized controlled trial. Am J Sports Med. 2006;34(11):1738-1746.[16]Burdakov D, Jensen L T, Alexopoulos H, et al. Tandem-Pore K +, Channels Mediate Inhibition of Orexin Neurons by Glucose. Neuron. 2006;50(5):711-722.[17]Ryan M, Wong A. Ultrasound-guided injections of hyperosmolar dextrose for overuse patellar tendinopathy: a pilot study.Br J Sports Med.2011;45(12):972-977.[18]Lyftogt J. Subcutaneous prolotherapy treatment of refractory knee, shoulder, and lateral elbow pain. Australasian Musculoskeletal Medicine. 2007; 12(2):202-210.[19]Veronesi B,Oortgiesen M.Neurogenic Inflammation and Particulate Matter (PM) Air Pollutants. Neurotoxicology, 2001; 22(6):795-810.[20]Tsai CH, Chiang YC, Chen HT, et al. High glucose induces vascular endothelial growth factor production in human synovial fibroblasts through reactive oxygen species generation. Biochim Biophys Acta. 2013;1830(3):2649-2658.[21]Ashraf S, Walsh DA. Angiogenesis in osteoarthritis. Curr Opin Rheumatol. 2008;20(5):573-580.[22]Ismail HM, Yamamoto K, Vincent TL, et al. Interleukin-1 Acts via the JNK-2 Signaling Pathway to Induce Aggrecan Degradation by Human Chondrocytes. Arthritis Rheumatol. 2015;67(7):1826-1836.[23]Dagenais S,Ogunseitan O,Haldeman S, et al. Side Effects and Adverse Events Related to Intraligamentous Injection of Sclerosing Solutions (Prolotherapy) for Back and Neck Pain: A Survey of Practitioners. Arch Phys Med Rehabil. 2006;87(7):909-913.[24]Vora A,Borg-Stein J, Nguyen R T. Regenerative injection therapy for osteoarthritis: fundamental concepts and evidence-based review. PM R. 2012;4(5 Suppl):S104-S109.[25]Rabago D,Kijowski R, Woods M, et al. Association between disease-specific quality-of-life and magnetic resonance imaging outcomes in a clinical trial of prolotherapy for knee osteoarthritis. Arch Phys Med Rehabil. 2013;94(11):2075-2082.[26]Eslamian F, Amouzandeh B. Therapeutic effects of prolotherapy with intra-articular dextrose injection in patients with moderate knee osteoarthritis: a single-arm study with 6 months follow up. Ther Adv Musculoskelet Dis. 2015;7(2):35-44.[27]Jean-Paul Ouellette,Jeffrey J.Patterson,George Yu,许涛. 增生疗法[J]. 实用疼痛学杂志,2006,2(1):3-9.[28]Lyftogt J. Prolotherapy and Achilles tendinopathy: a prospective pilot study of an old treatment. Australasian Musculoskeletal Medicine. 2005;10(1):12-16.[29]Maxwell NJ, Ryan MB, Taunton JE, et al. Sonographically Guided Intratendinous Injection of Hyperosmolar Dextrose to Treat Chronic Tendinosis of the Achilles Tendon: A Pilot Study. Ajr Am J Roentgenol. 2007; 189(4):215-220.[30]Ryan M,Wong A,Taunton J.Favorable Outcomes After Sonographically Guided Intratendinous Injection of Hyperosmolar Dextrose for Chronic Insertional and Midportion Achilles Tendinosis. AJR Am J Roentgenol. 2010;194(4):1047-1053.[31]Schultz LW. A Treatment for subluxation of the Temporomandibular Joint. JAMA.1937; 109(12):1947-1950.[32]Nagori SA, Jose A, Gopalakrishnan V, et al. Roy ID The efficacy of dextrose prolotherapy over placebo for temporomandibular joint hypermobility: a systematic review and meta-analysis. J Oral Rehabil. 2018;45(12):998-1006.[33]Refai H,Altahhan O,Elsharkawy R.The efficacy of dextrose prolotherapy for temporomandibular joint hypermobility: a preliminary prospective, randomized, double-blind, placebo- controlled clinical trial.J Oral Maxillofac Surg. 2011;69(12): 2962-2970.[34]Kiliç SC, Güngörmü? M. Is dextrose prolotherapy superior to placebo for the treatment of temporomandibular joint hypermobility? A randomized clinical trial. Int J Oral Maxillofac Surg. 2016;45(7): 813-819.[35]Mustafa R,Güngörmü? M,Mollao?lu N.Evaluation of the Efficacy of Different Concentrations of Dextrose Prolotherapy in Temporomandibular Joint Hypermobility Treatment. J Craniofac Surg. 2018;29(5):e461-e465.[36]Umlauf D,Frank S,Pap T,et al.Cartilage biology, pathology, and repair. Cell Mol Life Sci. 2010;67(24):4197-4211.[37]Clifton T,Selby M.Epidural abscess from prolotherapy: a cautionary tale. ANZ J Surg. 2018;88(3):E216-E217. .[38]刘伟,陈世荣.不同支架材料与间充质干细胞构建组织工程韧带在前交叉韧带损伤中的应用[J]. 中国组织工程研究, 2011,15(38):7181-7184.[39]侯存强,周宪华,孙磊. 骨骼肌对前交叉韧带重建腱性移植物关节内愈合效果的影响[J].中国骨科临床与基础研究杂志, 2012,4(2):133-137.[40]Sahr M, Sturnick DR, Nwawka OK. Quantitative Ultrasound Assessment of the Achilles Tendon Under Varied Loads. J Ultrasound Med. 2018;(3):13-23. |
| [1] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Comparison of the short-term efficacy of extracorporeal shock wave therapy for middle-aged and elderly knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1471-1476. |
| [2] | Li Dadi, Zhu Liang, Zheng Li, Zhao Fengchao. Correlation of total knee arthroplasty efficacy with satisfaction and personality characteristics [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1346-1350. |
| [3] | Wei Wei, Li Jian, Huang Linhai, Lan Mindong, Lu Xianwei, Huang Shaodong. Factors affecting fall fear in the first movement of elderly patients after total knee or hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1351-1355. |
| [4] | Lü Zhen, Bai Jinzhu. A prospective study on the application of staged lumbar motion chain rehabilitation based on McKenzie’s technique after lumbar percutaneous transforaminal endoscopic discectomy [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1398-1403. |
| [5] | Gao Yan, Zhao Licong, Zhao Hongzeng, Zhu Yuanyuan, Li Jie, Sang Deen. Alteration of low frequency fluctuation amplitude at brain-resting state in patients with chronic discogenic low back pain [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1160-1165. |
| [6] | Wu Gang, Chen Jianwen, Wang Shilong, Duan Xiaoran, Liu Haijun, Dong Jianfeng. Simple HyProCure subtalar stabilization in treatment of adolescent flexible flatfoot combined with painful accessory navicular bone [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 901-905. |
| [7] | Li Yan, Wang Pei, Deng Donghuan, Yan Wei, Li Lei, Jiang Hongjiang. Electroacupuncture for pain control after total knee arthroplasty: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 957-963. |
| [8] | Zhao Zhongyi, Li Yongzhen, Chen Feng, Ji Aiyu. Comparison of total knee arthroplasty and unicompartmental knee arthroplasty in treatment of traumatic osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 854-859. |
| [9] | Zhang Nianjun, Chen Ru. Analgesic effect of cocktail therapy combined with femoral nerve block on total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 866-872. |
| [10] | Li Quanxi, Shen Yu, Wan Wei, Sun Shanzhi. Changes of abdominal wall mechanics and pain after tension-free inguinal hernia repair with polypropylene mesh [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 548-552. |
| [11] | Zhang Xinchao, Wang Bingnan, Ge Zhe. Monoclonal antibody therapy for osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(32): 5171-5177. |
| [12] | Huang Cihui, Liu Jiayue, Huang Yingjie, Zhuang Zeqin, Lin Yunxin, Li Dan, Zheng Liang. Clinical efficacy of small needle knife combined with traditional Chinese medicine in the treatment of knee osteoarthritis: a network Meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(32): 5240-5248. |
| [13] | Chen Hongqiang, Zhou Hua, Chen Debin, Wu Xizhi, Wu Dewei, Zhao Bin. Gap balance technology can reduce the amount of osteotomy and maintain the balance of lower limb alignment and flexion and extension gap in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(30): 4828-4832. |
| [14] | Wang Xiaofei, Teng Xueren, Cong Linyan, Zhou Xu, Ma Zhenhua. Herbert screw internal fixation for treating adult osteochondritis dissecans of the knees [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 397-402. |
| [15] | Tang Shuo, Hou Decai. Constructing an animal model of femoral head necrosis: how to get closer to clinical application [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(29): 4691-4696. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||