Chinese Journal of Tissue Engineering Research ›› 2016, Vol. 20 ›› Issue (53): 7909-7916.doi: 10.3969/j.issn.2095-4344.2016.53.001
Detection and analysis of serum metal ions concentration level after metal-to-metal hip arthroplasty
Cui Peng1, Jiang Wen-xue2, Fan Meng2, Wan Yan-lin2
- 1Department of Orthopedics, Tianjin Hospital, Tianjin 300211, China; 2Department of Orthopedics, Tianjin First Center Hospital, Tianjin 300192, China
-
Revised:2016-10-17Online:2016-12-23Published:2016-12-23 -
Contact:Jiang Wen-xue, Ph.D., Professor, Master’s supervisor, Department of Orthopedics, Tianjin First Center Hospital, Tianjin 300192, China -
About author:Cui Peng, Master, Resident physician, Department of Orthopedics, Tianjin Hospital, Tianjin 300211, China
CLC Number:
Cite this article
Cui Peng, Jiang Wen-xue, Fan Meng, Wan Yan-lin. Detection and analysis of serum metal ions concentration level after metal-to-metal hip arthroplasty[J]. Chinese Journal of Tissue Engineering Research, 2016, 20(53): 7909-7916.
share this article
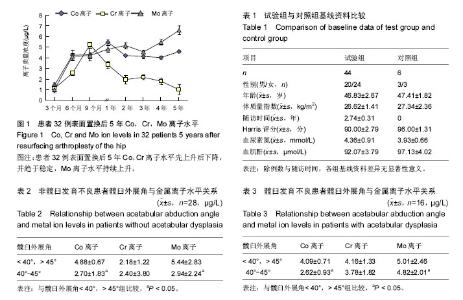
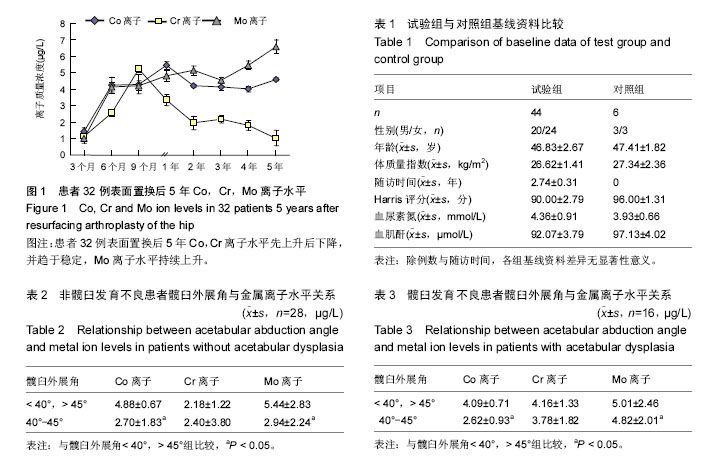
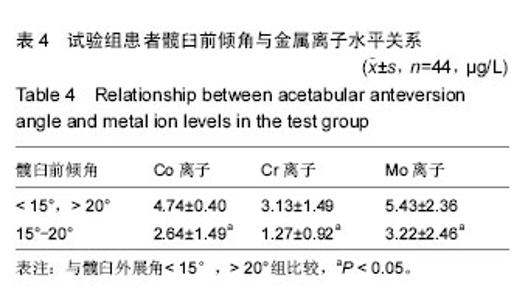
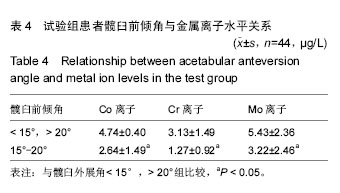
2.1 受试者数量分析 纳入髋关节表面置换者32例,全髋置换者12例,正常对照组6例,共计50例均进入结果分析,无中途退出者。 2.2 受试者基线分析 见表1。 2.3 不同时间血清金属离子水平 6例正常人血清Co质量浓度平均为0.71 μg/L;Cr质量浓度平均为00.73 μg/L;Mo质量浓度平均为00.84 μg/L。作为3种金属离子水平的基础参照值。表面置换患者32例体内金属离子水平均较正常值显著升高,Co离子水平于置换后1年到达顶峰,平均为0 (5.46±0.31) μg/L,较正常值高7.7倍(P < 0.01), 后缓慢下降,至置换后4年较正常值高5.6倍(4.00± 0.26) μg/L情况下再次升高,置换后5年高6.3倍(4.60± 0.42) μg/L,接近置换后2年(4.19±0.29) μg/L水平。 Cr离子水平持续升高,于置换后9个月到达顶峰,平均(5.37±1.01) μg/L,为正常值7.5倍(P < 0.01),后逐渐下降,置换后5年平均(1.00±0.04) μg/L,接近正常水平(P > 0.05)。 Mo离子水平稍有起伏,总体为上升趋势,置换后5年平均(6.54±0.54) μg/L,为正常7.8倍(P < 0.01)。较正常均呈现显著的高值(图1)。 全髋置换后5年Co、Cr离子水平分别为平均(7.12±0.97) μg/L,(6.79±1.03) μg/L,分别为正常值9.8倍和8.2倍,明显高于正常值(P < 0.01),但与表面置换后离子水平无明显统计学差异(P > 0.05),Mo离子水平接近正常(P > 0.05)。 2.4 金属离子水平与髋臼假体位置的关系 测量所有髋臼假体前倾角及外展角,与相应金属离子水平分组比较。髋臼发育不良患者髋臼及股骨侧术前可能存在比较大的畸形及股骨头的脱位,故术前髋臼大部分患者已存在较大形变,假体位置需做出相应调整,共计16例髋臼发育不良患者,髋臼假体外展角处于45°-50°时Co、Mo离子水平较< 45°或> 50°时显著降低(P < 0.05),Cr未见明显变化,28例非髋臼发育不良患者Co离子水平于外展角处于40°-45°时较低前倾角处于10°-20°时各金属离子水平明显较低(P < 0.05),不同前倾角间3种金属离子水平未见明显差异(表2-4)。 2.5 金属离子水平与股骨头假体直径的关系 金属对金属界面假体均为大头假体,但假体设计不同,表面置换与全髋置换股骨头直径行按术式分组,行组内分段对比。表面置换假体股骨头直径最小40 mm,最大 52 mm,以2 mm为组距分组对比,相邻两组间未出现明显差异。股骨头直径大于48 mm时,Co离子平均(4.02±2.12) μg/L,低于股骨头直径小于48 mm时(5.73±2.34) μg/L的平均值(P=0.045)。Cr,Mo离子水平不同直径间未见明显差异。全髋假体股骨头直径最小 44 mm,最大54 mm,以2 mm为组距分组对比,并以48 mm为界,未出现明显统计学差异。 "
"
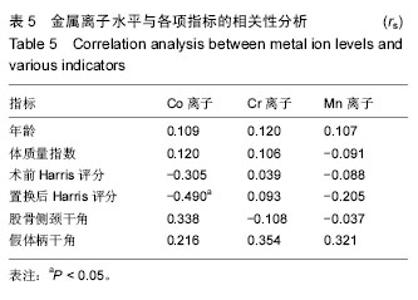
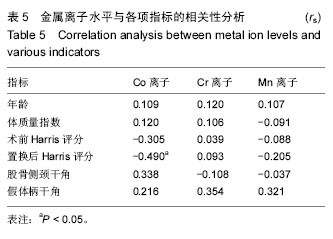
2.6 金属离子水平与试验组患者年龄、性别、体质量指数、Harris评分及股骨侧假体位置的关系 患者Co,Cr,Mo离子水平与年龄,性别,体质量指数,术前Harris、颈干角、外展角未见明显相关性(P > 0.05),Co离子与置换后Harris评分存在负相关(rs=-0.490,P=0.039)(表5)。"
| [1] 姜文学,尤佳,李轶津,等.髋关节表面置换的近期疗效及其并发症分析[J].中华骨科杂志,2009,29(9):858-863.[2] 王晓永,张卫国,吕德成,等.金属对金属全髋关节置换与全膝关节置换后早期钴铬钼离子的释出[J].中华骨科杂志, 2009,29(10):920-923.[3] Back DL, Young DA, Shimmin AJ. How do serum cobalt and chromium levels change after metal-on-metal hip resurfacing? Clin Orthop Relat Res. 2005;438:177-181.[4] Kim PR, Beaulé PE, Dunbar M, et al. Cobalt and chromium levels in blood and urine following hip resurfacing arthroplasty with the Conserve Plus implant. J Bone Joint Surg Am. 2011;93(2):107-117.[5] Daniel J, Ziaee H, Pradhan C, et al. Blood and urine metal ion levels in young and active patients after Birmingham hip resurfacing arthroplasty: four-year results of a prospective longitudinal study. J Bone Joint Surg Br. 2007;89(2):169-173.[6] Silverman Edward J, Blair A, Sheth Neil P. Metal-on-metal total hip arthroplasty: is there still a role in 2016? 2016;9(1):93-96.[7] Moroni A, Savarino L, Hoque M, et al. Do ion levels in hip resurfacing differ from metal-on-metal THA at midterm? Clin Orthop Relat Res. 2011;469(1): 180-187.[8] Visuri T, Borg H, Pulkkinen P, et al. A retrospective comparative study of mortality and causes of death among patients with metal on metal and metal on polyethylene total hip prostheses in primary osteoarthritis after a long term follow up. BMC Musculoskelet Disord. 2010;11:78.[9] Khan M, Takahashi T, Kuiper JH, et al. Current in vivo wear of metal-on-metal bearings assessed by exercise-related rise in plasma cobalt level. J Orthop Res. 2006;24(11):2029-2035.[10] Heisel C, Silva M, Skipor AK, et al. The relationship between activity and ions in patients with metal-on-metal bearing hip prostheses. J Bone Joint Surg Am. 2005;87(4):781-787.[11] Shahrdar C, Campbell P, Mirra J, et al. Painful metal-on-metal total hip arthroplasty. J Arthroplasty. 2006;21(2):289-293.[12] Reito A, Puolakka T, Elo P, et al. Outcome of Birmingham hip resurfacing at ten years: role of routine whole blood metal ion measurements in screening for pseudotumours. Int Orthop, 2014;38(11):2251-2257.[13] Khan M, Takahashi T, Kuiper JH, et al. Current in vivo wear of metal-on-metal bearings assessed by exercise-related rise in plasma cobalt level. J Orthop Res. 2006;24(11):2029-2035.[14] Matteo C, Giuseppe T, Andrea S, et al. Hip Resurfacing Implants. Orthopedics. 2015;38(8): 504-509.[15] 唐智,桂斌捷,丁楠,等.全髋关节置换后不同体位摄片髋臼角度的变化[J].中国组织工程研究,2016,20(26): 3817- 3822.[16] Mellon Stephen J, George G, Andersen Michael S, et al. Optimal acetabular component orientation estimated using edge-loading and impingement risk in patients with metal-on-metal hip resurfacing arthroplasty. J Biomech. 2015;48(2):318-323.[17] 邵建树,厉晓龙,刘伟峰,等.全髋关节置换中臼杯放置角度对关节屈伸活动安全性的影响[J].中国组织工程研究, 2015, 19(44):7053-7058.[18] Hart AJ, Skinner JA, Henckel J, et al. Insufficient acetabular version increases blood metal ion levels after metal-on-metal hip resurfacing. Clin Orthop Relat Res. 2011;469(9):2590-2597.[19] Langton DJ, Joyce TJ, Mangat N, et al. Reducing metal ion release following hip resurfacing arthroplasty. Orthop Clin North Am. 2011;42(2):169-180.[20] Langton DJ, Sprowson AP, Joyce TJ, et al. Blood metal ion concentrations after hip resurfacing arthroplasty: a comparative study of articular surface replacement and Birmingham Hip Resurfacing arthroplasties. J Bone Joint Surg Br. 2009;91(10):1287-1295.[21] Robinson PG, Wilkinson AJ, Meek RM. Metal ion levels and revision rates in metal-on-metal hip resurfacing arthroplasty: a comparative study. Hip Int. 2014;24(2): 123-128.[22] Holland JP, Langton DJ, Hashmi M. Ten-year clinical, radiological and metal ion analysis of the Birmingham Hip Resurfacing. J Bone Joint Surg Br. 2012;94(4): 471-476.[23] Harlan C,Amstutz MD,Karren M. The effect of patient selection and surgical technique on the results of Conserve® Plus hip resurfacing--3.5-to-14-year follow-up. Orthop Clin N Am. 2011;42(2):133-142. [24] De Steiger RN, Hang JR, Miller LN, et al. Five-year results of the ASR XL acetabular system and the ASR hip resurfacing system an analysis from the australian orthopaedic association national joint replacement registry. J Bone Joint Surg Am. 2011;93(24):2287- 2293.[25] Reito A, Puolakka T, Elo P, er al. High prevalence of adverse reactions to metal debris in small-headed ASR™ hips. Clin Orthop Relat Res. 2013;471(9):2954- 2961.[26] Jarvis IW, Meczes EL, Thomas HD, et al. Therapy-induced carboplatin-DNA adduct levels in human ovarian tumours in relation to assessment of adduct measurement in mouse tissues. Biochem Pharmacol. 2012,83(1):69-77.[27] Rezi? I, Curkovi? L, Ujevi? M. Simple methods for characterization of metals in historical textile threads. Talanta. 2010;82(1):237-244.[28] Matthies A, Underwood R, Cann P, et al. Retrieval analysis of 240 metal-on-metal hip components, comparing modular total hip replacement with hip resurfacing. J Bone Joint Surg Br. 2011;93(3):307-314.[29] Langton DJ, Jameson SS, Joyce TJ, et al. Early failure of metal-on-metal bearings in hip resurfacing and large-diameter total hip replacement: a consequence of excess wear. J Bone Joint Surg Br. 2010;92(1): 38-46.[30] Daniel J, Ziaee H, Pradhan C, et al. Six-year results of a prospective study of metal ion levels in young patients with metal-on-metal hip resurfacings. J Bone Joint Surg Br. 2009;91(2):176-179.[31] Bitsch RG, Zamorano M, Loidolt T, et al. Ion production and excretion in a patient with a metal-on-metal bearing hip prosthesis. A case report.J Bone Joint Surg Am. 2007;89(12):2758-2763.[32] Macpherson GJ, Breusch SJ. Metal-on-metal hip resurfacing: a critical review. Arch Orthop Trauma Surg. 2011;131(1):101-110.[33] Hosman AH, van der Mei HC, Bulstra SK, et al. Effects of metal-on-metal wear on the host immune system and infection in hip arthroplasty. Acta Orthop. 2010; 81(5): 526-534. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||