Chinese Journal of Tissue Engineering Research ›› 2021, Vol. 25 ›› Issue (15): 2321-2328.doi: 10.3969/j.issn.2095-4344.3810
Previous Articles Next Articles
Finite element analysis of novel femoral neck system for unstable femoral neck fractures
Fan Zhirong1, Su Haitao2, Zhou Lin1, Huang Huida1, Zhou Junde1, Jiang Tao2, Liu Zitao2
- 1The Second Clinical Medical College, Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China; 2Department of Orthopedics, Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou 510006, Guangdong Province, China
-
Received:2020-06-10Revised:2020-06-16Accepted:2020-07-20Online:2021-05-28Published:2021-01-04 -
Contact:Su Haitao, Professor, Chief physician, Department of Orthopedics, Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou 510006, Guangdong Province, China -
About author:Fan Zhirong, Master candidate, The Second Clinical Medical College, Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China -
Supported by:the Natural Science Foundation of Guangdong Province, No. 2018A030313694 (to JT)
CLC Number:
Cite this article
Fan Zhirong, Su Haitao, Zhou Lin, Huang Huida, Zhou Junde, Jiang Tao, Liu Zitao. Finite element analysis of novel femoral neck system for unstable femoral neck fractures[J]. Chinese Journal of Tissue Engineering Research, 2021, 25(15): 2321-2328.
share this article

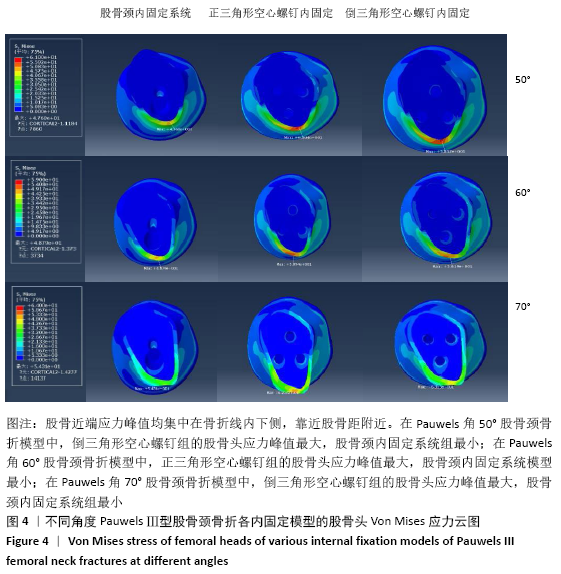
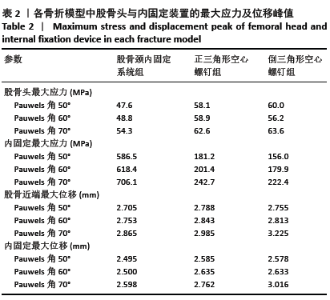
2.1 股骨近端应力分布及峰值 2.1.1 Pauwels角50°股骨颈骨折 3种内固定模型股骨近端应力峰值均集中在骨折线内下侧,靠近股骨距附近。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的股骨近端应力峰值分别为47.6,58.1,60.0 MPa,倒三角形空心螺钉组最大,股骨颈内固定系统组最小,见图4、表2。"
"
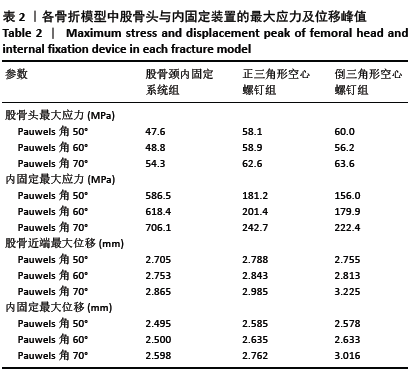
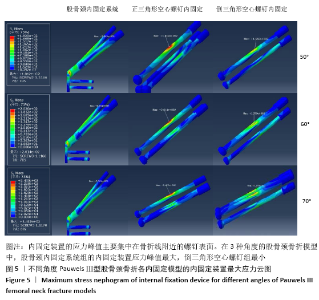
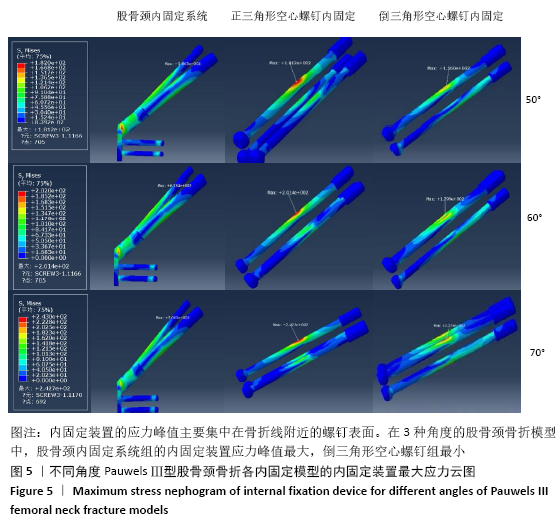
2.1.2 Pauwels角60°股骨颈骨折 3种内固定模型股骨近端应力峰值均集中在骨折线内下侧,靠近股骨距附近。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的股骨近端应力峰值分别为48.8,58.9,56.2 MPa,正三角形空心螺钉组最大,股骨颈内固定系统组最小,见图4、表2。 2.1.3 Pauwels角70°股骨颈骨折 3种内固定模型股骨近端应力峰值均集中在骨折线内下侧,靠近股骨距附近。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的股骨近端应力峰值分别为54.3,62.6,63.6 MPa,倒三角形空心螺钉组最大,股骨颈内固定系统组最小,见图4、表2。 2.2 内固定装置应力分布及峰值 2.2.1 Pauwels角50°股骨颈骨折 3种内固定模型内固定装置的应力峰值主要集中在骨折线附近的螺钉表面。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的内固定装置应力峰值分别为586.5,181.2,156.0 MPa,股骨颈内固定系统组最大,倒三角形空心螺钉组最小,见图5、表2。 2.2.2 Pauwels角60°股骨颈骨折 3种内固定模型内固定装置的应力峰值主要集中在骨折线附近的螺钉表面。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的内固定装置应力峰值分别为618.4,201.4,179.9 MPa,股骨颈内固定系统组最大,倒三角形空心螺钉组最小,见图5、表2。 2.2.3 Pauwels角70°股骨颈骨折 3种内固定模型内固定装置应力峰值主要集中在骨折线附近的螺钉表面。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的内固定装置应力峰值分别为706.1,242.7,222.4 MPa,股骨颈内固定系统组最大,倒三角形空心螺钉组最小,见图5、表2。 在内固定装置中,应力主要集中在骨折线附近的螺钉中间表面。由于结构的特殊性,股骨颈内固定系统的主钉与锁定防旋螺钉使用同一个套筒分出,同时存在一个大小为7.5°的角度,所以当轴向载荷加载时最大应力无可避免地集中在两钉连接处。股骨颈内固定系统组内固定装置的应力峰值高于两空心螺钉组。但是在应力分布云图中可以看出,股骨颈内固定系统模型中的应力分布比其他2个模型更均匀、更分散,见图5。这表明股骨颈内固定系统在股骨近端应力及应力分布传导方面优于正三角形空心螺钉和倒三角形空心螺钉,有利于为骨折愈合创造良好的力学环境。 "

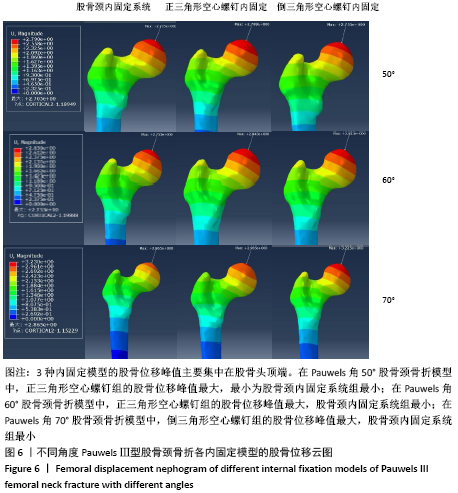
2.3 股骨的位移及峰值 2.3.1 Pauwels角50°股骨颈骨折 3种内固定模型的股骨位移峰值主要集中在股骨头顶端。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的股骨位移峰值分别为2.705,2.788,2.755 mm,正三角形空心螺钉组最大,最小为股骨颈内固定系统组最小,见图6、表2。 2.3.2 Pauwels角60°股骨颈骨折 3种内固定模型的股骨位移峰值主要集中在股骨头顶端。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的股骨位移峰值分别为2.753,2.843,2.813 mm,正三角形空心螺钉组最大,股骨颈内固定系统组最小,见图6、表2。 2.3.3 Pauwels角70°股骨颈骨折 3种内固定模型的股骨位移峰值主要集中在股骨头顶端。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的股骨位移峰值分别为2.753,2.985,3.225 mm,倒三角形空心螺钉组最大,股骨颈内固定系统组最小,见图6、表2。 根据股骨位移分布云图可知,最大位移在均发生在股骨头顶端部,如图6所示。与正三角形空心螺钉和倒三角形空心螺钉相比,不管角度大小,股骨颈内固定系统均具有更小的股骨位移,这表明股骨颈内固定系统具有更小的股骨头移位风险。在Pauwels角50°和60°股骨颈骨折中,倒三角形空心螺钉组的股骨位移小于正三角形空心螺钉组,到Pauwels角度增加到70°时正三角形空心螺钉组的股骨位移小于小于倒三角形空心螺钉组。 "
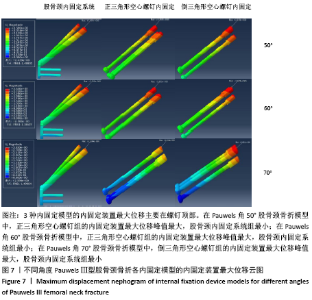
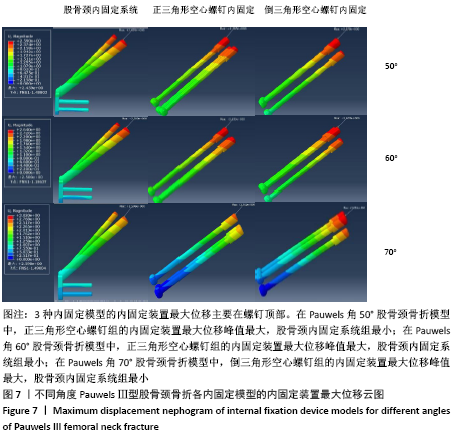
2.4 内固定装置的位移及峰值 2.4.1 Pauwels角50°股骨颈骨折 3种内固定模型的股骨位移峰值主要集中在内固定物上侧顶端。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的内固定装置位移峰值分别为2.495,2.585,2.578 mm,正三角形空心螺钉组最大,股骨颈内固定系统组最小,见图7、表2。 2.4.2 Pauwels角60°股骨颈骨折 3种内固定模型的股骨位移峰值主要集中在内固定物上侧顶端。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的内固定装置位移峰值分别为2.500,2.635,2.633 mm,正三角形空心螺钉组最大,股骨颈内固定系统组最小,见图7、表2。 2.4.3 Pauwels角70°股骨颈骨折 3种内固定模型的股骨位移峰值主要集中在内固定物上侧顶端。股骨颈内固定系统组、正三角形空心螺钉组、倒三角形空心螺钉组的内固定装置位移峰值分别为2.598,2.762,3.016 mm,倒三角形空心螺钉组最大,股骨颈内固定系统组最小,见图7、表2。 3种内固定模型的内固定装置最大位移主要在螺钉顶部。与正三角形空心螺钉和倒三角形空心螺钉相比,股骨颈内固定系统中具有更小的内固定装置位移,这表明股骨颈内固定系统具有更小的内固定移位风险。在Pauwels角 50°和60°股骨颈骨折中,倒三角形空心螺钉组的内固定位移小于正三角形空心螺钉组,当角度增加到70°时正三角形空心螺钉组的内固定位移小于倒三角形空心螺钉组。 "
| [1] JOHNELL O, KANIS JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006; 17(12): 1726-1733. [2] JOHNELL O, KANIS JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int. 2004;15(11):897-902. [3] GULLBERG B, JOHNELL O, KANIS JA. World-wide projections for hip fracture. Osteoporos Int. 1997;7(5):407-413. [4] ABRAHAMSEN B, VAN STAA T, ARIELY R, et al. Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int. 2009; 20(10):1633-1650. [5] MUNDI S, PINDIPROLU B, SIMUNOVIC N, et al. Similar mortality rates in hip fracture patients over the past 31 years. Acta Orthop. 2014; 85(1):54-59. [6] KLOP C, WELSING PM, COOPER C, et al. Mortality in British hip fracture patients, 2000-2010: a population-based retrospective cohort study. Bone. 2014;66:171-177. [7] ROCHE JJ, WENN RT, SAHOTA O, et al. Effect of comorbidities and postoperative complications on mortality after hip fracture in elderly people: prospective observational cohort study. BMJ. 2005;331(7529): 1374. [8] BHANDARI M, DEVEREAUX PJ, SWIONTKOWSKI MF, et al. Internal fixation compared with arthroplasty for displaced fractures of the femoral neck. A meta-analysis. J Bone Joint Surg Am. 2003;85(9):1673-1681. [9] STOEN RO, NORDSLETTEN L, MEYER HE, et al. Hip fracture incidence is decreasing in the high incidence area of Oslo, Norway. Osteoporos Int. 2012;23(10):2527-2534. [10] WANG SH, YANG JJ, SHEN HC, et al. Using a modified Pauwels method to predict the outcome of femoral neck fracture in relatively young patients. Injury. 2015;46(10):1969-1974. [11] BARTONICEK J. Pauwels’ classification of femoral neck fractures: correct interpretation of the original. J Orthop Trauma. 2001;15(5):358-360. [12] LIPORACE F, GAINES R, COLLINGE C, et al. Results of internal fixation of Pauwels type-3 vertical femoral neck fractures. J Bone Joint Surg Am. 2008;90(8):1654-1659. [13] MARSH JL, SLONGO TF, AGEL J, et al. Fracture and dislocation classification compendium - 2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma. 2007;21(10 Suppl):S1-133. [14] KUNAPULI SC, SCHRAMSKI MJ, LEE AS, et al. Biomechanical analysis of augmented plate fixation for the treatment of vertical shear femoral neck fractures. J Orthop Trauma. 2015;29(3):144-150. [15] YANG JJ, LIN LC, CHAO KH, et al. Risk factors for nonunion in patients with intracapsular femoral neck fractures treated with three cannulated screws placed in either a triangle or an inverted triangle configuration. J Bone Joint Surg Am. 2013;95(1):61-69. [16] HUANG HK, SU YP, CHEN CM, et al. Displaced femoral neck fractures in young adults treated with closed reduction and internal fixation. Orthopedics. 2010;33(12):873. [17] HAIDUKEWYCH GJ, ROTHWELL WS, JACOFSKY DJ, et al. Operative treatment of femoral neck fractures in patients between the ages of fifteen and fifty years. J Bone Joint Surg Am. 2004;86(8):1711-1716. [18] Asnis SE, Wanek-Sgaglione L. Intracapsular fractures of the femoral neck. Results of cannulated screw fixation. J Bone Joint Surg Am. 1994;76(12):1793-1803. [19] WANG Z, YIN Y, LI Q, et al. Comparison of early complications between the use of a cannulated screw locking plate and multiple cancellous screws in the treatment of displaced intracapsular hip fractures in young adults: a randomized controlled clinical trial. J Orthop Surg Res. 2018;13(1):201. [20] JOHNSON JP, BORENSTEIN TR, WARYASZ GR, et al. Vertically Oriented Femoral Neck Fractures: A Biomechanical Comparison of 3 Fixation Constructs. J Orthop Trauma. 2017;31(7):363-368. [21] PARKER MJ. Results of internal fixation of Pauwels type-3 vertical femoral neck fractures. J Bone Joint Surg Am. 2009;91(2):490-491. [22] Fixation using Alternative Implants for the Treatment of Hip fractures (FAITH) Investigators. Fracture fixation in the operative management of hip fractures (FAITH): an international, multicentre, randomised controlled trial. Lancet. 2017;389(10078):1519-1527. [23] GOFFIN JM, PANKAJ P, SIMPSON AH. The importance of lag screw position for the stabilization of trochanteric fractures with a sliding hip screw: a subject-specific finite element study. J Orthop Res. 2013; 31(4):596-600. [24] ZHOU L, LIN J, HUANG A, et al. Modified cannulated screw fixation in the treatment of Pauwels type III femoral neck fractures: A biomechanical study. Clin Biomech (Bristol, Avon). 2020;74:103-110. [25] LI J, YIN P, ZHANG L, et al. Medial anatomical buttress plate in treating displaced femoral neck fracture a finite element analysis. Injury. 2019; 50(11):1895-1900. [26] SENSOZ E, OZKAL FM, ACAR V, et al. Finite element analysis of the impact of screw insertion distal to the trochanter minor on the risk of iatrogenic subtrochanteric fracture. Proc Inst Mech Eng H. 2018; 232(8):807-818. [27] ALOLABI B, BAJAMMAL S, SHIRALI J, et al. Treatment of displaced femoral neck fractures in the elderly: a cost-benefit analysis. J Orthop Trauma. 2009;23(6):442-446. [28] DUCKWORTH AD, BENNET SJ, ADERINTO J, et al . Fixation of intracapsular fractures of the femoral neck in young patients: risk factors for failure. J Bone Joint Surg Br. 2011;93(6):811-816. [29] SLOBOGEAN GP, SPRAGUE SA, SCOTT T, et al. Complications following young femoral neck fractures. Injury. 2015;46(3):484-491. [30] SAMSAMI S, SABERI S, SADIGHI S, et al. Comparison of Three Fixation Methods for Femoral Neck Fracture in Young Adults: Experimental and Numerical Investigations. J Med Biol Eng. 2015;35(5):566-579. [31] LI J, ZHAO Z, YIN P, et al. Comparison of three different internal fixation implants in treatment of femoral neck fracture-a finite element analysis. J Orthop Surg Res. 2019;14(1):76. [32] ENOCSON A, LAPIDUS LJ. The vertical hip fracture - a treatment challenge. A cohort study with an up to 9 year follow-up of 137 consecutive hips treated with sliding hip screw and antirotation screw. BMC Musculoskelet Disord. 2012;13:171. [33] KEMKER B, MAGONE K, OWEN J, et al. A sliding hip screw augmented with 2 screws is biomechanically similar to an inverted triad of cannulated screws in repair of a Pauwels type-III fracture. Injury. 2017; 48(8):1743-1748. [34] LI J, WANG M, ZHOU J, et al. Optimum Configuration of Cannulated Compression Screws for the Fixation of Unstable Femoral Neck Fractures: Finite Element Analysis Evaluation. Biomed Res Int. 2018; 2018:1271762. [35] LI J, WANG M, LI L, et al . Finite element analysis of different configurations of fully threaded cannulated screw in the treatment of unstable femoral neck fractures. J Orthop Surg Res. 2018;13(1):272. [36] AMINIAN A, GAO F, FEDORIW WW, et al. Vertically oriented femoral neck fractures: mechanical analysis of four fixation techniques. J Orthop Trauma. 2007;21(8):544-548. [37] BASSO T, KLAKSVIK J, FOSS OA. Locking plates and their effects on healing conditions and stress distribution: A femoral neck fracture study in cadavers. Clin Biomech (Bristol, Avon). 2014;29(5):595-598. [38] TIANYE L, PENG Y, JINGLI X, et al. Finite element analysis of different internal fixation methods for the treatment of Pauwels type III femoral neck fracture. Biomed Pharmacother. 2019;112:108658. [39] YE Y, CHEN K, TIAN K, et al. Medial buttress plate augmentation of cannulated screw fixation in vertically unstable femoral neck fractures: Surgical technique and preliminary results. Injury. 2017;48(10): 2189-2193. [40] WANG G, TANG Y, WU X, et al. Finite element analysis of a new plate for Pauwels type III femoral neck fractures. J Int Med Res. 2020;48(2): 300060520903669. [41] LUTTRELL K, BELTRAN M, COLLINGE CA. Preoperative decision making in the treatment of high-angle “vertical” femoral neck fractures in young adult patients. An expert opinion survey of the Orthopaedic Trauma Association’s (OTA) membership. J Orthop Trauma. 2014;28(9): e221-225. [42] COLLINGE CA, MIR H, REDDIX R. Fracture morphology of high shear angle “vertical” femoral neck fractures in young adult patients. J Orthop Trauma. 2014;28(5):270-275. [43] LI J, WANG M, ZHOU J, et al. Finite element analysis of different screw constructs in the treatment of unstable femoral neck fractures. Injury. 2020;51(4):995-1003. |
| [1] | Xu Feng, Kang Hui, Wei Tanjun, Xi Jintao. Biomechanical analysis of different fixation methods of pedicle screws for thoracolumbar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1313-1317. |
| [2] | Jiang Yong, Luo Yi, Ding Yongli, Zhou Yong, Min Li, Tang Fan, Zhang Wenli, Duan Hong, Tu Chongqi. Von Mises stress on the influence of pelvic stability by precise sacral resection and clinical validation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1318-1323. |
| [3] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [4] | Zhang Yu, Tian Shaoqi, Zeng Guobo, Hu Chuan. Risk factors for myocardial infarction following primary total joint arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1340-1345. |
| [5] | Wei Wei, Li Jian, Huang Linhai, Lan Mindong, Lu Xianwei, Huang Shaodong. Factors affecting fall fear in the first movement of elderly patients after total knee or hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1351-1355. |
| [6] | Wang Jinjun, Deng Zengfa, Liu Kang, He Zhiyong, Yu Xinping, Liang Jianji, Li Chen, Guo Zhouyang. Hemostatic effect and safety of intravenous drip of tranexamic acid combined with topical application of cocktail containing tranexamic acid in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1356-1361. |
| [7] | Xiao Guoqing, Liu Xuanze, Yan Yuhao, Zhong Xihong. Influencing factors of knee flexion limitation after total knee arthroplasty with posterior stabilized prostheses [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1362-1367. |
| [8] | Huang Zexiao, Yang Mei, Lin Shiwei, He Heyu. Correlation between the level of serum n-3 polyunsaturated fatty acids and quadriceps weakness in the early stage after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1375-1380. |
| [9] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [10] | Wang Haiying, Lü Bing, Li Hui, Wang Shunyi. Posterior lumbar interbody fusion for degenerative lumbar spondylolisthesis: prediction of functional prognosis of patients based on spinopelvic parameters [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1393-1397. |
| [11] | Lü Zhen, Bai Jinzhu. A prospective study on the application of staged lumbar motion chain rehabilitation based on McKenzie’s technique after lumbar percutaneous transforaminal endoscopic discectomy [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1398-1403. |
| [12] | Chen Xinmin, Li Wenbiao, Xiong Kaikai, Xiong Xiaoyan, Zheng Liqin, Li Musheng, Zheng Yongze, Lin Ziling. Type A3.3 femoral intertrochanteric fracture with augmented proximal femoral nail anti-rotation in the elderly: finite element analysis of the optimal amount of bone cement [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1404-1409. |
| [13] | Du Xiupeng, Yang Zhaohui. Effect of degree of initial deformity of impacted femoral neck fractures under 65 years of age on femoral neck shortening [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1410-1416. |
| [14] | Zhang Shangpu, Ju Xiaodong, Song Hengyi, Dong Zhi, Wang Chen, Sun Guodong. Arthroscopic suture bridge technique with suture anchor in the treatment of acromioclavicular dislocation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1417-1422. |
| [15] | Liang Yan, Zhao Yongfei, Xu Shuai, Zhu Zhenqi, Wang Kaifeng, Liu Haiying, Mao Keya. Imaging evaluation of short-segment fixation and fusion for degenerative lumbar scoliosis assisted by highly selective nerve root block [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1423-1427. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||