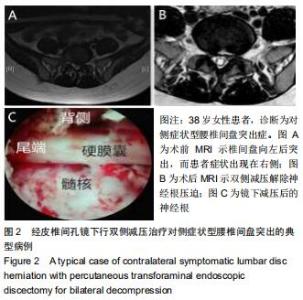
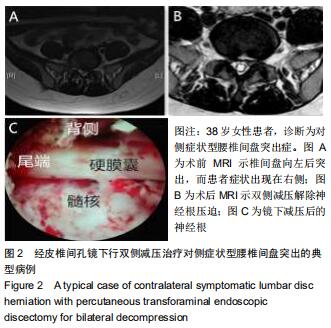
|
[1] MACNAB I. Negative disc exploration:an analysis of the causes of nerveroot involvement in sixty-eight patients.J Bone Joint Surg Am.1971;53(7):891-893.
[2] 李瑞,孙兆忠,房清敏,等.椎间孔镜TESSYS技术上关节突磨削程度对腰椎稳定性的影响[J].中国矫形外科杂志,2018,26(10): 898-903.
[3] KALEMCI O, KIZMAZOGLU C, OZER E, et al. Lumbar disc herniation associated with contralateral neurological deficit: can venous congestion be the cause? Asian Spine J.2013; 7(1):60-62.
[4] NAYLOR A, HAPPEY F, TURNER RL, et al. Enzymic and immunological activity in the intervertebral disk.Orthop Clin North Am. 1975;6(1):51-58.
[5] 王建忠,周跃,梅芳瑞.腰椎间盘突出物中白细胞介素-1含量与根性痛的相关性[J].现代康复,2001,5(2):39.
[6] 胡旭民,蔡兆鹏,黄霖,等.经皮椎间孔镜下髓核摘除联合侧隐窝减压治疗对侧症状腰椎间盘突出症[J].中国骨与关节损伤杂志,2016, 31(5):527-529.
[7] 侯树勋,吴闻文,刘汝落,等.髓核突出类型与腰腿痛严重程度的关系(附300例分析)[J].解放军医学杂志,1993,18(5):349-351.
[8] KORNBERG M. Sciatica contralateral to lumbar disk herniation. Orthopedics.1994;17(4):362-364.
[9] CHOUDHURY AR, TAYLOR JC, WORTHINGTON BS, et al. Lumbar radiculopathy contralateral to upper lumbar disc herniation:report of 3 cases. Br J Surg.1978;65(12):842-844.
[10] 孙根文,塔依尔•阿不都哈德尔.经皮椎间孔镜技术治疗腰椎病变的研究进展[J].中国矫形外科杂志,2014,22(5):422-425.
[11] KIM P, JU CI, KIM HS, et al. Lumbar Disc Herniation Presented with Contralateral Symptoms.J Korean Neurosurg Soc. 2017; 60(2):220-224.
[12] SUCU HK, GELAL F.Lumbar disc herniation with contralateral symptoms.Eur Spine J.2006;15:570-574
[13] 张艳玲,韩小博.单侧腰椎间盘突出致对侧症状的诊疗创新思路[J].中国骨与关节损伤杂志,2014,30(3):278-279.
[14] 马维平,朱兵,王文,等.经皮椎间孔镜治疗对侧症状腰椎间盘突出症的入路分析[J].中国医刊,2018,53(1):51-53.
[15] ASAN Z. Lumbar Disc Herniations Causing Contralateral Radicular Symptoms: Can They Be Explained by a Hypotenusal Theory? World Neurosurgery.2018;114(15): 1297-1301.
[16] AKDENIZ T, KANER T, TUTKAN I, et al. Unilateral surgical approach for lumbar disc herniation with contralateral symptoms. J Neurosurg Spine.2012;17:124-127.
[17] YANG JS, ZHANG DJ, HAO DJ. Lumbar disc herniation with contralateral radiculopathy: do we neglect the epidural fat?Pain Physician. 2015;18(2):E253-256.
[18] NAKAGAWA Y, YOSHIDA M, KAWAKAMI M, et al. Posterior Endoscopic Surgery for Lumbar Disc Herniation with Contralateral Symptoms-A Report of Two Cases. Minim Invasive Neurosurg. 2006;49(5):282-285.
[19] KIM P, JU CL, KIM HS, et al. Lumbar Disc Herniation Presented with Contralateral Symptoms. J Korean Neurosurg Soc.2017; 60(2):220-224.
|