Chinese Journal of Tissue Engineering Research ›› 2026, Vol. 30 ›› Issue (22): 5659-5670.doi: 10.12307/2026.132
Previous Articles Next Articles
Articular cartilage lesions at different stages of steroid-induced osteonecrosis of the femoral head: characteristics and mechanisms of crescent sign formation
Wan Ziyi1, 2, Jiang Mengyu2, Zhou Yuehui1, 2, Xue Yuxuan1, 2, Wei Yangwenxiang1, 2, Zhou Chi3, 4, 5
- 1Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China; 2Lingnan Medical Research Center, Guangzhou University of Chinese Medicine, Guangzhou 510000, Guangdong Province, China; 3The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China; 4Guangdong Clinical Research Institute of Traditional Chinese Medicine, Guangzhou 510407, Guangdong Province, China; 5Maoming Hospital, Guangzhou University of Chinese Medicine, Maoming 525022, Guangdong Province, China
-
Received:2025-03-11Accepted:2025-08-08Online:2026-08-08Published:2025-12-26 -
Contact:Zhou Chi, PhD, Associate chief physician, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China; Guangdong Clinical Research Institute of Traditional Chinese Medicine, Guangzhou 510407, Guangdong Province, China; Maoming Hospital, Guangzhou University of Chinese Medicine, Maoming 525022, Guangdong Province, China -
About author:Wan Ziyi, MS candidate, Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China; Lingnan Medical Research Center, Guangzhou University of Chinese Medicine, Guangzhou 510000, Guangdong Province, China -
Supported by:National Natural Science Foundation of China, No. 82474539 (to ZC); 2023 Maoming Traditional Chinese Medicine Innovation and Development Program Project, No. 2024-2026(2023SZY008) (to ZC); Guangdong Provincial Medical Science and Technology Research Fund Project, No. A2024056 (to ZC)
CLC Number:
Cite this article
Wan Ziyi, Jiang Mengyu, Zhou Yuehui, Xue Yuxuan, Wei Yangwenxiang, Zhou Chi. Articular cartilage lesions at different stages of steroid-induced osteonecrosis of the femoral head: characteristics and mechanisms of crescent sign formation[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(22): 5659-5670.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
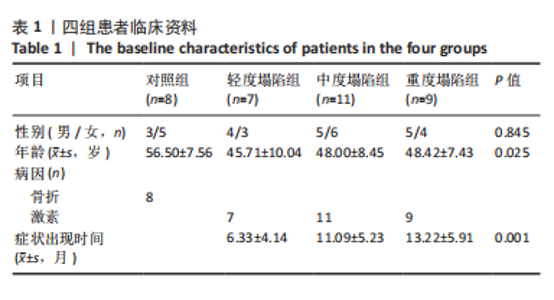
2.1 标本和临床资料收集分类 共收集35个股骨头标本,其中股骨颈骨折8例,激素性股骨头坏死27例,根据2019年国际骨循环研究会(ARCO)X射线片分期标准[24]、围塌陷期理论[25-26]、大体标本关节软骨形变程度,分为轻度塌陷(< 2 mm)组6例、中度塌陷(2-4 mm)组11例、重度塌陷(> 4 mm)组9例,股骨颈骨折标本作为对照组。临床资料如表1所示,各组间性别无明显差异,轻度塌陷组年龄显著小于对照组、中度塌陷组和重度塌陷组(P < 0.025)。"

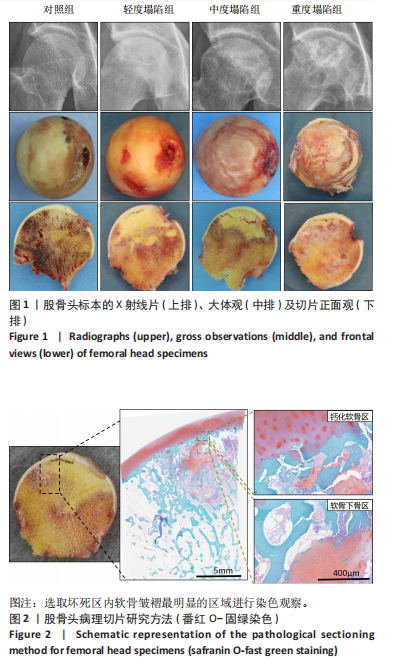
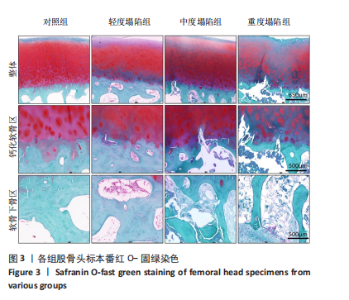
2.2 大体观察结果 患者分组如图1所示。对照组关节软骨厚度均匀,软骨表面光滑、完整,与软骨下骨无分离缺损,骨小梁排列规律,按压软骨质韧,各方向触感没有明显变化。轻度塌陷组关节厚度基本均匀,关节表面可见细微的褶皱,关节软骨与软骨下骨出现分离缺损,可见明显的坏死区,骨小梁排列紊乱,皱褶区域内按压可感受到柔软的触感和不平整。中度塌陷组关节厚度欠均匀,关节表面可见明显的皱褶,关节软骨与软骨下骨分离缺损面积较大,坏死区骨小梁排列紊乱,皱褶区域内按压可感受到软骨的不平整和脆弱松弛感。重度塌陷组关节表面软骨严重破坏,厚度不均,关节软骨与软骨下骨大面积分离缺损甚至剥脱,坏死区域骨小梁排列紊乱,皱褶区域按压有空虚感。 2.3 组织病理研究结果 股骨头组织病理研究方法如图2所示,切取软骨皱褶最明显的区域制成石蜡切片并染色,主要观察钙化软骨区和下方的软骨下骨区。 2.3.1 番红O-固绿染色结果 见图3。对照组软骨细胞排列有序,各层软骨结构清晰,可观察到同源软骨细胞均匀分布,软骨空陷窝较少,软骨基质染色均匀,软骨下骨板连续完整。轻度塌陷组软骨细胞排列较规律,各层软骨结构较清晰,可观察到同源软骨细胞减少,空陷窝增多,深层软骨基质染色"
"
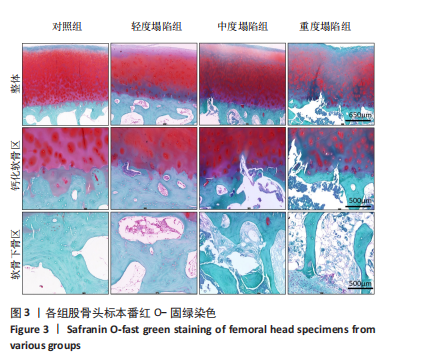
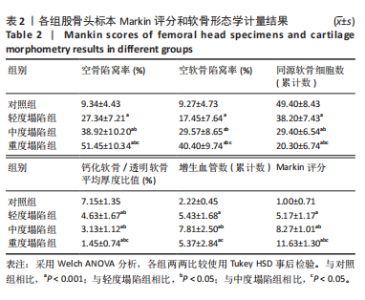
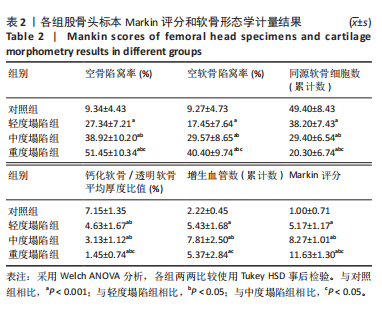
出现缺失,可见软骨下骨板断裂,骨侵蚀和片状软骨钙化。中度塌陷组软骨表面存在纤维化,软骨细胞排列不规律,各层软骨结构紊乱,同源软骨细胞分布较少,软骨空陷窝较多,深层软骨基质染色缺失,浅层软骨基质出现缺失,软骨下骨板断裂,深层软骨侵蚀,软骨下骨硬化增多。重度塌陷组可见软骨表面剥离或台阶样改变,软骨排列不规律,同源软骨较少,软骨空陷窝较多,深层软骨破坏,深层到浅层软骨基质染色大面积缺失,软骨下骨板断裂,关节软骨与软骨下骨分离,软骨下骨硬化明显。随着塌陷程度的增加,软骨细胞排列从有序逐渐变得紊乱,空陷窝数量增多,软骨基质从深层向浅层方向染色缺失,软骨下骨板的断裂和硬化现象增多。 对照组Markin评分为1.00±0.71,轻度塌陷组Markin评分为5.17±1.17,中度塌陷组Markin评分为8.27±1.01,重度塌陷组Markin评分为11.63± 1.30,塌陷程度越严重,关节软骨损伤越严重,激素性股骨头坏死各组与对照组比较差异均有显著性意义(P < 0.001),激素性股骨头坏死各组间两两比较差异均有显著性意义(P < 0.05),见表2。"
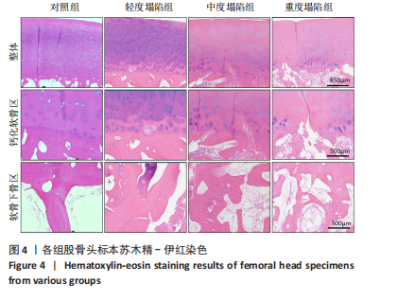
2.3.2 苏木精-伊红染色结果 见图4。对照组深层软骨与钙化软骨之间潮线均匀完整,钙化软骨与软骨下骨之间可见较为明显的黏合线,钙化软骨层完整,可见少量散在的空隙,软骨下骨板连续完整。轻度塌陷组软骨空陷窝增多,钙化软骨层空隙增多增大,软骨与钙化软骨之间出现血管和肉芽侵蚀,破坏潮线完整性,钙化软骨与软骨下骨之间黏合线"
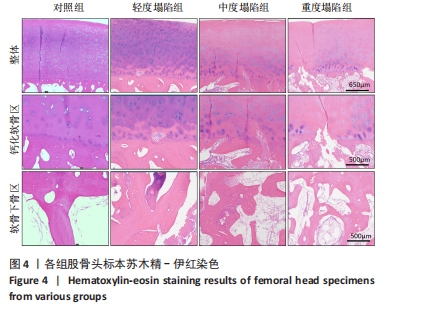
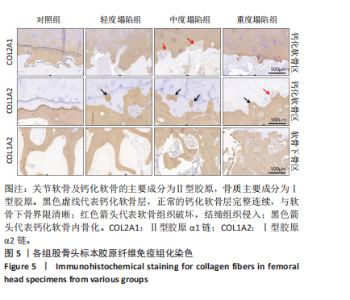
出现中断,可见钙化软骨骨化,软骨下骨板断裂。随着塌陷程度加重,软骨空陷窝增多,钙化软骨层厚度减小、空隙增大,软骨与钙化软骨之间血管和肉芽组织侵蚀现象增多,潮线、黏合线中断或消失,钙化软骨骨化、软骨下骨板断裂分离现象增多,小梁间隙内脂肪细胞、炎性细胞和肉芽组织增多。 2.3.3 免疫组化染色结果 (1)胶原纤维染色结果:见图5。各组透明软骨层和钙化软骨层均可见软骨基质COL2A1强阳性染色。对照组钙化软骨层染色均匀,轻度塌陷组和中度塌陷组钙化软骨层肉芽组织侵入部分染色缺失,重度塌陷组钙化软骨层COL2A1阳性染色面积大幅消失,提示激素性股骨头坏死钙化软骨层破坏严重。"
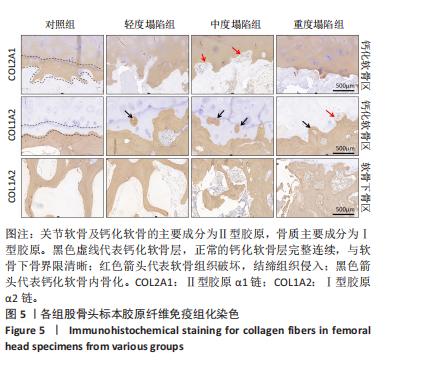

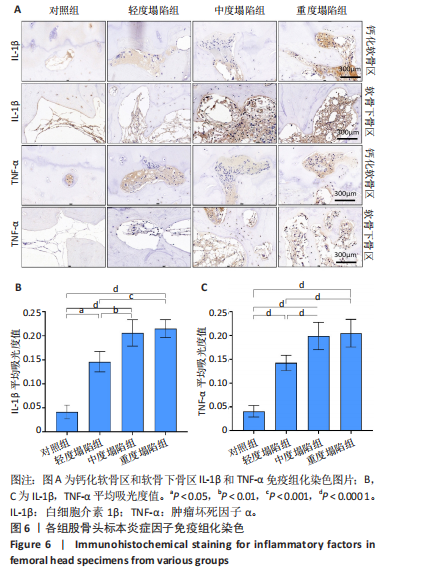
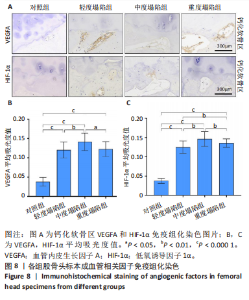
各组软骨下骨区的骨基质COL1A2均呈强阳性表达。对照组钙化软骨与软骨下骨界限分明,连接完好,钙化软骨层分布均匀,软骨骨化现象较少;轻度塌陷组可见钙化软骨散在的软骨骨化现象,钙化软骨完整性被破坏;中度塌陷组钙化软骨层软骨骨化现象增多,钙化软层完整性被破坏;重度塌陷组钙化层面积大幅减少,深层软骨钙化侵蚀,软骨骨化现象明显。在软骨下骨区域,对照组骨小梁排列整齐,空骨陷窝较少,骨间隙仅可见少量脂肪细胞。随着塌陷程度增加,骨小梁排列从有序到紊乱,骨间隙面积减少,结缔组织、肉芽组织增多。 (2)炎症因子染色结果:白细胞介素1β和肿瘤坏死因子α在钙化软骨区及软骨下骨区的表达见图6。对照组的钙化软骨区和骨小梁间隙存在少量的结缔组织和纤维组织,呈白细胞介素1β和肿瘤坏死因子α强阳性染色。轻度塌陷、中度塌陷和重度塌陷组的钙化软骨区和软骨下骨区中结缔组织白细胞介素1β和肿瘤坏死因子α阳性染色细胞明显增多,平均吸光度值相比对照组明显增大(P < 0.05,P < 0.000 1),中度和重度塌陷组平均吸光度值明显大于轻度塌陷组(P < 0.01,P < 0.001,P < 0.000 1),中度塌陷组和重度塌陷组之间没有显著差异(P > 0.05),白细胞介素1β和肿瘤坏死因子α整体表达水平随塌陷程度增加而增大。 (3)基质金属蛋白酶染色结果:钙化软骨区MMP13和MMP3染色结果见图7。对照组钙化软骨层和深层软骨MMP13和MMP3阳性染色细胞较少,轻度塌陷组阳性染色细胞数量增多,集中于钙化软骨层;中度塌陷组深层软骨阳性染色细胞数量增多,染色面积和染色强度增大;重度塌陷组软骨组织呈大面积强阳性染色。轻度塌陷、中度塌陷和重度塌陷组MMP13和MMP3的平均吸光度值均显著大于对照组(P < 0.000 1);中度塌陷组和重度塌陷组MMP13和MMP3平均吸光度值显著大于轻度塌陷组(P < 0.05,P < 0.001);重度塌陷组MMP13的平均吸光度值显著大于轻度塌陷组(P < 0.000 1)。钙化软骨区MMP13和MMP3表达随塌陷程度增加而增大。 (4)成血管相关因子染色结果:钙化软骨区VEGFA和HIF-1α染色结果见图8。对照组钙化软骨层可见少量空隙和阳性细胞;轻度塌陷组钙化软骨层空隙增大,空隙内部阳性细胞数量增多,可见少"

"

"
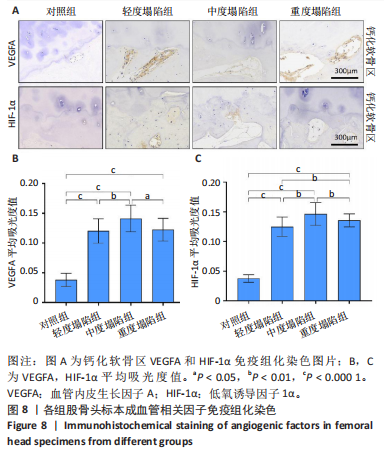
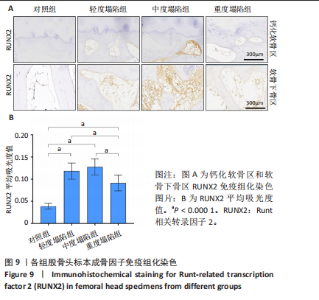
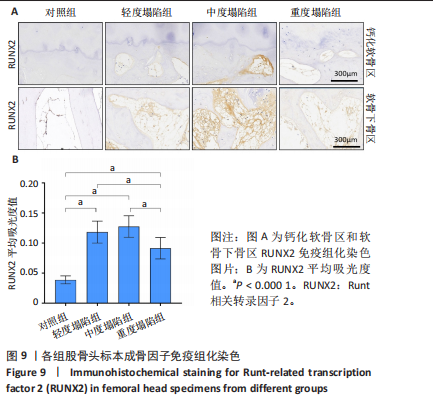
量的内皮细胞和小血管增生;中度塌陷组可见钙化软骨层空隙延伸至深层软骨,染色面积和染色强度增大,内皮细胞和小血管增生增加;重度塌陷组深层软骨可见空隙及阳性染色。轻度、中度和重度塌陷组HIF-1α和VEGFA的平均吸光度值显著大于对照组(P < 0.000 1);中度塌陷组VEGFA和HIF-1α的平均吸光度值显著大于轻度塌陷组(P < 0.01);重度塌陷组HIF-1α的平均吸光度值显著小于中度塌陷组(P < 0.01),VEGFA的平均吸光度值显著小于中度塌陷组(P < 0.05)。在轻中度塌陷中HIF-1α和VEGFA表达随塌陷程度增大而增大,重度塌陷组HIF-1α和VEGFA表达有所下降。 (5)成骨因子染色结果:钙化软骨区和软骨下骨区RUNX2染色结果见图9。对照组钙化软骨区和软骨下骨区几乎没有阳性染色细胞;轻度塌陷组钙化软骨空隙周围和软骨下骨区存在阳性染色;中度和重度塌陷组阳性细胞数增多,染色强度和面积增大。轻度、中度、重度塌陷组RUNX2染色的平均吸光度值显著高于对照组(P < 0.000 1),轻度塌陷组和中度塌陷组平均吸光度值没有明显的变化(P > 0.05),重度塌陷组平均吸光度值相对轻度、中度塌陷组减小(P < 0.000 1)。激素性股骨头坏死标本中RUNX2表达增加,重度塌陷组RUNX2表达相对下降。"

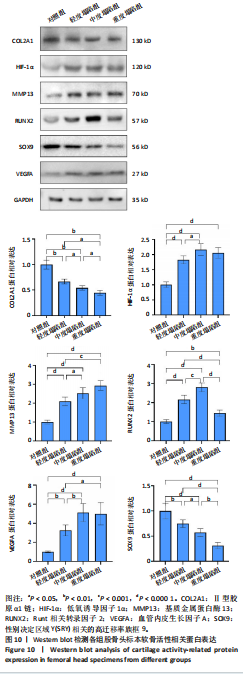
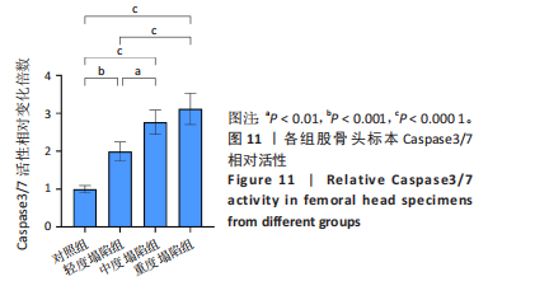
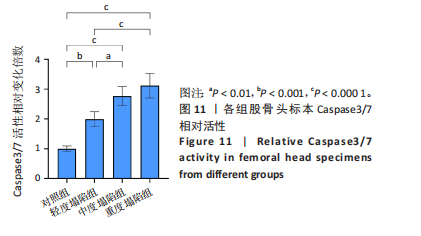
2.4 Western blot检测结果 各组股骨头标本软骨活性相关蛋白见图10。激素性股骨头坏死患者股骨头样本中COL2A1和转录因子SOX9蛋白表达显著低于对照组(P < 0.01,P < 0.000 1),与塌陷程度呈负相关,MMP13蛋白表达高于对照组(P < 0.000 1),与塌陷程度呈正相关。此外,成骨相关因子RUNX2在激素性股骨头坏死患者中的表达显著增加(P < 0.01,P < 0.000 1),重度塌陷组RUNX2表达相对轻度和中度塌陷组下降(P < 0.001,P < 0.000 1),HIF-1α和VEGFA在激素性股骨头坏死患者中的表达也显著增加(P < 0.01,P < 0.000 1)。 2.5 软骨凋亡检测结果 Caspase3/7活性测定试剂盒检测结果见图11,结果显示激素性股骨头坏死患者股骨头样本的Caspase3/7活性显著高于对照组(P < 0.001,P < 0.000 1),且Caspase3/7的活性与股骨头塌陷程度呈正相关。"
"
| [1] DIMA A, PEDERSEN AB, PEDERSEN L, et al. Association of common comorbidities with osteonecrosis: a nationwide population-based case-control study in Denmark. BMJ Open. 2018;8(2):e020680. [2] MIMURA N, IWAMOTO T, FURUTA S, et al. Prevalence and risk factors of osteonecrosis of the femoral head in patients with ANCA-associated vasculitis: a multicentre cohort study. RMD Open. 2023;9(1):e002787. [3] KWON HM, HAN M, LEE TS, et al. Effect of Corticosteroid Use on the Occurrence and Progression of Osteonecrosis of the Femoral Head: A Nationwide Nested Case-Control Study. J Arthroplasty. 2024; 39(10):2496-2505.e1. [4] SHIMIZU H, SHIMIZU T, TAKAHASHI D, et al. Corticosteroid dose increase is a risk factor for nonalcoholic fatty liver disease and contralateral osteonecrosis of the femoral head: a case report. BMC Musculoskelet Disord. 2019;20(1):88. [5] LOU P, ZHOU G, WEI B, et al. Sclerotic zone in femoral head necrosis: from pathophysiology to therapeutic implications. EFORT Open Rev. 2023;8(6):451-458. [6] YIXUAN H, XINWEI Y, FEIFEI G, et al. Effect of Sclerosis Bands in Femoral Head Necrosis on Non-Vascularized Fibular Grafting-A Finite Element Study. Orthop Surg. 2024;16(10):2526-2538. [7] LIU LH, ZHANG QY, SUN W, et al. Corticosteroid-induced Osteonecrosis of the Femoral Head: Detection, Diagnosis, and Treatment in Earlier Stages. Chin Med J (Engl). 2017;130(21):2601-2607. [8] NAKAMURA J, FUKUSHIMA W, ANDO W, et al. Time elapsed from definitive diagnosis to surgery for osteonecrosis of the femoral head: a nationwide observational study in Japan. BMJ Open. 2024; 14(3):e082342. [9] CHENG L, WANG S. Correlation between bone mineral density and sarcopenia in US adults: a population-based study. J Orthop Surg Res. 2023;18(1):588. [10] LI WL, TAN B, JIA ZX, et al. Exploring the Risk Factors for the Misdiagnosis of Osteonecrosis of Femoral Head: A Case-Control Study. Orthop Surg. 2020;12(6):1792-1798. [11] CHANG C, GREENSPAN A, GERSHWIN ME. The pathogenesis, diagnosis and clinical manifestations of steroid-induced osteonecrosis. J Autoimmun. 2020;110:102460. [12] RAKHSHANKHAH N, ABBASZADEH M, KAZEMI A, et al. Deep learning approach to femoral AVN detection in digital radiography: differentiating patients and pre-collapse stages. BMC Musculoskelet Disord. 2024;25(1):547. [13] NAM KW, KIM YL, YOO JJ, et al. Fate of untreated asymptomatic osteonecrosis of the femoral head. J Bone Joint Surg Am. 2008;90(3): 477-484. [14] MONT MA, ZYWIEL MG, MARKER DR, et al. The natural history of untreated asymptomatic osteonecrosis of the femoral head: a systematic literature review. J Bone Joint Surg Am. 2010;92(12): 2165-2170. [15] LIEBERMAN JR, ENGSTROM SM, MENEGHINI RM, et al. Which factors influence preservation of the osteonecrotic femoral head? Clin Orthop Relat Res. 2012;470(2):525-534. [16] MONT MA, CHERIAN JJ, SIERRA RJ, et al. Nontraumatic Osteonecrosis of the Femoral Head: Where Do We Stand Today? A Ten-Year Update. J Bone Joint Surg Am. 2015;97(19):1604-1627. [17] 魏秋实,庞凤祥,陈哓俊,等.经髋关节外科脱位打压植骨支撑术治疗ARCO Ⅲ期股骨头坏死的临床疗效分析[J].中华损伤与修复杂志(电子版),2020,15(2):90-95. [18] WEI W, TAN B, YAN Y, et al. Hip Preservation or Total Hip Arthroplasty? A Retrospective Case-Control Study of Factors Influencing Arthroplasty Decision-Making for Patients with Osteonecrosis of the Femoral Head in China. Orthop Surg. 2023;15(3):731-739. [19] 中国医师协会骨科医师分会骨循环与骨坏死专业委员会,中华医学会骨科分会骨显微修复学组,国际骨循环学会中国区.中国成人股骨头坏死临床诊疗指南(2020)[J].中华骨科杂志,2020, 40(20):12. [20] 中国微循环学会骨微循环专业委员会,徐鑫,时利军,等.股骨头坏死临床诊疗技术专家共识(2022年)[J].中国修复重建外科杂志, 2022,36(11):1319-1326. [21] 中华医学会骨科学分会创伤骨科学组,中国医师协会骨科医师分会创伤专家工作委员会.成人股骨颈骨折诊治指南[J].中华创伤骨科杂志,2018,20(11):921-928. [22] HE Y, GRAM A, SIMONSEN O, et al. AB0104 Develop and Evaluate a New Modified Mankin Score System with Special Attention to Subchondral Bone. Ann Rheum Dis. 2014;73(Suppl 2):838. [23] RIZZARDI AE, JOHNSON AT, VOGEL RI, et al. Quantitative comparison of immunohistochemical staining measured by digital image analysis versus pathologist visual scoring. Diagn Pathol. 2012;7:42. [24] YOON BH, MONT MA, KOO KH, et al. The 2019 Revised Version of Association Research Circulation Osseous Staging System of Osteonecrosis of the Femoral Head. J Arthroplasty. 2020;35(4):933-940. [25] ZHANG QY, LI ZR, GAO FQ, et al. Pericollapse Stage of Osteonecrosis of the Femoral Head: A Last Chance for Joint Preservation. Chin Med J (Engl). 2018;131(21):2589-2598. [26] 魏秋实,何伟,张庆文,等.围塌陷期股骨头坏死不同影像学表现研究[J].中国修复重建外科杂志,2021,35(9):1105-1110. [27] HATANAKA H, MOTOMURA G, IKEMURA S, et al. Volume of hip synovitis detected on contrast-enhanced magnetic resonance imaging is associated with disease severity after collapse in osteonecrosis of the femoral head. Skeletal Radiol. 2019;48(8):1193-1200. [28] 魏秋实,杨帆,陈哓俊,等.激素性与酒精性股骨头坏死患者骨标本坏死区域病理与显微结构特点分析[J].中国修复重建外科杂志,2018,32(7):866-872. [29] 张德志,胡蕴玉,费正奇,等.激素性骨坏死关节软骨下皮质骨病理改变的实验研究[J].中国矫形外科杂志,2006,14(10):769-771. [30] MA J, GE J, CHENG L, et al. Subchondral Bone Plate Classification: A New and More Sensitive Approach for Predicting the Prognosis of Osteonecrosis of the Femoral Head. Cartilage. 2023;14(3):269-277. [31] MURPHY G, LEE MH. What are the roles of metalloproteinases in cartilage and bone damage? Ann Rheum Dis. 2005;64 Suppl 4(Suppl 4):iv44-47. [32] GOLDRING MB, OTERO M, PLUMB DA, et al. Roles of inflammatory and anabolic cytokines in cartilage metabolism: signals and multiple effectors converge upon MMP-13 regulation in osteoarthritis. Eur Cell Mater. 2011;21:202-220. [33] WOO S, LEE Y, SUN D. A Pilot Experiment to Measure the Initial Mechanical Stability of the Femoral Head Implant in a Cadaveric Model of Osteonecrosis of Femoral Head Involving up to 50% of the Remaining Femoral Head. Medicina (Kaunas). 2023;59(3):508. [34] HALL M, VAN DER ESCH M, HINMAN RS, et al. How does hip osteoarthritis differ from knee osteoarthritis? Osteoarthritis Cartilage. 2022;30(1):32-41. [35] WANG C, MENG H, WANG Y, et al. Analysis of early stage osteonecrosis of the human femoral head and the mechanism of femoral head collapse. Int J Biol Sci. 2018;14(2):156-164. [36] CHEN Y, MIAO Y, LIU K, et al. Less sclerotic microarchitecture pattern with increased bone resorption in glucocorticoid-associated osteonecrosis of femoral head as compared to alcohol-associated osteonecrosis of femoral head. Front Endocrinol (Lausanne). 2023; 14:1133674. [37] CHEN Y, YU Y, WEN Y, et al. A high-resolution route map reveals distinct stages of chondrocyte dedifferentiation for cartilage regeneration. Bone Res. 2022;10(1):38. [38] GOLDRING SR, GOLDRING MB. Changes in the osteochondral unit during osteoarthritis: structure, function and cartilage-bone crosstalk. Nat Rev Rheumatol. 2016;12(11):632-644. [39] FONDI C, FRANCHI A. Definition of bone necrosis by the pathologist. Clin Cases Miner Bone Metab. 2007;4(1):21-26. [40] EVANS LAE, PITSILLIDES AA. Structural clues to articular calcified cartilage function: A descriptive review of this crucial interface tissue. J Anat. 2022;241(4):875-895. [41] MAHJOUB M, BERENBAUM F, HOUARD X. Why subchondral bone in osteoarthritis? The importance of the cartilage bone interface in osteoarthritis. Osteoporos Int. 2012;23 Suppl 8:S841-846. [42] IMHOF H, BREITENSEHER M, KAINBERGER F, et al. Importance of subchondral bone to articular cartilage in health and disease. Top Magn Reson Imaging. 1999;10(3):180-192. [43] BOYDE A. The Bone Cartilage Interface and Osteoarthritis. Calcif Tissue Int. 2021;109(3):303-328. [44] PARK S, BELLO A, ARAI Y, et al. Functional Duality of Chondrocyte Hypertrophy and Biomedical Application Trends in Osteoarthritis. Pharmaceutics. 2021;13(8):1139. [45] DENG B, WANG F, YIN L, et al. Quantitative study on morphology of calcified cartilage zone in OARSI 0~4 cartilage from osteoarthritic knees. Curr Res Transl Med. 2016;64(3):149-154. [46] WANG X, WU Q, ZHANG R, et al. Stage-specific and location-specific cartilage calcification in osteoarthritis development. Ann Rheum Dis. 2023;82(3):393-402. [47] 陈雷雷,何伟.股骨头缺血性坏死相关生物力学研究进展[J].中国骨伤,2011,24(2):174-177. [48] WANG P, WANG C, MENG H, et al. The Role of Structural Deterioration and Biomechanical Changes of the Necrotic Lesion in Collapse Mechanism of Osteonecrosis of the Femoral Head. Orthop Surg. 2022;14(5):831-839. [49] YU Y, WANG S, ZHOU Z. Cartilage Homeostasis Affects Femoral Head Necrosis Induced by Methylprednisolone in Broilers. Int J Mol Sci. 2020;21(14):4841. [50] CHEN L, HONG G, FANG B, et al. Predicting the collapse of the femoral head due to osteonecrosis: From basic methods to application prospects. J Orthop Translat. 2017;11:62-72. [51] LIU Y, MA Y, YANG W, et al. Integrated proteomics and metabolomics analysis of sclerosis-related proteins and femoral head necrosis following internal fixation of femoral neck fractures. Sci Rep. 2024; 14(1):13207. [52] WANG Y, SUN D, ZHANG J, et al. Multi-sequence MRI-based radiomics: An objective method to diagnose early-stage osteonecrosis of the femoral head. Eur J Radiol. 2024;177:111563. [53] HAN X, HONG G, GUO Y, et al. Novel MRI technique for the quantification of biochemical deterioration in steroid-induced osteonecrosis of femoral head: a prospective diagnostic trial. J Hip Preserv Surg. 2021;8(1):40-50. [54] OUYANG W, GUO G, XIA J, et al. Arthroscopic assisted versus open core decompression for osteonecrosis of the femoral head: A systematic review and meta-analysis. PLoS One. 2024;19(11):e0313265. [55] 林天烨,吴智明,张文胜,等.复方生脉成骨胶囊修复激素性股骨头坏死的作用机制[J].中国组织工程研究,2024,28(2):200-207. |
| [1] | Li Hao, Tao Hongcheng, Zeng Ping, Liu Jinfu, Ding Qiang, Niu Chicheng, Huang Kai, Kang Hongyu. Mitogen-activated protein kinase signaling pathway regulates the development of osteoarthritis: guiding targeted therapy with traditional Chinese medicine [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(6): 1476-1485. |
| [2] | Wang Zhengye, Liu Wanlin, Zhao Zhenqun. Advance in the mechanisms underlying miRNAs in steroid-induced osteonecrosis of the femoral head [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(5): 1207-1214. |
| [3] | Chen Yixian, Chen Chen, Lu Liheng, Tang Jinpeng, Yu Xiaowei. Triptolide in the treatment of osteoarthritis: network pharmacology analysis and animal model validation [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(4): 805-815. |
| [4] | Yang Xiao, Bai Yuehui, Zhao Tiantian, Wang Donghao, Zhao Chen, Yuan Shuo. Cartilage degeneration in temporomandibular joint osteoarthritis: mechanisms and regenerative challenges [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(4): 926-935. |
| [5] | Xu Peng, Jiang Wei, Yu You, Lei Zhengliang, Tian Yang, Zhang Jie, Liu Luchang. Cobalt chloride-induced hypoxic environment accelerates knee cartilage degeneration in New Zealand rabbits [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(22): 5650-5658. |
| [6] | Han Jie, Hu Tianfa, Wu Yachao, Nong Bin, Yu Kailong. Forkhead box transcription factor O3 affects bone metabolism and participates in the pathological processes of various bone-related diseases [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(22): 5770-5781. |
| [7] | Zheng Wen, Zhu Dongsheng, Wang Xiaodong. Secreted modular calcium binding protein regulates autophagy in the acetabular cartilage of rats with developmental dysplasia of the hip [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(18): 4618-4626. |
| [8] | Lin Yong, Yang Xiaoqiang, Lin Kun, Yang Fan, He Mincong, Wei Qiushi. Immune microenvironment and inflammatory repair of cystic degeneration in steroid-induced osteonecrosis of the femoral head: a single-cell sequencing analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(17): 4309-4317. |
| [9] | Chen Xinlong, Meng Tao, Wang Yaomin, Zhang Kefan, Li Jian, Shi Hui, Zhang Chenchen. Ferroptosis inhibitors in the treatment of osteoarthritis: diversity and multitarget characteristics [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(16): 4166-4179. |
| [10] | Wang Zhengye, Liu Wanlin, Zhao Zhenqun. Multidimensional target regulation of vascular endothelial growth factor A in articular cartilage development [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(16): 4193-4203. |
| [11] | Wu Tianyi, Miao Yiming, Wan Kaichen, Teng Yun, Zou Jun. Protective effect of mesoporous ZLN005@polydopamine nanoparticles on chondrocytes in osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(14): 3576-3585. |
| [12] | Jiang Yidi, Zhao Jianwei, Zhou Jue, Lyu Jinpeng, Wang Datao, Li Xunsheng, Yue Zhigang, Cui Bo, Sun Hongmei. Regulation of antler stem cell exosomes miRNA-145 on inflammatory chondrocytes [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(13): 3288-3297. |
| [13] | Li Yijin, Li Jiahao, Zhang Haitao, Huang Yiwei, Chen Jinlun, Zeng Yirong, Feng Wenjun. GJK Tablets intervene in cartilage homeostasis to protect articular cartilage of mice with knee osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(12): 2994-3004. |
| [14] | Ke Yanqin, Yuan Jie, He Guanghui, Zhang Xiaoling. Remimazolam inhibits chondrocyte senescence and alleviates osteoarthritis: roles and mechanisms [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(12): 3005-3013. |
| [15] | Lu Yuchun, Zhu Zimo, Li Chaomeng, Liu Ju, Jiang Zixian, Li Xiufang, Wang Tao, Wang Wenjing. Effect and mechanism of dichloromethane extract of fresh Sambucus adnata Wall. in rat osteoarthritis models [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(12): 3014-3028. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||