Chinese Journal of Tissue Engineering Research ›› 2016, Vol. 20 ›› Issue (44): 6682-6688.doi: 10.3969/j.issn.2095-4344.2016.44.021
Auxiliary reference significance of Blumensaat line for knee joint disease
Cheng Xiang-yun, Zhang Sheng-xiao, Cao Wan-quan, Wang Gang, Lu Yan-hui, Zhu Hong, Yang Zi-quan
- Department of Orthopedic Surgery, the Second Hospital of Shanxi Medical University, Taiyuan 030001, Shanxi Province, China
-
Revised:2016-08-10Online:2016-10-28Published:2016-10-28 -
Contact:Yang Zi-quan, M.D., Associate chief physician, Associate professor, Master’s supervisor, Department of Orthopedic Surgery, the Second Hospital of Shanxi Medical University, Taiyuan 030001, Shanxi Province, China -
About author:Cheng Xiang-yun, Studying for master’s degree, Department of Orthopedic Surgery, the Second Hospital of Shanxi Medical University, Taiyuan 030001, Shanxi Province, China -
Supported by:the Natural Science Foundation of Shanxi Province, No. 2015011111; the National Natural Science Foundation of China, No. 30973048
CLC Number:
Cite this article
Cheng Xiang-yun, Zhang Sheng-xiao, Cao Wan-quan, Wang Gang, Lu Yan-hui, Zhu Hong, Yang Zi-quan. Auxiliary reference significance of Blumensaat line for knee joint disease[J]. Chinese Journal of Tissue Engineering Research, 2016, 20(44): 6682-6688.
share this article
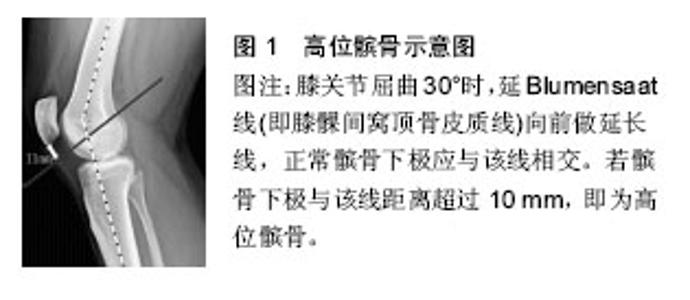
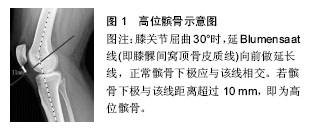
2.1 Blumensaat线与高位髌骨的判断 2.1.1 高位髌骨介绍 高位髌骨是指髌骨与股骨滑车比较,髌骨位置相对较高,在膝关节屈曲时,引起髌骨不稳定的一类骨关节疾病[7]。绝大多数的高位髌骨患者的发病原因是先天性髌骨发育异常,其中女性患者居多,男女比例为1∶1.5[8]。由于高位髌骨位置的特殊性,髌骨在屈曲位时,常压迫髌上囊,髌股关节间压力增加,关节应力亦随之发生改变[9]。高位髌骨患者随着年龄增长,其继发性疾病随之增多,如继发性习惯性髌骨脱位、Osgood-Schlatter骨突炎、髌骨软骨软化症、髌股关节炎等,因而如何对高位髌骨进行早期诊断显得尤为重要[10]。 2.1.2 Blumensaat线法测高位髌骨 高位髌骨主要依靠影像学资料同时结合患者自身症状来进行早期诊断。此处着重介绍Blumensaat法[11]。1938年学者Blumensaat等首先报道了此方法:在膝关节屈曲30°时,延Blumensaat线(即膝髁间窝顶骨皮质线)向前做延长线,正常髌骨下极应与该线相交。若髌骨下极与该线距离超过10 mm,即为高位髌骨[12](如图1所示)。该方法有两个主要缺点[13]:第一,在摄片时,患者一般不能准确屈曲到30°;第二,Blumensaat线与股骨长轴所形成的夹角(intercondylar shelf angle,ISA)在不同患者身上有差异,这就影响了该方法所测距离的准确性,见图2。"
"
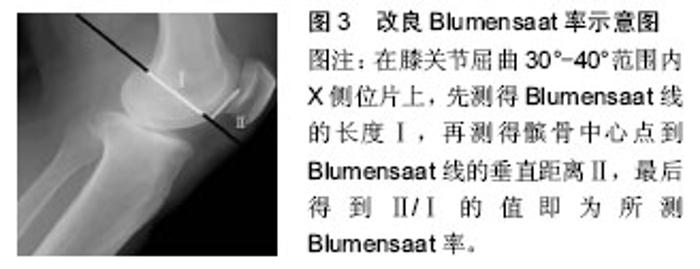
随着医学不断发展,为了消除这两个缺点,改良Blumensaat法(ISA-corrected Blumensaat methods)被学者提出[14]。该方法与原始Blumensaat法的区别在于:在测量髌骨下极与Blumensaat线的垂直距离时,明确规定好Blumensaat线与股骨长轴的角度,该角度由专业统计人员所统计出,可小范围波动。 而后,因为以上两种方法在操作中欠简便,日本学者更新了另一种改良Blumensaat率[15](modified Blumensaat ratio):在膝关节屈曲30°-40°范围内X射线侧位片上,先测得Blumensaat线的长度Ⅰ,再测得髌骨中心点到Blumensaat线的垂直距离Ⅱ,最后得到Ⅱ/Ⅰ的值即为所测Blumensaat率。Blumensaat率的正常值为0.8-1.2。大于1.2即为高位髌骨(见图3)。"
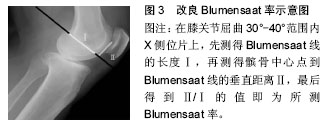
目前在测量髌骨高度领域依靠X射线片被广泛认可和使用的经典指标主要还有以下几种:Insall-Salvat(IS)指数,Blackburne-Peel(BP)指数和Caton-Deschamps(CD)指数等。其中Blumensaat法、改良Blumensaat法这种直接方法已逐渐被经典的Insall-Salvat(IS)指数,Blackburne-Peel(BP)指数和Caton-Deschamps(CD)指数等取代。髌骨滑车指数是完全基于MRI技术的测量髌骨高度的方法,其于2006年由Biedert等提出,已获得一定认可度和使用度。 通过影像学方法结合患者自身情况诊断高位髌骨后,对该疾病主要有以下治疗方法。早期症状较轻时可采用保守治疗,主要包括药物治疗(如注射玻璃酸钠、口服营养药物等)和行为治疗(避免过度运动等)。症状严重甚至出现髌骨脱位的患者则可以考虑手术治疗,目前主要术式包括髌韧带转位术、胫骨结节移位术、内侧髌股韧带重建,外侧支持带松解、滑车成形等,并辅助以关节镜下髌骨关节软骨表面化处理。对于重度髌股关节病的患者,可以考虑行膝关节置换[16]。 就目前为止,高位髌骨仍缺乏经典、精准的测量方法以及比较全面的治疗标准。从最初的Blumensaat值到如今日本学者提出的改良Blumensaat率,高位髌骨的测量方法一直在更新、简化中。相信不久的将来,在同道的共同努力下,一个更能实际应用于临床,同时操作简便的髌骨测量方法会出现。在如今高速发展的医疗背景下,对于高位髌骨的治疗方法,相信很快会有根据患者严重程度、年龄、性别、种族人群而制定的治疗细则出现。 2.2 Blumensaat线与前交叉韧带损伤的判断 2.2.1 前交叉韧带损伤介绍 膝关节前交叉韧带,为膝关节内的核心结构,起于股骨外侧髁内侧面,止于胫骨髁间隆起前方,并与外侧半月板的前中部相连[17]。它是维持膝关节稳定性的重要韧带,可防止胫骨向前移位等[18]。前交叉韧带损伤后可导致膝关节疼痛、活动障碍,如果诊治不当或延误治疗会导致膝关节的不稳定,并继发退行性关节炎等疾病,为此前交叉韧带损伤后及时准确的诊治是十分必要的[19]。 2.2.2 Blumensaat角辅助诊断前交叉韧带损伤 前交叉韧带损伤后的诊断主要依靠一系列辅助检查[20]。Lachman试验和前抽屉试验这两种临床检查方法在诊断前交叉韧带损伤中比较常用。通过X射线及CT检查不能直接观察出前交叉韧带的损伤,但可判断前交叉韧带起止点是否有撕脱性细微骨折块以及其骨折块的的数量、大小。而MRI具有高分辨率、高软组织对比、无痛、无放射和多切面成像的特点,MRI是前交叉韧带损伤的最主要影像学检查[21]。 膝关节MRI诊断前交叉韧带损伤可依据MRI影像的直接征象(如前交叉韧带消失,韧带连续性中断等)和间接征象(如Blumensaat角异常等)[22]。文章主要介绍的是MRI影像上依据Blumensaat角辅助诊断前交叉韧带损伤[23]。 Blumensaat角,即Blumensaat线和前交叉韧带远端部分延长交叉所形成的夹角,该角度在MRI图像的髁间窝部分矢状层面上比较容易观察(如图4所示)。正常人MRI上观察Blumensaat一般在0°-15°之间,若该角度大于15°,或者该角度呈负值(即两线相交于远端),皆提示前交叉韧带损伤[24]。对此角度的认识可进一步增加相关工作者对MRI影像上前交叉韧带损伤的把握能力,进一步提高其准确率。"
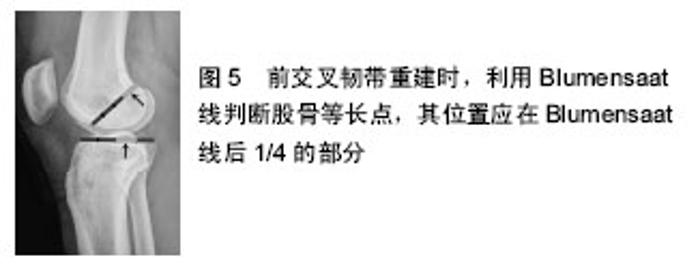
Blumensaat角作为一个间接征象判断前交叉韧带损伤,有其独特的优势,但是也有局限的一面。Blumensaat角之所以能辅助判断前交叉韧带损伤,其原理如下:因为前交叉韧带起于股骨外侧髁内侧面,故在MRI图像上矢状面髁间窝部分,可看到Blumensaat线与前交叉韧带形成一个夹角。若前交叉韧带未损伤,可看到前交叉韧带和Blumensaat线的夹角很小(0°-15°),其夹角相交于近端。当前交叉韧带发生损伤时,前交叉韧带会出现松弛迂曲或者直接发生断裂,此时前交叉韧带和Blumensaat线的夹角则会变大,甚至因为前交叉韧带断裂,其夹角相交于远端[25]。从此原理可以看出,Blumensaat角可以较好反映前交叉韧带损伤情况。对于一些陈旧性损伤的患者,前交叉韧带被吸收,Blumensaat角便不能发挥其辅助作用,但是此类患者单凭直接征象便可较好判断。利用Blumensaat角的另一局限性为,该角度的测量并没有统一完善的标准,对于前交叉韧带轻微撕裂的患者,由于前交叉韧带迂曲不明显,利用Blumensaat角进行测量,还是存在一定误差,此时应结合另外一些征象进行判断。 前交叉韧带损伤的MRI征象: 直接征象[26]:①前交叉韧带消失;②韧带连续性中断,实质断裂;③韧带扭曲,呈波浪状改变;④韧带内形成假瘤;⑤韧带出现部分或弥漫高信号;⑥起止点的撕脱骨折;⑦前交叉韧带走行异常。 间接征象[27]:① Blumensaat角改变;②后交叉韧带弓形变;③后交叉韧带夹角< 105°;④半月板外周部垂直撕裂;⑤同时具有股骨外侧髁骨挫伤和胫骨平台前外侧骨挫伤的表现;⑥股骨外侧髁凹陷征(Notch征);⑦Segond骨折;⑧胫骨前移位等。 2.3 Blumensaat线与前交叉韧带损伤重建的位置定位 2.3.1 关于前交叉韧带损伤重建 前交叉韧带损伤后,患者步行时膝关节很大概率会出现漂浮不稳、无力,有脱出的感觉,严重影响患者的生活质量,并且会继发骨性关节炎。若前交叉韧带断裂1/4以上或完全断裂,目前主流的治疗措施是行膝前交叉韧带重建手术[28]。目前前交叉韧带重建手术依靠膝关节镜进行引导,就重建材料来分类主要包括自体肌腱重建和人工韧带重建。依据前交叉韧带重建方法,大致可分为单束重建和双束重建[29]。 前交叉韧带重建手术步骤主要如下:对膝关节腔在关节镜下进行顺序检查,判断前交叉韧带损伤程度;取自体肌腱或人工肌腱;前交叉韧带等长点的确定;胫骨骨隧道的选择;钻取骨隧道;前交叉韧带移植物的引入与固定[30]。 其中,一个关键步骤为等长点的确定,该步骤甚至可以决定该手术的成功与否[31]。因为移植物若位置不佳,很大概率会与股骨髁间窝发生撞击,或者与股骨外髁内侧面发生磨损,对患者术后恢复会造成不良影响。手术后的前交叉韧带需与原始前交叉韧带最大程度的保持等长,这样在运动中重建材料才能始终保持紧张,患膝不至于出现某个范围内的失稳。现在,如何进行有效定位也是现在的研究热点,利用Blumensaat线辅助定位前交叉韧带等长点已被越来越多的人认可[32]。 2.3.2 Blumensaat线和前交叉韧带损伤重建 利用Blumensaat线确定前交叉韧带重建等长点最为经典的方法便是Harner四分法,其在X射线片上即可判断等长点的正确位置:将Blumensaat线四等分,便可确定股骨隧道等长点位置,其位置应在Blumensaat线后1/4的部分,而胫骨隧道等长点应在在胫骨平台关节面长度的第2个1/4处(如图5所示)。在手术中按照术前的Harner四分法测量同时参考膝内侧髁间隆起进行准确定位,手术后可根据X线片来进行评估分析。文献显示使用该定位方法,患者术后恢复良好,Lysholm膝关节功能评分术前(45.5±6.5)分,术后(96.2±2.2)分[33]。 除等长点的确定,骨隧道钻取也非常重要,应保证胫骨隧道外口、胫骨隧道等长点、股骨隧道外口、股骨隧道等长点这4点应保持一条直线[34]。以上便是利用Blumensaat线定位前交叉韧带等长点的内容。其效果比较好的原因在于,骨道位置很接近原始前交叉韧带起止点的位置。现有研究表明,对于解剖重建可很有效的增加手术效果[35]。"
| [1] Seyahi A, Atalar AC, Koyuncu LO, et al. [Blumensaat line and patellar height]. Acta Orthop Traumatol Turc. 2006;40(3):240-247. [2] Barnett AJ, Prentice M, Mandalia V, et al. Patellar height measurement in trochlear dysplasia. Knee Surg Sports Traumatol Arthrosc. 2009; 17: 1412-1415. [3] Hanada M, Takahashi M, Koyama H, et al. Assessing the validity of the modified Blumensaat method for radiographic evaluation of patellar height. Eur J Orthop Surg Traumatol. 2015; 25: 757-762. [4] Holtzman GW, Harris-Hayes M. Treatment of patella alta with taping, exercise, mobilization, and functional activity modification: a case report. Physiother Theory Pract. 2012; 28: 71-83. [5] 张克民,李伟,于立志.膝关节前交叉韧带损伤的MRI诊断及分析[J].中国矫形外科杂志,2011,19(8): 637-39. [6] 徐雁,敖英芳,余家阔,等.单束重建前交叉韧带骨道位置对临床效果影响的研究[J]. 中国运动医学杂志,2008,27(2): 202-205. [7] Ali SA, Helmer R, Terk MR. Patella alta: lack of correlation between patellotrochlear cartilage congruence and commonly used patellar height ratios. AJR.2009;193:1361-1366. [8] Brouwer RW, Bierma-Zeinstra SM, van Koeveringe AJ, et al. Patellar height and the inclination of the tibial plateau after high tibial osteotomy. The open versus the closed-wedge technique. J Bone Joint Surg Br. 2005; 87: 1227-1232. [9] Seidl A, Baldini T, Krughoff K, et al. Biomechanical Assessment of Patellar Advancement Procedures for Patella Alta. Orthopedics. 2016; 39: e492-497. [10] Magnussen RA, De Simone V, Lustig S, et al. Treatment of patella alta in patients with episodic patellar dislocation: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2014; 22: 2545-2550. [11] Otsuki S, Nakajima M, Oda S, et al. Three-dimensional transfer of the tibial tuberosity for patellar instability with patella alta. J Orthop Sci. 2013; 18: 437-442. [12] Stefanik JJ, Zhu Y, Zumwalt AC, et al. Association between patella alta and the prevalence and worsening of structural features of patellofemoral joint osteoarthritis: the multicenter osteoarthritis study. Arthritis Care Res. 2010; 62: 1258-1265. [13] Benoit B, Laflamme GY, Laflamme GH, et al. Long-term outcome of surgically-treated habitual patellar dislocation in children with coexistent patella alta. Minimum follow-up of 11 years. J Bone Joint Surg Br. 2007; 89: 1172-1177. [14] Biedert RM, Albrecht S. The patellotrochlear index: a new index for assessing patellar height. Knee Surg Sports Traumatol Arthrosc.2006; 14: 707-712. [15] Narkbunnam R, Chareancholvanich K. Effect of patient position on measurement of patellar height ratio. Arch Orthop Trauma Surg. 2015; 135: 1151-1156. [16] Pace A, Fergusson C. Preoperative computerized radiograph measurement of Blumensaat's line as an aid to correct placement of the femoral tunnel in ACL reconstruction. J Knee Surg. 2006; 19: 176-180. [17] Ferretti M, Ekdahl M, Shen W, et al. Osseous landmarks of the femoral attachment of the anterior cruciate ligament: an anatomic study. Arthroscopy. 2007; 23: 1218-1225. [18] Roberts CC, Towers JD, Spangehl MJ, et al. Advanced MR imaging of the cruciate ligaments. Radiol Clin North Am. 2007; 45: 1003-1016, vi-vii. [19] 汪田福,郝智秀,高相飞.前交叉韧带生物力学特性及其损伤对膝关节稳定性的影响[J].清华大学学报(自然科学版), 010,96(7):1005-1008. [20] Farrow LD, Gillespie RJ, Victoroff BN, et al. Radiographic location of the lateral intercondylar ridge: its relationship to Blumensaat's line. Am J Sports Med. 2008; 36: 2002-2006. [21] Chan YS, Lo YP, Lien LC, et al. Improved divergence angles with femoral interference screw placement through the tibial tunnel as measured by multiplanar reconstruction computed tomography. Arthroscopy. 2009; 25: 54-61. [22] Magarelli N, Carducci C, Cannataro G, et al. MR in the evaluation of new anterior cruciate ligament and tibial tunnel position: correlation with clinical and functional features. Radiol Med. 2011; 116: 1124-1133. [23] 潘诗农,卢再鸣,陈志安,等.前交叉韧带损伤:3.0T MR影像与关节镜对照分析[J].中国介入影像与治疗学,2009,6(1): 5-9. [24] Saxena A, Ray B, Rajagopal KV, et al. Morphometry and magnetic resonance imaging of anterior cruciate ligament and measurement of secondary signs of anterior cruciate ligament tear. Bratisl Lek Listy. 2012; 113(9):539-543. [25] Chen L, Zhao H, Li J, et al. [Diffusion tensor imaging map of anterior cruciate ligament contrasted with MRI in healthy adults]. Zhong nan da xue xue bao Yi xue ban. 2013; 38: 610-616. [26] 张洪志,刘爱国,冯宝华,等.前交叉韧带损伤的诊断与治疗[J].中国矫形外科杂志,2013,21(2):146-149. [27] 廖云,孙仁权,廖国栋. MRI多征象分析在膝关节前交叉韧带损伤诊断中的临床应用价值分析[J]. 中国CT和MRI杂志, 2015,13(6): 101-103. [28] Kruczynski J, Piontek T, Trzeciak T, et al. [Graft remodeling following Hertel ACL reconstruction in MR imaging]. Chir Narzadow Ruchu Ortop Pol. 2003;68(2): 101-104. [29] Sinha S, Naik AK, Meena D, et al. Creation of femoral tunnel by outside-in technique for ACL reconstruction: an analysis. Arch Orthop Trauma Surg. 2014; 134: 1709-1716. [30] 岳勇,阿德力,哈巴西,等.膝关节前交叉韧带损伤的早期手术和晚期手术的系统评价[J]. 中国矫形外科杂志,2008, 16(12): 900-903. [31] Kadija M, Milovanovic D, Bumbasirevic M, et al. Length of the femoral tunnel in anatomic ACL reconstruction: comparison of three techniques. Knee Surg Sports Traumatol Arthroscopy. 2015. [32] Sinha S, Naik AK, Arya CS, et al. Trans-tibial guide wire placement for femoral tunnel in single bundle anterior cruciate ligament reconstruction. Indian J Orthop. 2015; 49: 352-356. [33] Rodriguez-Merchan EC. Evidence-Based ACL Reconstruction. Arch Bone Joint Surg. 2015; 3: 9-12. [34] Farrow LD, Morris PM, Huston KL, et al. A Simple Radiographic Sign of Vertical Anterior Cruciate Ligament Tunnel Placement. J Knee Surg. 2015; 28: 428-431. [35] Negahi Shirazi A, Chrzanowski W, Khademhosseini A, et al. Anterior Cruciate Ligament: Structure, Injuries and Regenerative Treatments. Adv Exp Med Biol. 2015; 881:161-186. [36] Speziali A, Placella G, Tei MM, et al. Diagnostic value of the clinical investigation in acute meniscal tears combined with anterior cruciate ligament injury using arthroscopic findings as golden standard. Musculoskeletal Surg. 2016; 100: 31-35. [37] Johnson AJ, Howell SM, Costa CR, et al. The ACL in the arthritic knee: how often is it present and can preoperative tests predict its presence? Clin Orthop Relat Res. 2013; 471: 181-188. [38] Frobell RB, Roos EM, Roos HP, et al. A randomized trial of treatment for acute anterior cruciate ligament tears. New Eng J Med. 2010; 363: 331-342. [39] Ageberg E. Neuromuscular training optimises knee function after arthroscopic ACL reconstruction. Aust J Physiother. 2007; 53: 287. |
| [1] | Shi Bin, An Jing, Chen Long-gang, Zhang Nan, Tian Ye . Influencing factors for pain after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 993-997. |
| [2] | Wang Xian-xun. Impact of local compression cryotherapy combined with continuous passive motion on the early functional recovery after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 998-1003. |
| [3] | Yuan Wei, Zhao Hui, Ding Zhe-ru, Wu Yu-li, Wu Hai-shan, Qian Qi-rong. Association between psychological resilience and acute mental disorders after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1015-1019. |
| [4] | Chen Qun-qun, Qiao Rong-qin, Duan Rui-qi, Hu Nian-hong, Li Zhao, Shao Min. Acu-Loc®2 volar distal radius bone plate system for repairing type C fracture of distal radius [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1025-1030. |
| [5] | Huang Xiang-wang, Liu Hong-zhe. A new low elastic modulus of beta titanium alloy Ti2448 spinal pedicle screw fixation affects thoracic stability: biomechanical analysis [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1031-1035. |
| [6] | Xie Qiang. Three-dimensional finite element model for biomechanical analysis of stress in knee inversion and external rotation after posterior cruciate ligament rupture [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1036-1040. |
| [7] | He Ze-dong, Zhao Jing, Chen Liang-yu, Li Ke, Weng Jie. Multilevel finite element analysis on the biological tribology damage of water on bone tissue [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1041-1045. |
| [8] | Jiang Zi-wei, Huang Feng, Cheng Si-yuan, Zheng Xiao-hui, Sun Shi-dong, Zhao Jing-tao, Cong Hai-chen,Sun Han-qiao, Dong Hang. Design and finite element analysis of digital splint [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1052-1056. |
| [9] | Wang Fei, Liu Zhi-bin, Tao Hui-ren, Zhang Jian-hua, Li Chang-hong, Cao Qiang, Zheng Jun, Liu Yan-xiong, Qu Xiao-peng. Clinical efficacy of preoperative osteotomy designs using paper-cut technology versus photoshop software for ankylosing spondylitis with kyphosis [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1057-1063. |
| [10] | Li Hui, Ma Jun-yi, Ma Yuan, Zhu Xu . Establishment of a three-dimensional finite element model of ankylosing spondylitis kyphosis [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1069-1073. |
| [11] | Ling Guan-han, Ou Zhi-xue, Yao Lan, Wen Li-chun, Wang Guo-xiang, Lin Heng-feng. Establishment of simulating three-dimensional model of China-Japan Friendship Hospital Classification for L type osteonecrosis of the femoral head [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1074-1079. |
| [12] | Fu Wei-min, Wang Ben-jie. Assessing the degree of necrotic femoral head, and association of blood supply with pathlogical changes: study protocol for a diagnostic animal trial [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1086-1091. |
| [13] | Zhang Wen-qiang, Ding Qian, Zhang Na. Associations between alpha angle and herniation pit on oblique axial magnetic resonance imaging in asymptomatic hip joints of adults [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1098-1103. |
| [14] | Sun Xiao-xin1, Zhou Wei2, Zuo Shu-ping3, Liu Hao1, Song Jing-feng1, Liang Chun-yu1. Morphological characteristics for the magnetic resonance imaging assessment of discoid lateral meniscal tears in children [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1104-1109. |
| [15] | Lin Han-wen, Wen Jun-mao, Huang Chao-yuan, Zhou Chi, Tang Hong-yu. Correlation between the changes in lower limb power line and pain area in the knee osteoarthritis patients: imaging evaluation [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1110-1114. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||