Chinese Journal of Tissue Engineering Research ›› 2018, Vol. 22 ›› Issue (3): 486-492.doi: 10.3969/j.issn.2095-4344.0051
Analgesic effect of femoral nerve block versus adductor canal block after total knee arthroplasty: a meta-analysis
Wang Yin, Wang Xing-bo, Guo Shi-fang, Yang Qing-shan, Chen Zhi-xin
- First Department of Orthopedics, Gansu Provincial Hospital, Lanzhou 730000, Gansu Province, China
-
Online:2018-01-28Published:2018-01-28 -
Contact:Chen Zhi-xin, M.D., Chief physician, First Department of Orthopedics, Gansu Provincial Hospital, Lanzhou 730000, Gansu Province, China -
About author:Wang Yin, Master, Attending physician, First Department of Orthopedics, Gansu Provincial Hospital, Lanzhou 730000, Gansu Province, China
CLC Number:
Cite this article
Wang Yin, Wang Xing-bo, Guo Shi-fang, Yang Qing-shan, Chen Zhi-xin. Analgesic effect of femoral nerve block versus adductor canal block after total knee arthroplasty: a meta-analysis[J]. Chinese Journal of Tissue Engineering Research, 2018, 22(3): 486-492.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks

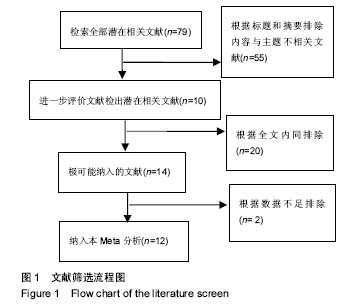
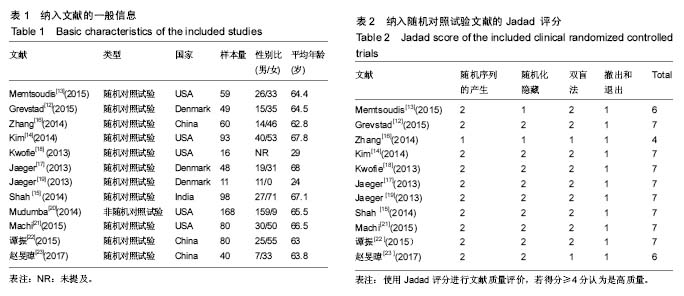
2.1 检索结果 初步检索到文献79篇。通过阅读题目和摘要,剔除综述、题目与研究不相符和未涉及评价指标的文献共65篇,全文阅读其余14篇,排除2篇不能获得完整数据的文献,最终纳入12篇文献[12-23],文献检索流程见图1,其中中文文献2篇,英文文献10篇,文献基本特征信息见表1。12篇文献共计802例患者(872膝):收肌管阻滞组414膝,股神经阻滞组458膝。其中11篇随机对照试验采用Jadad量表进行评分(最低4分,最高7分,平均分为6.64分,表2),非随机对照试验进行MINORS文献偏倚分析(表3)。发表偏倚用漏斗图直观评价。"

"

"
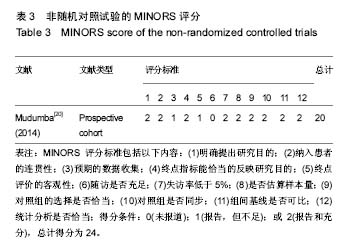

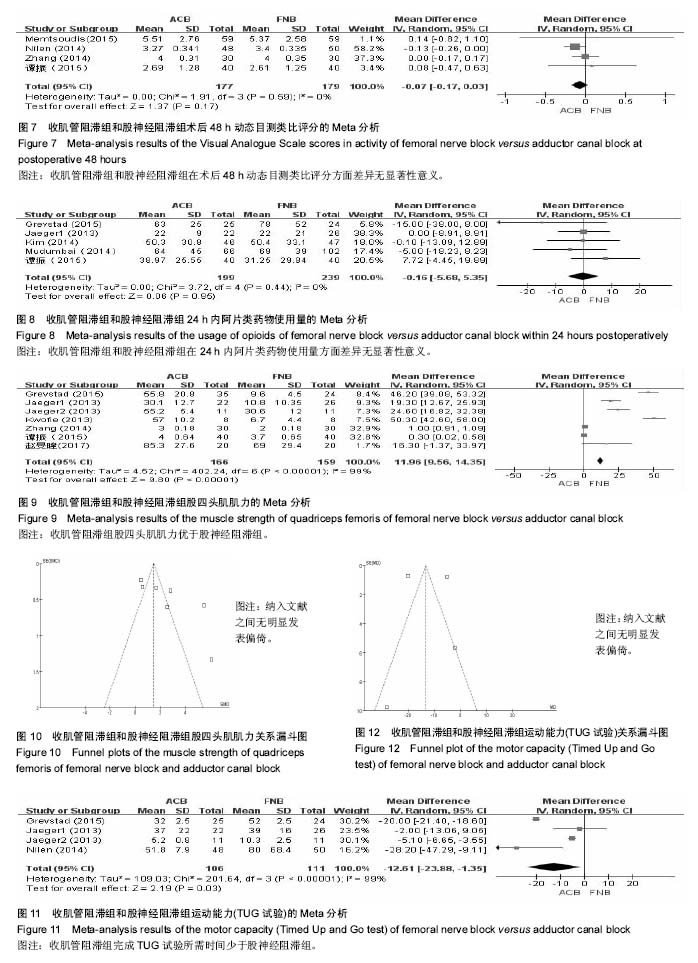
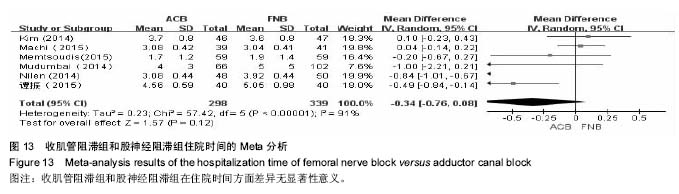
2.2 静息目测类比评分 Meta分析结果显示,5篇文献中418膝在术后8 h静息目测类比疼痛评分中发现收肌管阻滞组和股神经阻滞组之间差异有显著性意义[12-16] (MD=-0.17,95%CI为-0.27至-0.07,I2=85%,见图2)。8项研究报道了745例患肢术后24 h的静息目测类比疼痛评分[13-17,20-22](MD=-0.05,95%CI为-0.53至0.43,I2=90%,见图3),7项研究报道了697例患肢在术后48 h的静息目测类比疼痛评分[13-16,20-22](MD=-0.05,95%CI为-0.14至0.04,I2=0%,见图4),2组之间差异均无显著性意义。 2.3 动态目测类比评分 研究表明,仅3篇文献227 膝[12-13,16]、4篇文献306膝[13,16-17,22]和4篇文献356 膝[13,15-16,22],分别报道了术后8,24,48 h动态目测类比疼痛评分。结果显示,收肌管阻滞组和股神经阻滞组之间差异均无显著性意义(MD=0,95% CI为-0.09至0.09,I2=0%,见图5;MD=0.03,95%CI为-0.12至0.18,I2=45%,见图6;MD=-0.07,95% CI为-0.17至0.03,I2=0%,见图7)。 2.4 阿片类药物累计使用量 5篇文献包含438膝评估了阿片类药物24 h内累计使用量[12,4,17,20,22],结果显示2组差异无显著性意义(MD=-0.16,95%CI为-5.68至5.35,I2=0%,见图8)。 2.5 股四头肌肌力 7篇文献325膝测评了评估了股四头肌肌力[12,16-19,22-23],Meta分析表明,股四头肌肌力在收肌管阻滞组均远大于股神经阻滞组(MD=11.96,95%CI为9.56至14.35,I2=99%,见图9,10)。 2.6 活动能力(TUG试验) 仅4篇文献中总计217膝为评价术后活动能力进行了TUG试验[12,15,17,19],分析发现收肌管阻滞组所需时间小于股神经阻滞组(MD=-12.61,95% CI为-23.88至-1.35,I2=99%,见图11,12)。 2.7 住院时间 对6篇文献中总计637膝的住院时间进行了分析[13-15,20-22],结果发现在收肌管阻滞组与股神经阻滞组的住院时间差异无显著性意义(MD=-0.34,95%CI为-0.76至0.08,I2=91%,见图13)。"


"

"
| [1] Merle-Vincent F, Couris CM, Schott AM, et al. Factors predicting patient satisfaction 2 years after total knee arthroplasty for osteoarthritis. Joint Bone Spine. 2011;78(4): 383-386.[2] Skinner HB, Shintani EY. Results of a multimodal analgesic trial involving patients with total hip or total knee arthroplasty.Am J Orthop. 2004;33(2):85-92.[3] Chan EY, Fransen M, Sathappan S, et al. Comparing the analgesia effects of single-injection and continuous femoral nerve blocks with patient controlled analgesia after total knee arthroplasty. J Arthroplasty. 2013;28(4):608-613.[4] Brian M, Jonathan J, Douglas W, et al. ong-Term Pain,Stiffness, and Functional Disability Following Total Knee Arthroplasty With and Without an Extended Ambulatory Continuous Femoral Nerve Block: A Prospective, One-Year Follow-Up of a Multicenter, Randomized, Triple-Masked, Placebo-Controlled Trial. Reg Anesth Pain Med. 2011;36(2):116-120.[5] 彭周全,张卫,李丽伟.股神经阻滞对全身麻醉下全膝置换患者炎性反应的影响[J].中华实验外科杂志,2014,12(31):2789.[6] Wasserstein D, Farlinger C, Brull R, et al. Advanced age, obesity and continuous femoral nerve blockade are independent risk factors for inpatient falls after primary total knee arthroplasty. J Arthroplasty. 2013;28(7): 1121-1124.[7] Sharma S, Iorio R, Specht LM, et al Complications of femoral nerve block for total knee arthroplasty. Clin Orthop Relat Res. 2010;468(1): 135-140.[8] Teo EY,Ang CL,Sathappan SS.A variant of patellar clunk syndrome after bilateral total knee arthroplasty: clinical manifestations and arthroscopic images.Orthop Surg. 2014;4(6):326-328.[9] Jin SQ, Ding XB, Tong YE. ffect of saphenous nerve block for post-operative pain on knee surgery: a meta-analysis. Int J Clin Exp Med. 2015;8:368-376.[10] Hanson NA, Allen CJ, Hostetter LS, et al.Continuous ultrasound-guided adductor canal block for total knee arthroplasty: a randomized, double-blind trial. Anesth Analg. 2014;118:1370-1377.[11] Jæger P, Koscielniak-Nielsen ZJ. Adductor canal block for post-operative pain treatment after revision knee arthroplasty: a blinded, randomized, placebo-controlled study. PLoS One. 2014;9: e111951.[12] Grevstad U, Mathiesen O, Valentiner LS, et al. Effect of adductor canal block versus femoral nerveblock on quadriceps strength,mobilization, and pain after total knee arthroplasty: a randomized, blinded study. Reg Anesth Pain Med. 2015;40:3-10.[13] Memtsoudis SG, Yoo D, Stundner O, et al. Subsartorial adductor canal vs femoral nerve block for analgesia after total knee replacement. Int Orthop. 2015;39:673-680.[14] Kim DH, Lin Y, Goytizolo EA, et al.Adductor canal block versus femoral nerve block for total knee arthroplasty: a prospective, randomized, controlled trial. Anesthesiology. 2014;120:540-550.[15] Shah NA, Jain NP.Is continuous adductor canal block better than continuous femoral nerve block after total knee arthroplasty? Effect on ambulation ability, early functional recovery and pain control: a randomized controlled trial. J Arthroplast.2014;29:2224-2229.[16] Zhang W, Hu Y, Tao Y, et al. Ultrasound-guided continuous adductor canal block for analgesia after total knee replacement. Chin Med J (Engl).2014;127:4077-4081.[17] Jaeger P, Zaric D, Fomsgaard JS, et al.Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty: a randomized, double-blind study. Reg Anesth Pain Med.2013;38:526-532.[18] Kwofie MK, Shastri UD, Gadsden JC, et al. The effects of ultrasound-guided adductor canal block versus femoral nerve block on quadriceps strength and fall risk: a blinded, randomized trial of volunteers. Reg Anesth Pain Med.2013;38:321-325.[19] Jaeger P, Nielsen ZJ, Henningsen MH, et al. Adductor canal block versus femoral nerve block and quadriceps strength a randomized, double-blind, placebo-controlled, crossover study in healthy volunteers. Anesthesiology. 2013;118:409-415.[20] Mudumbai SC, Kim TE, Howard SK, et al. Continuous adductor canal blocks are superior to continuous femoral nerve blocks in promoting early ambulation after TKA. Clin Orthop Relat Res. 2014;472:1377-1383.[21] Machi AT, Sztain JF, Kormylo NJ, et al. Discharge Readiness after Tricompartment Knee Arthroplasty: Adductor Canal versus Femoral Continuous Nerve Blocks-A Dual-center, Randomized Trial. Anesthesiology.2015;123:444-456.[22] 谭振,康鹏德,裴福兴, 等.多模式镇痛下收肌管与股神经阻滞在全膝关节置换术后初期镇痛及早期康复中的作用[J].中华骨科杂志,2015, 35(9): 914-920.[23] 赵旻暐,王宁,田华,等.膝关节置换术后连续收肌管阻滞与股神经阻滞的疗效比较[J].北京大学学报(医学版), 2017,49(1):142-147.[24] Pelt CE, Anderson AW, Anderson MB, et al.Postoperative falls after total knee arthroplasty in patients with a femoral nerve catheter: can we reduce the incidence? J Arthroplasty. 2014;29(6):1154-1157.[25] Wasserstein D, Farlinger C, Brull R, et al.Advanced age, obesity and continuous femoral nerve blockade are independent risk factors for inpatient falls after primary total knee arthroplasty. J Arthroplasty. 2013;28(7): 1121-1124.[26] Sharma S, Iorio R, Specht LM, et al.Complications of femoral nerve block for total knee arthroplasty. Clin Orthop Relat Res. 2010;468(1): 135–140.[27] Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol.2005;5:13.[28] Rasmussen M, Kim E, Kim T, et al.A retrospective comparative provider workload analysis for femoral nerve and adductor canal catheters following knee arthroplasty. J Anesth.2015;29:303-307.[29] Patterson ME, Bland KS, Thomas LC, et al. The adductor canal block provides effective analgesia similar to a femoral nerve block in patients undergoing total knee arthroplasty–a retrospective study. J Clin Anesth. 2015;27:39-44.[30] 吴丹冬,陈虹,黄伟,等.持续股神经阻滞与患者自控静脉镇痛对人工全膝关节置换术后康复的影响[J].中华创伤杂志, 2015,5(31):435-438. |
| [1] | Zhang Yu, Tian Shaoqi, Zeng Guobo, Hu Chuan. Risk factors for myocardial infarction following primary total joint arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1340-1345. |
| [2] | Li Dadi, Zhu Liang, Zheng Li, Zhao Fengchao. Correlation of total knee arthroplasty efficacy with satisfaction and personality characteristics [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1346-1350. |
| [3] | Wei Wei, Li Jian, Huang Linhai, Lan Mindong, Lu Xianwei, Huang Shaodong. Factors affecting fall fear in the first movement of elderly patients after total knee or hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1351-1355. |
| [4] | Wang Jinjun, Deng Zengfa, Liu Kang, He Zhiyong, Yu Xinping, Liang Jianji, Li Chen, Guo Zhouyang. Hemostatic effect and safety of intravenous drip of tranexamic acid combined with topical application of cocktail containing tranexamic acid in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1356-1361. |
| [5] | Xiao Guoqing, Liu Xuanze, Yan Yuhao, Zhong Xihong. Influencing factors of knee flexion limitation after total knee arthroplasty with posterior stabilized prostheses [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1362-1367. |
| [6] | Huang Zexiao, Yang Mei, Lin Shiwei, He Heyu. Correlation between the level of serum n-3 polyunsaturated fatty acids and quadriceps weakness in the early stage after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1375-1380. |
| [7] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [8] | Yuan Jiawei, Zhang Haitao, Jie Ke, Cao Houran, Zeng Yirong. Underlying targets and mechanism of Taohong Siwu Decoction in prosthetic joint infection on network pharmacology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1428-1433. |
| [9] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [10] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Comparison of the short-term efficacy of extracorporeal shock wave therapy for middle-aged and elderly knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1471-1476. |
| [11] | Zhong Hehe, Sun Pengpeng, Sang Peng, Wu Shuhong, Liu Yi. Evaluation of knee stability after simulated reconstruction of the core ligament of the posterolateral complex [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 821-825. |
| [12] | Zhao Zhongyi, Li Yongzhen, Chen Feng, Ji Aiyu. Comparison of total knee arthroplasty and unicompartmental knee arthroplasty in treatment of traumatic osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 854-859. |
| [13] | Liu Shaohua, Zhou Guanming, Chen Xicong, Xiao Keming, Cai Jian, Liu Xiaofang. Influence of anterior cruciate ligament defect on the mid-term outcome of fixed-bearing unicompartmental knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 860-865. |
| [14] | Zhang Nianjun, Chen Ru. Analgesic effect of cocktail therapy combined with femoral nerve block on total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 866-872. |
| [15] | Yuan Jun, Yang Jiafu. Hemostatic effect of topical tranexamic acid infiltration in cementless total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 873-877. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||