Chinese Journal of Tissue Engineering Research ›› 2021, Vol. 25 ›› Issue (24): 3908-3913.doi: 10.12307/2021.101
Previous Articles Next Articles
Etiology and treatment of femoral trochlear dysplasia: congenital genetic determination or stress stimulation of patella
Zhou Yuanbo, Wang Jindong
- Department of Orthopedics, Second Hospital of Shanxi Medical University, Taiyuan 030000, Shanxi Province, China
-
Received:2020-11-06Revised:2020-11-11Accepted:2020-11-26Online:2021-08-28Published:2021-03-18 -
Contact:Wang Jindong, MD, Associate chief physician, Associate professor, Department of Orthopedics, Second Hospital of Shanxi Medical University, Taiyuan 030000, Shanxi Province, China -
About author:Zhou Yuanbo, Master candidate, Department of Orthopedics, Second Hospital of Shanxi Medical University, Taiyuan 030000, Shanxi Province, China
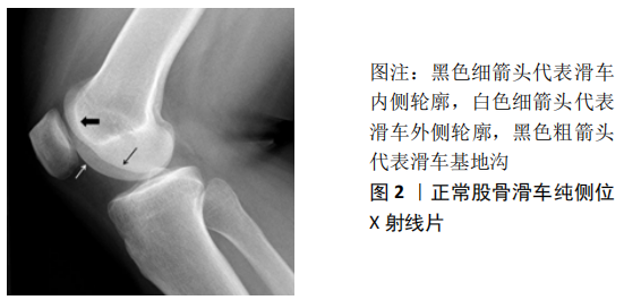
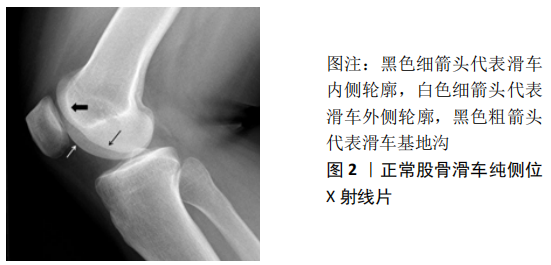
2.1 滑车发育不良的病因 目前有关滑车发育不良的病因尚没有定论,现主要有两大观点,一些学者认为滑车发育不良是先天基因决定的,而也有一些学者认为与后天髌骨的应力刺激有关。 2.1.1 滑车发育与基因有关 有各种各样的研究支持了滑车发育是先天基因决定的。最初,GARRON等[8]和GLARD等[9]对胎儿尸体的股骨滑车形态进行了测量,发现胎儿的滑车沟角以及内外侧滑车倾斜角与成人没有统计学差异,提示滑车形态在胎儿期就已经发育成型。为进一步观察滑车形态是否随时间而改变,一些学者发现超声是测量股骨滑车的安全且有效工具[10-11],?YE等[12]采用超声对174名新生儿的滑车沟角进行测量,并分为滑车不良组(沟角>159°)和正常组(沟角<159°),随后对15例滑车不良的膝关节和101例正常的膝关节在第6,18,72个月进行随访,结果发现研究对象从新生儿到6岁这段时期,滑车不良组和正常组的滑车沟角都发生了具有统计学差异的变化,滑车不良组平均沟角从161°变化到158.3°,正常组平均沟角从149.5°变化到151.6°,但这种变化很微小,而且这种变化主要发生在前18个月,提示后天对股骨滑车的塑形并不产生明显的影响。 2.1.2 滑车发育与髌骨的应力刺激有关 一系列动物实验证明滑车的发育与髌骨的应力刺激密切相关,国内外一些学者通过手术干预将兔子的髌骨造成位置不良或脱位状态,与对照组相比,手术干预组的滑车出现了发育不良[13-17],说明髌骨的位置不良不能给滑车造成充分的应力刺激,从而影响滑车的发育。最近,LU等[17]将一组幼兔的髌骨切除,术后3个月对照组与髌骨切除组在软骨层面的滑车沟角有统计学差异[(144.2±1.5)°vs. (151.9±2.4)°,P < 0.001],术后6个月对照组与髌骨切除组在骨性层面的滑车沟角出现统计学差异[(136.2±2.2)°vs. (160.4±2.6)°,P < 0.001],而且另外一个研究结果显示幼兔髌骨的早期复位会阻止滑车发育不良的发 生[18],这些兔子研究实验都充分支持了髌骨的应力刺激对滑车发育至关重要。 在人体方面,胎位为臀先露的新生儿滑车发育不良的发生率是头先露的15倍,胎位为膝关节伸直状态下的新生儿滑车发育不良的发生率是膝关节可以自由屈伸状态下的45倍[19],这表明在妊娠晚期,胎儿屈膝状态产生的髌骨应力刺激对股骨滑车发育至关重要。FERLIC等[20]利用CT测量了髌骨高度和股骨滑车发育形态的指标,发现高位的髌骨与滑车发育不良具有相关性,例如滑车沟角(r=0.344,P=0.005)、滑车面的不对称性(r=-0.399,P=0.005)、滑车中心高度(r=0.490,P < 0.001)等。LIEBENSTEINER等[21]发现股骨前倾角过大与滑车发育不良也相关,作者认为股骨前倾角过大会改变髌股关节的内外侧压力,进而影响滑车发育的形态。 在上述理论的支持下,付琨朋[22]通过对23例患有双侧复发性髌骨脱位伴滑车发育不良儿童(平均年龄7.6岁,5-11岁)的一侧膝关节行内侧髌骨支持带成形术,而对侧膝关节保守治疗,术前CT测量两侧的滑车形态学指标没有差异,而术后随访48个月发现,手术侧的滑车形态较保守治疗侧明显改善,说明及早手术干预会改善滑车发育的形态。对于手术干预时间的选择,RAJDEV等[23]对20例10岁以上髌骨不稳的儿童行内侧髌骨支持带成形术,术后随访滑车形态并没有变化,而1例10岁以下的儿童术后随访发现滑车形态得到改善,建议对10岁以下的儿童行髌骨稳定的手术。 2.2 滑车的影像学评估 正常股骨滑车面的形态类似“U”形,从近端到远端“U”形逐渐变陡变深,而滑车发育不良可定义为滑车的沟槽或内外侧滑车面的骨性异常,特征是滑车面平坦或沟浅,最早是由瑞典BRATTSTROM教授[24]提出,为了进一步评估滑车的形态,以下将从X射线片、CT/MRI、滑车发育不良的分型等内容来评估滑车的发育形态。 2.2.1 滑车的X射线片评估 在膝关节纯侧位X射线片上(股骨内外侧后髁完全重叠),正常股骨滑车前方可以看到3条致密的线条(图2),最前面的2条致密线条代表内外侧髁的轮廓(黑色细箭头代表滑车内侧轮廓,白色细箭头代表滑车外侧轮廓),这2条线几乎重叠,后方的致密线代表滑车沟的基地线(黑色粗箭头代表滑车基地沟),这条线完全位于股骨内外侧髁轮廓线的后方,意味着滑车沟低于滑车的内外侧壁。而滑车发育不良的X射线片会产生3个征象:①滑车沟的基地线与股骨外侧髁的轮廓线相交叉,则视为交叉征,意味着滑车沟发育扁平;②滑车沟的基地线位于股骨干前方皮质延长线的前方,则视为突起征,突起征大于3 mm则可诊断为滑车发育不良[25],该征象意味着滑车近端整体抬高,对髌骨轨迹产生类似“滑雪跳台”的作用;③滑车内外侧髁的轮廓线彼此分开,则视为双线征,意味着滑车内侧髁发育低平。 "
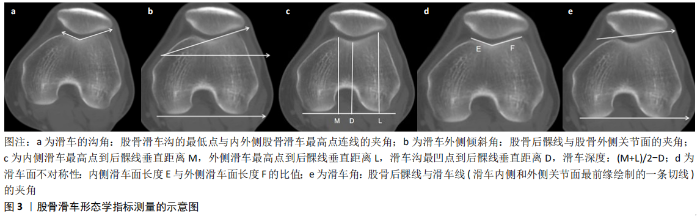
尽管上述描述的3个征象能很好地帮助医生诊断滑车不良,但实际运用的困难在于它要求X射线片必须是纯侧位,KO?TER等[26]发现膝关节侧位X射线片对诊断滑车发育不良并不可靠,因为下肢外旋10°,正常滑车会出现假阳性的交叉征,如果下肢内旋5°,滑车面发育平坦的交叉征会出现假阴性,因此,利用X射线片诊断滑车发育不良并不是特别可靠的工具。 2.2.2 滑车的CT/MRI评估 采用CT或者MRI的横断位片可以对滑车形态量化评估。通常情况下,CT选择的横断面是从近端往远端扫描刚进入滑车后再远端5 mm的层面[20],MRI选择的横断面在从近端往远端扫描出现第1张具有完整软骨滑车的层面[27]。以下是临床上常用的量化滑车发育不良的指标(图3):①滑车的沟角是股骨滑车沟的最低点与内外侧股骨滑车的最高点连线的夹角,沟角大于145°被认为滑车发育不良[28],最新的1篇包含1 204例患者的荟萃分析表明[29],在滑车的软骨层面测量,正常组的滑车沟角平均为141.83°(95% 置信区间:139.90°?-?143.76°),而髌股关节不稳组的滑车沟角平均为156.24 °(95% 置信区间:153.71°-158.77°);在软骨下骨层面测量,正常组的滑车沟角平均为133.69°(95% 置信区间:131.23°-136.15°),而髌股关节不稳组的滑车沟角平均为148.42°(95% 置信区间:144.02°-152.82°);②滑车外侧倾斜角是股骨后髁线与滑车外侧关节面的夹角[30],其值小于11°可诊断为滑车发育不良(敏感性93%,特异性87%)[30],而且该角度被评价为临床上最为实用且测量结果最为可靠[31];③计算滑车的深度需要先测量内侧滑车最高点到后髁线垂直距离M和外侧滑车最高点到后髁线垂直距离L以及滑车沟最凹点到后髁线垂直距离D,滑车的深度是(M+L)/2-D,其值小于3 mm可诊断为滑车发育不良(敏感性100%,特异性96%)[30];④滑车面不对称性定义为内侧滑车面长度与外侧滑车面长度的比值,其值小于2∶5可诊断为滑车发育不良(敏感性100%,特异性96%)[30];⑤DONG等[32]发现滑车角是一个可靠且能量化滑车发育严重程度的指标,滑车角是股骨后髁线与滑车线(滑车内侧和外侧关节面最前缘绘制的一条切线)的夹角,其值大于8°可诊断为滑车发育不良(敏感性82%,特异性79%)。以上指标均可量化滑车发育的严重程度。 2.2.3 滑车发育不良的分型 临床上最经典滑车发育不良的分型方法是Dejour分型,这种分型是结合膝关节X射线侧位片与轴位CT片。A型:X射线片只存在交叉征,轴位CT显示滑车沟浅,沟角大于145°;B型:X射线片存在交叉征和突起征,轴位CT显示滑车沟扁平;C型:X射线片存在交叉征和双线征,轴位CT显示外侧滑车形态异常呈凸轮状,内侧滑车发育不全;D型:X射线片存在交叉征、双线征和突起征,轴位CT显示外侧滑车形态异常呈凸轮状,内侧滑车发育不全,内外侧滑车之间呈现“悬崖征”。这种分型方法不仅反映滑车发育不良的严重程度,在指导滑车成形术方面也有重大意义[33]。 尽管Dejour分型法广泛应用,但是这种方法存在一致性和可重复性差的问题。LIPPACHER等[34]发现Dejour的4型分型法一致性一般(24%-78%),但当把滑车发育不良分成2型时,即轻度滑车发育不良为A型和重度滑车发育不良BCD型,一致性有了明显的提高(56%-96%)。TSCHOLL等[35]也发现Dejour分型分为2型的一致性要好于分为4型,同时发现轴位MRI选择的层面不同对分型的一致性也会产生影响,建议选取髌骨中间高度的位置作为轴位层面能获得更高的一致性。随着3D打印在医学领域的应用,FRITZ等[36]发现采用3D打印股骨滑车可以帮助临床医师提高滑车发育不良的诊断率,但并不能帮助临床医师提高Dejour分型法的正确率。以上都说明Dejour 4类分型法存在着不足。 最近,SHARMA等[37]根据轴位MRI创造了一种新的分型方法,OBC(Oswestry-Bristol Classification)分型法,它将滑车发育不良分成4型。正常型:滑车发育形态正常;轻度滑车发育不良:滑车沟较浅;中度滑车发育不良:滑车面平坦;重度滑车发育不良:滑车面突起。OBC分型方法组间一致性(Kappa=0.58)要好于Dejour分型法(Kappa=0.44),对于复发性髌骨患者的术式选择方面,该分型方法系统且有科学指导性。 还有学者提出在关节镜下能直观对滑车发育不良进行分型[38],Ⅰ型:滑车沟较浅,整个滑车面相比股骨干的皮质有整体抬高;Ⅱ型:近端滑车面突出,外侧滑车异常突起,远端滑车面平坦并伴有内侧滑车发育不良。这种分型方法组间和组内一致性高达81%-92%。该作者建议Ⅰ型患者采用内侧髌骨支持带成形术即足以解决问题,Ⅱ型患者可考虑采用滑车成形术。 2.3 滑车发育不良带来的临床问题 2.3.1 滑车发育不良与髌股关节不稳 髌股关节不稳可定义为在膝关节屈伸时髌骨相对于股骨滑车的异常的运动轨迹,严重者可导致髌骨脱位,是骨科常见的问题,好发于青少 年[1],患者可表现为膝前痛、打软腿,甚至反复摔倒等症状。髌骨的稳定性受骨性与软组织的影响,比如股骨滑车发育不良、高位髌骨、膝外翻、过大的股骨和胫骨扭转畸形、过大的胫骨结节-滑车沟距离、内侧髌股韧带损伤、股内外侧斜肌不平衡等[2-4],其中滑车发育不良逐渐被证明为最主要的危险因素[5-7,39],有学者报道对于年龄小于25岁且伴有滑车发育不良的初次髌骨脱位患者,5年内再次脱位的发生率高达60%-70%[40]。 股骨滑车是髌骨的重要骨性稳定结构,一个发育正常的滑车对有脱位倾向的髌骨提供机械性阻挡。有限元分析表明滑车外侧倾斜角减小会导致髌骨出现更大的外侧偏移[41]。在尸体上的生物力学实验也揭示了滑车发育不良对髌股关节的影响[42]:①在膝关节屈伸过程中,滑车发育不良的膝关节会出现更大的髌骨外倾和髌骨内旋,这在Dejour D型尤为明显;②滑车发育不良有更大的髌股关节压力和较小的髌股关节接触面积,这个现象在Dejour B、D型比DejourA、C型明显;③当对髌骨施加100 N的外侧拉力时,滑车发育不良组的髌骨比正常组平均多外移了3 mm(P=0.003)。以上均说明滑车发育不良与不良的髌骨轨迹密切相关。 2.3.2 滑车发育不良与软骨磨损 上述生物力学实验证明滑车发育不良会增大髌股关节之间的压力,提示滑车发育不良也许会加速软骨的磨损。国内有学者通过MRI发现,滑车发育不良会引起滑车外侧面和髌骨外侧面的软骨损伤,其中Dejour B、C、D型的滑车发育不良可引起更广泛的软骨损伤[43]。国外也有学者报道有单独髌股关节炎的患者存在滑车发育不良的比例明显高于对照组(55% vs. 6%)[44]。另外,也有学者发现滑车深度减低(小于3 mm)或内外侧关节面比例下降(小于0.4)或过大的滑车沟角(大于170°)与更糟糕的WORMS评分(软骨病变评分方法)存在联系[45]。 2.3.3 滑车发育不良与前叉韧带损伤 滑车发育不良也是前交叉韧带损伤的一个危险因素,有研究报道,前交叉韧带损伤患者滑车发育不良的发病率要明显大于正常组(15.45% vs. 4.5%)[46]。国内有学者也报道了前交叉韧带损伤患者的滑车发育不良的发病率是30.7%,而对照组只有14.4%,而且前交叉损伤患者比对照组有更大的滑车沟角、更小的内外侧关节面比例和更小的外侧倾斜角(P < 0.01)[47]。当然,目前关于滑车发育不良与前交叉韧带损伤之间关系的文章并不多,将来还需要进一步的研究来探索两者存在关系的原因。 2.4 滑车成形术 滑车成形术的目的是纠正滑车异常的形态,可以重塑滑车沟的位置、加深滑车沟的深度、消除突起征等,从而恢复髌骨相对滑车的正常的运动轨迹。有关滑车成形术的历史起源最早可追溯到1890年,英国Pollard医生发现异常的滑车形态并尝试通过手术来纠正它[48],如今,滑车成形术已发展成熟,主要包括外侧滑车抬高术、滑车沟加深术、滑车楔形下压成形术、关节镜下Bereiter滑车成形术。 2.4.1 滑车成形术的适应证与禁忌证 为更好地从滑车成形术中受益,把握好适应证与禁忌证至关重要[49]。适应证应满足以下条件:①复发性髌骨脱位;②保守治疗无效;③滑车发育不良分型为Dejour B、C、D型;④患者骨骺已闭合或接近闭合。 绝对禁忌证包括:①先天性髌骨脱位;②严重的髌股关节炎;③滑车发育不良分型为Dejour A型;④骨骺尚未闭合的患者。 相对禁忌证包括:①股骨的扭转畸形角度>30°;②膝关节存在内翻或外翻畸形;③胫骨的扭转畸形>25°;④高位髌骨(Caton指数>1.6)。 2.4.2 滑车成形术的临床效果 许多研究都证实了滑车成形术能获得让患者满意的临床效果,但也可能出现软骨损伤、关节僵硬等并发症。首先,在尸体上的生物力学实验表明,对模拟滑车发育不良的膝关节行滑车成形术,术后髌骨的稳定性可恢复至正常[50]。在术后影像学评估方面,对患者行滑车成形术结合内侧髌骨韧带重建术,术后MRI评估发现髌骨与滑车的对合关系可恢复到正常人水平[51]。在术后随访方面,CARSTENSEN等[52]对行滑车沟加深术结合内侧髌骨韧带重建术的67例复发性髌骨脱位患者随访2-6.8年,术后膝关节功能评分(IKDC评分、Kujala评分)较术前都有明显改善(P < 0.001),患者术后满意率高达91%,有84.8%的患者可参加运动,但有8例出现了膝关节僵硬的并发症。同样,也有学者对17例患者行外侧滑车抬高术的膝关节随访时间长达25年,没有一例膝关节出现再次脱位的情况,术后16年膝关节功能评分(Lille评分)为90±15,术后25年评分为86±23,只有4例膝关节出现了较为严重的关节炎而做了关节置换手术,该学者认为滑车成形术并不会加快软骨的磨损[53]。 滑车成形术结合其他术式的临床效果要好于单独滑车成形术[54],但滑车成形术相比单独的其他术式是否有优势目前还没有取得一致的结论,BALCAREK等[55]通过荟萃分析表明单独的内侧髌骨韧带重建术与滑车成形术结合其他术式都能取得令人满意的临床效果,但滑车成形术结合其他术式会有更低的复发率(7% vs. 2.1%)。然而,ZAFFAGNINI等[56]也通过荟萃分析表明单独的内侧髌骨韧带重建术与滑车成形术结合内侧髌骨韧带重建术相比,在提高膝关节功能评分与髌骨再次脱位率方面,两种手术方式没有统计学差异,但滑车成形术结合内侧髌骨韧带重建术会带来更高的膝关节僵硬的风险。 "

| [1] SANDERS TL, PAREEK A, HEWETT TE, et al. Incidence of First-Time Lateral Patellar Dislocation: A 21-Year Population-Based Study. Sports Health. 2018;10(2):146-151. [2] IRGER M, ACHTNICH A, IMHOFF AB, et al. Diagnosis and therapy of chronic patellofemoral instability. Orthopade. 2020;49(1):73-84. [3] WEBER AE, NATHANI A, DINES JS, et al. An Algorithmic Approach to the Management of Recurrent Lateral Patellar Dislocation. J Bone Joint Surg Am. 2016;98(5):417-427. [4] PARIKH SN, LYKISSAS MG, GKIATAS I. Predicting Risk of Recurrent Patellar Dislocation. Curr Rev Musculoskelet Med. 2018;11(2):253-260. [5] SUNDARARAJAN SR, RAJ M, RAMAKANTH R, et al. Prediction of recurrence based on the patellofemoral morphological profile and demographic factors in first-time and recurrent dislocators. Int Orthop. 2020;44(11):2305-2314. [6] HUNTINGTON LS, WEBSTER KE, DEVITT BM, et al. Factors associated with an increased risk of recurrence after a first-time patellar dislocation: a systematic review and Meta-analysis. Am J Sports Med. 2020;48(10):2552-2562. [7] SANDERS TL, PAREEK A, HEWETT TE, et al. High rate of recurrent patellar dislocation in skeletally immature patients: a long-term population-based study. Knee Surg Sports Traumatol Arthrosc. 2018;26(4):1037-1043. [8] GARRON E, JOUVE JL, TARDIEU C, et al. Anatomic study of the anterior patellar groove in the fetal period. Rev Chir Orthop Reparatrice Appar Mot. 2003;89(5):407-412. [9] GLARD Y, JOUVE JL, GARRON E, et al. Anatomic study of femoral patellar groove in fetus. J Pediatr Orthop. 2005;25(3):305-308. [10] ØYE CR, HOLEN KJ, FOSS OA. Mapping of the femoral trochlea in a newborn population: an ultrasonographic study. Acta Radiol. 2015;56(2):234-243. [11] KOHLHOF H, HEIDT C, BÄHLER A, et al. Can 3D ultrasound identify trochlea dysplasia in newborns? Evaluation and applicability of a technique. Eur J Radiol. 2015;84(6):1159-1164. [12] ØYE CR, FOSS OA, HOLEN KJ. Minor change in the sulcus angle during the first six years of life: a prospective study of the femoral trochlea development in dysplastic and normal knees. J Child Orthop. 2018;12(3):245-250. [13] HURI G, ATAY OA, ERGEN B, et al. Development of femoral trochlear groove in growing rabbit after patellar instability. Knee Surg Sports Traumatol Arthrosc. 2012;20(2):232-238. [14] LI W, WANG Q, WANG F, et al. Femoral trochlear dysplasia after patellar dislocation in rabbits. Knee. 2013;20(6):485-489. [15] KAYMAZ B, ATAY OA, ERGEN FB, et al. Development of the femoral trochlear groove in rabbits with patellar malposition. Knee Surg Sports Traumatol Arthrosc. 2013;21(8):1841-1848. [16] YANG G, LI F, LU J, et al. The dysplastic trochlear sulcus due to the insufficient patellar stress in growing rats. BMC Musculoskelet Disord. 2019; 20(1):411. [17] LU J, WANG C, LI F, et al. Changes in Cartilage and Subchondral Bone of Femoral Trochlear Groove After Patellectomy in Growing Rabbits. Orthop Surg. 2020;12(2):653-660. [18] WANG S, JI G, YANG X, et al. Femoral trochlear groove development after patellar subluxation and early reduction in growing rabbits. Knee Surg Sports Traumatol Arthrosc. 2016;24(1):247-253. [19] ØYE CR, FOSS OA, HOLEN KJ. Breech presentation is a risk factor for dysplasia of the femoral trochlea. Acta Orthop. 2016;87(1):17-21. [20] FERLIC PW, RUNER A, DAMMERER D, et al. Patella Height Correlates With Trochlear Dysplasia: A Computed Tomography Image Analysis. Arthroscopy. 2018;34(6):1921-1928. [21] LIEBENSTEINER MC, RESSLER J, SEITLINGER G, et al. High Femoral Anteversion Is Related to Femoral Trochlea Dysplasia. Arthroscopy. 2016; 32(11):2295-2299. [22] 付琨朋.复发性髌骨脱位伴股骨滑车发育不良的儿童患者在手术纠正髌骨位置后滑车形态的变化[D].石家庄:河北医科大学,2018. [23] RAJDEV NR, PARIKH SN. Femoral trochlea does not remodel after patellar stabilization in children older than 10 years of age. J Pediatr Orthop B. 2019; 28(2):139-143. [24] BRATTSTROEM H. Shape of the intercondylar groove normally and in recurrent dislocation of patella. A clinical and x-ray-anatomical investigation. Acta Orthop Scand Suppl. 1964;68:Suppl 68:1-148. [25] DEJOUR H, WALCH G, NEYRET P, et al. Dysplasia of the femoral trochlea. Rev Chir Orthop Reparatrice Appar Mot. 1990;76(1):45-54. [26] KOËTER S, BONGERS EM, DE ROOIJ J, et al. Minimal rotation aberrations cause radiographic misdiagnosis of trochlear dysplasia. Knee Surg Sports Traumatol Arthrosc. 2006;14(8):713-717. [27] SHEN J, QIN L, YAO WW, et al. The significance of magnetic resonance imaging in severe femoral trochlear dysplasia assessment. Exp Ther Med. 2017;14(6):5438-5444. [28] DEJOUR H, WALCH G, NOVE-JOSSERAND L, et al. Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc. 1994;2(1):19-26. [29] TAN SHS, CHNG KSJ, LIM BY, et al. The Difference between Cartilaginous and Bony Sulcus Angles for Patients with or without Patellofemoral Instability: A Systematic Review and Meta-Analysis. J Knee Surg. 2020;33(3):235-241. [30] CARRILLON Y, ABIDI H, DEJOUR D, et al. Patellar instability: assessment on MR images by measuring the lateral trochlear inclination-initial experience. Radiology. 2000;216(2):582-585. [31] PAIVA M, BLØND L, HÖLMICH P, et al. Quality assessment of radiological measurements of trochlear dysplasia; a literature review. Knee Surg Sports Traumatol Arthrosc. 2018;26(3):746-755. [32] DONG Z, NIU Y, DUAN G, et al. Evaluation of Trochlear Dysplasia Severity Using Trochlear Angle: A Retrospective Study Based on Computed Tomography (CT) Scans. Med Sci Monit. 2018;24:5118-5122. [33] RUSH J, DIDUCH D. When is Trochleoplasty a Rational Addition? Sports Med Arthrosc Rev. 2019;27(4):161-168. [34] LIPPACHER S, DEJOUR D, ELSHARKAWI M, et al. Observer agreement on the Dejour trochlear dysplasia classification: a comparison of true lateral radiographs and axial magnetic resonance images. Am J Sports Med. 2012; 40(4):837-843. [35] TSCHOLL PM, WANIVENHAUS F, FUCENTESE SF. Conventional Radiographs and Magnetic Resonance Imaging for the Analysis of Trochlear Dysplasia: The Influence of Selected Levels on Magnetic Resonance Imaging. Am J Sports Med. 2017;45(5):1059-1065. [36] FRITZ B, FUCENTESE SF, ZIMMERMANN SM, et al. 3D-printed anatomic models of the knee for evaluation of patellofemoral dysplasia in comparison to standard radiographs and computed tomography. Eur J Radiol. 2020;127: 109011. [37] SHARMA N, BROWN A, BOURAS T, et al. The Oswestry-Bristol Classification. Bone Joint J. 2020;102-B(1):102-107. [38] NELITZ M, LIPPACHER S. Arthroscopic evaluation of trochlear dysplasia as an aid in decision making for the treatment of patellofemoral instability. Knee Surg Sports Traumatol Arthrosc. 2014;22(11):2788-2794. [39] JAQUITH BP, PARIKH SN. Predictors of Recurrent Patellar Instability in Children and Adolescents After First-time Dislocation. J Pediatr Orthop. 2017;37(7):484-490. [40] LEWALLEN L, MCINTOSH A, DAHM D. First-Time Patellofemoral Dislocation: Risk Factors for Recurrent Instability. J Knee Surg. 2015;28(4):303-309. [41] REZVANIFAR SC, FLESHER BL, JONES KC, et al. Lateral patellar maltracking due to trochlear dysplasia: A computational study. Knee. 2019;26(6):1234-1242. [42] VAN HAVER A, DE ROO K, DE BEULE M, et al. The effect of trochlear dysplasia on patellofemoral biomechanics: a cadaveric study with simulated trochlear deformities. Am J Sports Med. 2015;43(6):1354-1361. [43] 陈思然,安颖颖,展影,等.股骨滑车发育不良致髌股关节软骨损伤T2mapping序列定量评估[J].中华医学杂志,2019,99(21):1651-1655. [44] MOFIDI A, VERAVALLI K, JINNAH RH, et al. Association and impact of patellofemoral dysplasia on patellofemoral arthropathy and arthroplasty. Knee. 2014;21(2):509-513. [45] JUNGMANN PM, THAM SC, LIEBL H, et al. Association of trochlear dysplasia with degenerative abnormalities in the knee: data from the Osteoarthritis Initiative. Skeletal Radiol. 2013;42(10):1383-1392. [46] AKGÜN AS, AGIRMAN M. Associations between Anterior Cruciate Ligament Injuries and Patella Alta and Trochlear Dysplasia in Adults Using Magnetic Resonance Imaging. J Knee Surg. 2020 Mar 4. doi: 10.1055/s-0040-1702198. Online ahead of print. [47] CHEN M, QIN L, LI M, et al. Correlation analysis between femoral trochlear dysplasia and anterior cruciate ligament injury based on CT measurement. Quant Imaging Med Surg. 2020;10(4):847-852. [48] NTAGIOPOULOS PG, DEJOUR D. Current concepts on trochleoplasty procedures for the surgical treatment of trochlear dysplasia. Knee Surg Sports Traumatol Arthrosc. 2014;22(10):2531-2539. [49] CAMATHIAS C, SPETH BM, RUTZ E, et al. Solitary Trochleoplasty for Treatment of Recurrent Patellar Dislocation. JBJS Essent Surg Tech. 2018; 8(2):e11. [50] AMIS AA, OGUZ C, BULL AM, et al. The effect of trochleoplasty on patellar stability and kinematics: a biomechanical study in vitro. J Bone Joint Surg Br. 2008;90(7):864-869. [51] BALCAREK P, ZIMMERMANN F. Deepening trochleoplasty and medial patellofemoral ligament reconstruction normalize patellotrochlear congruence in severe trochlear dysplasia. Bone Joint J. 2019;101-B(3):325-330. [52] CARSTENSEN SE, FEELEY SM, BURRUS MT, et al. Sulcus Deepening Trochleoplasty and Medial Patellofemoral Ligament Reconstruction for Patellofemoral Instability: A 2-Year Study. Arthroscopy. 2020;36(8):2237-2245. [53] BAUDUIN E, PUTMAN S, MIGAUD H, et al. Compared outcomes 16 and 25 years after lateral wedge augmentation trochleoplasty: Rate of recurrent dislocation and progression to osteoarthritis. Orthop Traumatol Surg Res. 2019;105(7):1361-1367. [54] REN B, ZHANG X, ZHANG L, et al. Isolated trochleoplasty for recurrent patellar dislocation has lower outcome and higher residual instability compared with combined MPFL and trochleoplasty: a systematic review. Arch Orthop Trauma Surg. 2019;139(11):1617-1624. [55] BALCAREK P, REHN S, HOWELLS NR, et al. Results of medial patellofemoral ligament reconstruction compared with trochleoplasty plus individual extensor apparatus balancing in patellar instability caused by severe trochlear dysplasia: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2017;25(12):3869-3877. [56] ZAFFAGNINI S, PREVITALI D, TAMBORINI S, et al. Recurrent patellar dislocations: trochleoplasty improves the results of medial patellofemoral ligament surgery only in severe trochlear dysplasia. Knee Surg Sports Traumatol Arthrosc. 2019;27(11):3599-3613. |
| [1] | Pu Rui, Chen Ziyang, Yuan Lingyan. Characteristics and effects of exosomes from different cell sources in cardioprotection [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(在线): 1-. |
| [2] | Min Youjiang, Yao Haihua, Sun Jie, Zhou Xuan, Yu Hang, Sun Qianpu, Hong Ensi. Effect of “three-tong acupuncture” on brain function of patients with spinal cord injury based on magnetic resonance technology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(在线): 1-8. |
| [3] | Xu Feng, Kang Hui, Wei Tanjun, Xi Jintao. Biomechanical analysis of different fixation methods of pedicle screws for thoracolumbar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1313-1317. |
| [4] | Jiang Yong, Luo Yi, Ding Yongli, Zhou Yong, Min Li, Tang Fan, Zhang Wenli, Duan Hong, Tu Chongqi. Von Mises stress on the influence of pelvic stability by precise sacral resection and clinical validation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1318-1323. |
| [5] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [6] | Zhang Yu, Tian Shaoqi, Zeng Guobo, Hu Chuan. Risk factors for myocardial infarction following primary total joint arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1340-1345. |
| [7] | Li Dadi, Zhu Liang, Zheng Li, Zhao Fengchao. Correlation of total knee arthroplasty efficacy with satisfaction and personality characteristics [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1346-1350. |
| [8] | Xiao Guoqing, Liu Xuanze, Yan Yuhao, Zhong Xihong. Influencing factors of knee flexion limitation after total knee arthroplasty with posterior stabilized prostheses [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1362-1367. |
| [9] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [10] | Wang Haiying, Lü Bing, Li Hui, Wang Shunyi. Posterior lumbar interbody fusion for degenerative lumbar spondylolisthesis: prediction of functional prognosis of patients based on spinopelvic parameters [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1393-1397. |
| [11] | Lü Zhen, Bai Jinzhu. A prospective study on the application of staged lumbar motion chain rehabilitation based on McKenzie’s technique after lumbar percutaneous transforaminal endoscopic discectomy [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1398-1403. |
| [12] | Chen Xinmin, Li Wenbiao, Xiong Kaikai, Xiong Xiaoyan, Zheng Liqin, Li Musheng, Zheng Yongze, Lin Ziling. Type A3.3 femoral intertrochanteric fracture with augmented proximal femoral nail anti-rotation in the elderly: finite element analysis of the optimal amount of bone cement [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1404-1409. |
| [13] | Du Xiupeng, Yang Zhaohui. Effect of degree of initial deformity of impacted femoral neck fractures under 65 years of age on femoral neck shortening [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1410-1416. |
| [14] | Liang Yan, Zhao Yongfei, Xu Shuai, Zhu Zhenqi, Wang Kaifeng, Liu Haiying, Mao Keya. Imaging evaluation of short-segment fixation and fusion for degenerative lumbar scoliosis assisted by highly selective nerve root block [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1423-1427. |
| [15] | Yuan Jiawei, Zhang Haitao, Jie Ke, Cao Houran, Zeng Yirong. Underlying targets and mechanism of Taohong Siwu Decoction in prosthetic joint infection on network pharmacology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1428-1433. |
| Viewed | ||||||||||||||||||||||||||||||||||||||||||||||||||
|
Full text 663
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
Abstract 1143
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||