Chinese Journal of Tissue Engineering Research ›› 2017, Vol. 21 ›› Issue (11): 1658-1663.doi: 10.3969/j.issn.2095-4344.2017.11.004
Previous Articles Next Articles
Does a fixed distal femur resection angle influence radiographic alignment in total knee arthroplasty?
Ma Lu-yao1, Guo Wan-shou1, 2, Ma Jin-hui1, Yue De-bo2
- 1China-Japan Friendship School of Clinical Medicine, Peking University, Beijing 100029, China; 2Department of Joint Surgery, China-Japan Friendship Hospital, Beijing 100029, China
-
Revised:2017-01-09Online:2017-04-18Published:2017-05-06 -
Contact:Guo Wan-shou, Chief physician, Professor, Doctoral supervisor, China-Japan Friendship School of Clinical Medicine, Peking University, Beijing 100029, China; Department of Joint Surgery, China-Japan Friendship Hospital, Beijing 100029, China -
About author:Ma Lu-yao, Studying for doctorate, China-Japan Friendship School of Clinical Medicine, Peking University, Beijing 100029, China
CLC Number:
Cite this article
Ma Lu-yao, Guo Wan-shou, Ma Jin-hui, Yue De-bo. Does a fixed distal femur resection angle influence radiographic alignment in total knee arthroplasty? [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(11): 1658-1663.
share this article
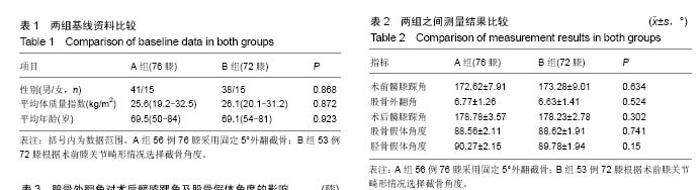
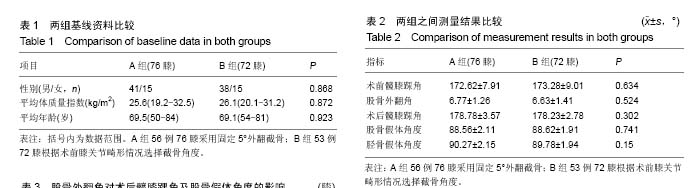
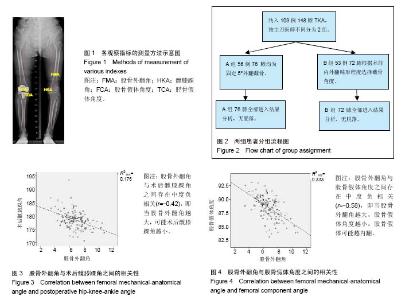
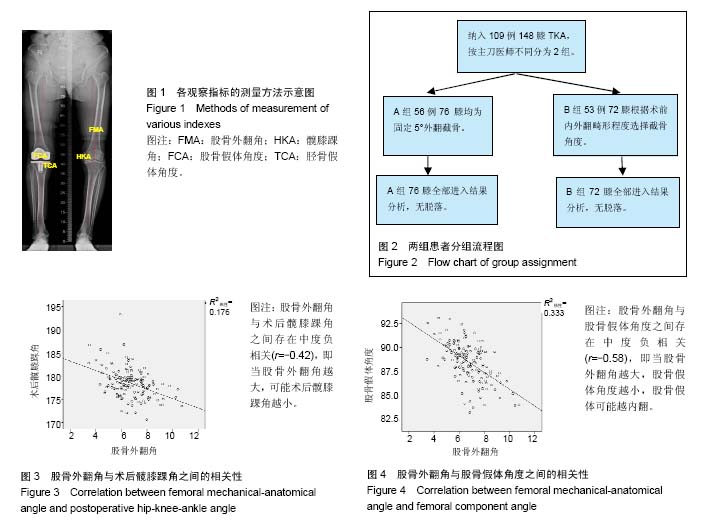
2.1 参与者数量分析 按意向性处理,共109例患者的148膝TKA纳入研究,根据不同的主刀医师将患者分为2组,A组56例76膝TKA选择固定5°外翻截骨,B组53例72膝TKA根据术前膝关节畸形情况选择截骨角度。全部进入结果分析,无脱落。分组流程图见图2。 2.2 基线资料比较 2组患者在性别、年龄及体质量指数方面之间差异均无显著性意义,具有可比性(表1)。 2.3 测量指标比较 2组在股骨外翻角、术前髋膝踝角、术后髋膝踝角、股骨及胫骨假体角度之间差异均无显著性意义(表2)。A组术后平均髋膝踝角为178.78°,内外翻3°以内为62%;B组术后平均髋膝踝角为178.23°,内外翻3°以内为65%,2组差异并无显著性意义(P=0.664)。"
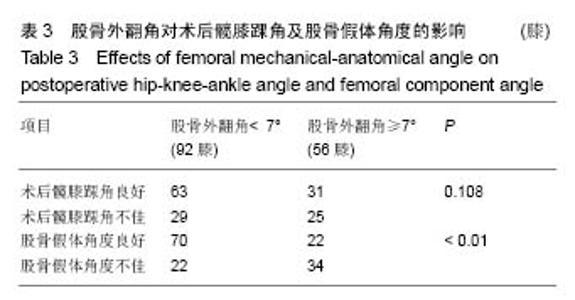
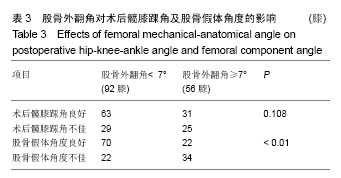
2.4 股骨外翻角的分组比较 所有患者术前股骨外翻角平均为(6.70±1.34)°(3.45°-10.74°),所有股骨外翻角中小于7°的共有92膝(62%),≥7°的共有56膝(38%)。股骨外翻角分别与术后髋膝踝角良好及不佳、股骨假体角度良好及不佳的结果进行卡方检验(表3)。在股骨外翻角<7°组,有69%的TKA术后力线良好,而在≥7°组中,有55%的TKA术后力线良好,2组之间差异无显著性意义(P=0.108)。在股骨外翻角<7°组中,术后有76%股骨假体对线良好,而≥7°组中仅有39%股骨假体对线良好,两组差异有显著性意义(P < 0.01)。将股骨外翻角与术后髋膝踝角进行Pearson相关性分析,r=-0.42,P < 0.01(图3)。股骨外翻角与股骨假体角度进行Pearson相关性分析,r=-0.58,P < 0.01(图4)。 2.5 不良事件 本研究中纳入的所有患者均无不良事件发生。"
"
| [1] Parratte S, Pagnano MW, Trousdale RT, et al. Effect of postoperative mechanical axis alignment on the fifteen-year survival of modern, cemented total knee replacements. J Bone Joint Surg Am. 2010;92(12): 2143-2149.[2] Vanlommel L, Vanlommel J, Claes S, et al. Slight undercorrection following total knee arthroplasty results in superior clinical outcomes in varus knees. Knee Surg Sports Traumatol Arthrosc. 2013; 21(10): 2325-2330.[3] Bellemans J. Neutral mechanical alignment: a requirement for successful TKA: opposes. Orthopedics.2011;34(9): e507-509.[4] Bellemans J, Colyn W, Vandenneucker H, et al. The Chitranjan Ranawat award: is neutral mechanical alignment normal for all patients? The concept of constitutional varus. Clin Orthop Relat Res. 2012;470(1): 45-53.[5] Fang DM, Ritter MA, Davis KE. Coronal alignment in total knee arthroplasty: just how important is it. J Arthroplasty. 2009;24(6 Suppl): 39-43.[6] Berend ME, Ritter MA, Meding JB, et al. Tibial component failure mechanisms in total knee arthroplasty. Clin Orthop Relat Res. 2004;(428): 26-34.[7] Werner FW, Ayers DC, Maletsky LP, et al. The effect of valgus/varus malalignment on load distribution in total knee replacements. J Biomech. 2005;38(2):349-355.[8] Ritter MA, Davis KE, Meding JB, et al. The effect of alignment and BMI on failure of total knee replacement. J Bone Joint Surg Am. 2011;93(17):1588-1596.[9] Longstaff LM, Sloan K, Stamp N, et al. Good alignment after total knee arthroplasty leads to faster rehabilitation and better function. J Arthroplasty. 2009;24(4): 570-578.[10] Mason JB, Fehring TK, Estok R, et al. Meta-analysis of alignment outcomes in computer-assisted total knee arthroplasty surgery. J Arthroplasty. 2007;22(8): 1097-1106.[11] Thienpont E, Fennema P, Price A. Can technology improve alignment during knee arthroplasty. Knee. 2013;20 Suppl 1: S21-28.[12] Confalonieri N, Manzotti A, Pullen C, et al. Computer-assisted technique versus intramedullary and extramedullary alignment systems in total knee replacement: a radiological comparison. Acta Orthop Belg. 2005;71(6): 703-709.[13] Shah NA, Patil HG, Dhawale AS, et al. Limited femoral navigation versus conventional intramedullary femoral jig based instrumentation for achieving optimal restoration of mechanical axis post total knee arthroplasty: a prospective comparative study of 200 knees. J Arthroplasty. 2015;30(4): 559-563.[14] Voleti PB, Hamula MJ, Baldwin KD, et al. Current data do not support routine use of patient-specific instrumentation in total knee arthroplasty. J Arthroplasty. 2014;29(9):1709-1712.[15] Nam D, Nawabi DH, Cross MB, et al. Accelerometer-based computer navigation for performing the distal femoral resection in total knee arthroplasty. J Arthroplasty. 2012;27(9): 1717-1722.[16] Hasegawa M, Miyazaki S, Yamaguchi T, et al. Comparison of Midterm Outcomes of Minimally Invasive Computer-Assisted vs Minimally Invasive Jig-Based Total Knee Arthroplasty. J Arthroplasty. 2017;32(1): 43-46.[17] Bae DK, Song SJ, Park CH, et al. A Comparison of the Medium-Term Results of Total Knee Arthroplasty Using Computer-Assisted and Conventional Techniques to Treat Patients With Extraarticular Femoral Deformities. J Arthroplasty. 2017;32(1): 71-78.[18] Miyasaka T, Kurosaka D, Saito M, et al. Accuracy of Computed Tomography-Based Navigation-Assisted Total Knee Arthroplasty: Outlier Analysis. J Arthroplasty. 2017;32(1): 47-52.[19] Fujimoto E, Sasashige Y, Nakata K, et al. Technical Considerations and Accuracy Improvement of Accelerometer-Based Portable Computer Navigation for Performing Distal Femoral Resection in Total Knee Arthroplasty. J Arthroplasty. 2017;32(1): 53-60.[20] Liodakis E, Antoniou J, Zukor DJ, et al. Navigated vs Conventional Total Knee Arthroplasty: Is There a Difference in the Rate of Respiratory Complications and Transfusions. J Arthroplasty. 2016;31(10): 2273-2277.[21] Zhu M, Ang CL, Yeo SJ, et al. Minimally Invasive Computer-Assisted Total Knee Arthroplasty Compared With Conventional Total Knee Arthroplasty: A Prospective 9-Year Follow-Up. J Arthroplasty. 2016;31(5):1000-1004.[22] Nam D, Vajapey S, Haynes JA, et al. Does Use of a Variable Distal Femur Resection Angle Improve Radiographic Alignment in Primary Total Knee Arthroplasty. J Arthroplasty. 2016.[23] Bardakos N, Cil A, Thompson B, et al. Mechanical axis cannot be restored in total knee arthroplasty with a fixed valgus resection angle: a radiographic study. J Arthroplasty. 2007;22(6 Suppl 2): 85-89.[24] Shi X, Li H, Zhou Z, et al. Comparison of Postoperative Alignment Using Fixed vs Individual Valgus Correction Angle in Primary Total Knee Arthroplasty With Lateral Bowing Femur. J Arthroplasty. 2016;31(5): 976-983.[25] Davis JA, Hogan C, Dayton M. Postoperative Coronal Alignment After Total Knee Arthroplasty: Does Tailoring the Femoral Valgus Cut Angle Really Matter. J Arthroplasty. 2015; 30(8):1444-1448.[26] McGrory JE, Trousdale RT, Pagnano MW, et al. Preoperative hip to ankle radiographs in total knee arthroplasty. Clin Orthop Relat Res. 2002;(404):196-202.[27] Kharwadkar N, Kent RE, Sharara KH, et al. 5 degrees to 6 degrees of distal femoral cut for uncomplicated primary total knee arthroplasty: is it safe. Knee. 2006;13(1): 57-60.[28] Deakin AH, Basanagoudar PL, Nunag P, et al. Natural distribution of the femoral mechanical-anatomical angle in an osteoarthritic population and its relevance to total knee arthroplasty. Knee. 2012;19(2): 120-123.[29] Nam D, Maher PA, Robles A, et al. Variability in the relationship between the distal femoral mechanical and anatomical axes in patients undergoing primary total knee arthroplasty. J Arthroplasty. 2013;28(5): 798-801.[30] Oswald MH, Jakob RP, Schneider E, et al. Radiological analysis of normal axial alignment of femur and tibia in view of total knee arthroplasty. J Arthroplasty. 1993;8(4): 419-426.[31] Moreland JR, Bassett LW, Hanker GJ. Radiographic analysis of the axial alignment of the lower extremity. J Bone Joint Surg Am. 1987;69(5): 745-749.[32] Huang TW, Lee CY, Lin SJ, et al. The Influence of Alignment on Midterm Outcome after Total Knee Arthroplasty in Patients With Marked Coronal Femoral Bowing. J Arthroplasty. 2015; 30(9):1531-1536.[33] Deakin AH, Sarungi M. A comparison of variable angle versus fixed angle distal femoral resection in primary total knee arthroplasty. J Arthroplasty. 2014;29(6): 1133-1137.[34] Meric G, Gracitelli GC, Aram LJ, et al. Variability in Distal Femoral Anatomy in Patients Undergoing Total Knee Arthroplasty: Measurements on 13,546 Computed Tomography Scans. J Arthroplasty. 2015;30(10): 1835-1838.[35] Yau WP, Chiu KY, Tang WM, et al. Coronal bowing of the femur and tibia in Chinese: its incidence and effects on total knee arthroplasty planning. J Orthop Surg (Hong Kong). 2007;15(1): 32-36.[36] SC Reed JG. The accuracy of femoral intramedullary guides in total knee arthroplasty. J Arthroplasty. 1997.[37] Xiao J, Wang C, Zhu L, et al. Improved method for planning intramedullary guiding rod entry point in total knee arthroplasty. Arch Orthop Trauma Surg. 2014;134(5): 693-698.[38] Swanson KE, Stocks GW, Warren PD, et al. Does axial limb rotation affect the alignment measurements in deformed limbs. Clin Orthop Relat Res. 2000;(371): 246-252. |
| [1] | Jiang Zi-wei, Huang Feng, Cheng Si-yuan, Zheng Xiao-hui, Sun Shi-dong, Zhao Jing-tao, Cong Hai-chen,Sun Han-qiao, Dong Hang. Design and finite element analysis of digital splint [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1052-1056. |
| [2] | Wang Fei, Liu Zhi-bin, Tao Hui-ren, Zhang Jian-hua, Li Chang-hong, Cao Qiang, Zheng Jun, Liu Yan-xiong, Qu Xiao-peng. Clinical efficacy of preoperative osteotomy designs using paper-cut technology versus photoshop software for ankylosing spondylitis with kyphosis [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1057-1063. |
| [3] | Li Hui, Ma Jun-yi, Ma Yuan, Zhu Xu . Establishment of a three-dimensional finite element model of ankylosing spondylitis kyphosis [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1069-1073. |
| [4] | Ling Guan-han, Ou Zhi-xue, Yao Lan, Wen Li-chun, Wang Guo-xiang, Lin Heng-feng. Establishment of simulating three-dimensional model of China-Japan Friendship Hospital Classification for L type osteonecrosis of the femoral head [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1074-1079. |
| [5] | Fu Wei-min, Wang Ben-jie. Assessing the degree of necrotic femoral head, and association of blood supply with pathlogical changes: study protocol for a diagnostic animal trial [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1086-1091. |
| [6] | Zhang Wen-qiang, Ding Qian, Zhang Na. Associations between alpha angle and herniation pit on oblique axial magnetic resonance imaging in asymptomatic hip joints of adults [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1098-1103. |
| [7] | Sun Xiao-xin1, Zhou Wei2, Zuo Shu-ping3, Liu Hao1, Song Jing-feng1, Liang Chun-yu1. Morphological characteristics for the magnetic resonance imaging assessment of discoid lateral meniscal tears in children [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1104-1109. |
| [8] | Lin Han-wen, Wen Jun-mao, Huang Chao-yuan, Zhou Chi, Tang Hong-yu. Correlation between the changes in lower limb power line and pain area in the knee osteoarthritis patients: imaging evaluation [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1110-1114. |
| [9] | Zhang Yun-ge, Song Ke-guan. Periprosthetic osteolysis induced by wear particles: research progress of calcineurin/activated T cell nuclear factor signaling pathway [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1115-1122. |
| [10] | Liu Wei, Huang Jian. Applied research and progress of three-dimensional printing technology in joint replacement [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1123-1130. |
| [11] | Liu Jian-kun, Deng Shu-cai. Status and role of three-dimensional printing technology in spine surgery [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1131-1136. |
| [12] | Xi Li-cheng, Li Hong-yu. Research progress of the influence of alcohol on the local microenvironment of femoral head [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1137-1142. |
| [13] | Ye Xiang-yang, Sun Xiang, Tang Li-xin, Zhen Ping, Geng Bin, Wang Hua-lei, Zhao Yu-guo. Acetabular liner wear of cross-linked versus conventional polyethylene for total hip arthroplasty: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1143-1148. |
| [14] | Liang Xin, Wang Heng, Li Xian-rong. Preoperative application of alprazolam for patients with anxiety and depression and pain after total knee arthroplasty: its safety and effectiveness [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 985-992. |
| [15] | Shi Bin, An Jing, Chen Long-gang, Zhang Nan, Tian Ye . Influencing factors for pain after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 993-997. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||