Chinese Journal of Tissue Engineering Research ›› 2013, Vol. 17 ›› Issue (35): 6321-6326.doi: 10.3969/j.issn.2095-4344.2013.35.016
Previous Articles Next Articles
Clinical application of artificial lumbar disc replacement: Present and future
Bai Wen-yuan1, 2, Gu Hong-sheng3, Liao Zhen-hua2, Liu Wei-qiang1, 2
- 1Graduate School of Shenzhen, Tsinghua University, Shenzhen 518055, Guangdong Province, China; 2Research Institute of Tsinghua University in Shenzhen, Shenzhen 518057, Guangdong Province, China; 3Shenzhen Second People’s Hospital, Shenzhen 518049, Guangdong Province, China
-
Received:2013-04-12Revised:2013-05-29Online:2013-08-27Published:2013-08-27 -
Contact:Liu Wei-qiang, Professor, Graduate School of Shenzhen, Tsinghua University, Shenzhen 518055, Guangdong Province, China; Research Institute of Tsinghua University in Shenzhen, Shenzhen 518057, Guangdong Province, China weiqliu@hotmail.com -
About author:Bai Wen-yuan★, Studying for master’s degree, Graduate School of Shenzhen, Tsinghua University, Shenzhen 518055, Guangdong Province, China; Research Institute of Tsinghua University in Shenzhen, Shenzhen 518057, Guangdong Province, China 83827418@qq.com -
Supported by:National Science and Technology Planning Project, No.2012BAI18B05*; Shenzhen Key Laboratory Upgrading Project, No. ZDSY20120616140540279*
CLC Number:
Cite this article
Bai Wen-yuan, Gu Hong-sheng, Liao Zhen-hua, Liu Wei-qiang. Clinical application of artificial lumbar disc replacement: Present and future[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(35): 6321-6326.
share this article
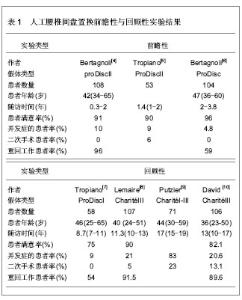
2.1 纳入研究基本概况 文章纳入的34篇文献中,属于大宗实验报道的有3个前瞻性实验[4-7]、4个回顾性实验[8-10]、以及权威部门批准的器械豁免实验[11-16],文献[17-34]旨在探索影响人工腰椎间盘置换临床结果的因素,所以一同纳入本文,用来研究腰椎间盘置换术的临床应用现状。 表1列出了大宗的人工腰椎间盘置换前瞻性和回顾性实验结果,可知中、短期随访结果明显优于远期随访的结果。值得关注的是,在17年回顾性实验结果中[9],最好的临床结果是患者发生自发性骨强直,而且相邻节段发生退变率高达17%,该临床实验结果与腰椎间盘置换防止相邻节段椎间盘退变的理念不符。"


表2列出了权威部门批准的器械豁免实验(Instrumental Device Exemption,IDE)的结果,包括由美国FDA批准的多中心ProDisc Ⅱ的器械豁免实验2年随访结果、Charité Ⅲ 的器械豁免实验2年和5年随访结果、瑞典罗林斯卡医学院伦理委员会批准的3种腰椎间盘假体(Charité Ⅲ、ProDisc Ⅱ、Maverick)的2年随访结果。在这些实验中,实验组(人工腰椎间盘置换)与对照组(腰椎融合术)都得到了较好的临床效果,实验组的失血量、手术时间、住院时间、患者满意率、并发症发生率、目测类比评分和ODI改善情况等都得到了较满意的效果。"
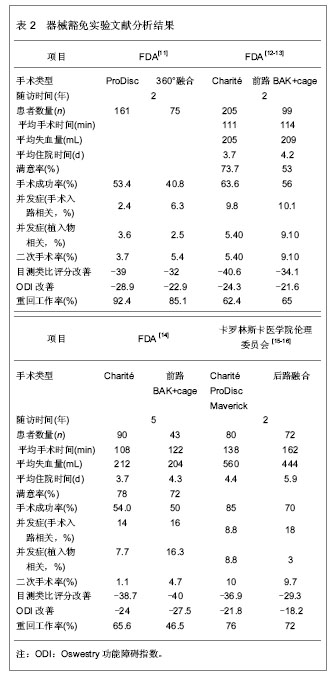

Charité假体器械豁免实验2年随访结果显示,置换组在患者满意率、目测类比评分和ODI评分明显优于融合组,然而其5年随访结果却与融合组没有统计学差异,患者满意率也与融合组接近。有人担心,因为在该FDA控制的实验中施行手术的都是最优秀的脊柱外科医生,患者的适应证选择非常严格,在随访时间较短的情况下容易得到满意的疗效。假体投放市场后,术后长期疗效可能降低,并发症增多。虽然Blumenthal等[12]报道了Charité假体进入市场1年后进行的4 000余例手术,并发症的发生率与器械豁免实验结果相似[17],作者认为,腰椎间盘假体置换术后的短、中期随访结果是否能与融合术相媲美,远期随访结果是否能防止小关节和相邻节段退变,还需要大量前瞻性、大宗样本、长期随访的资料来证实。 2.2 腰椎间盘置换术的临床应用现状 2.2.1 人工腰椎间盘置换的适应证和禁忌证 美国骨科医师协会制定的人工腰椎间盘置换适应证为有症状的椎间盘破裂、退变,脊柱融合所致相邻节段退变不稳。禁忌证为手术节段脊柱畸形、严重骨质疏松、Ⅱ级以上腰椎滑脱、骨性椎管狭窄、手术瘢痕粘连引起的腰痛。通过分析大量的临床实验结果,作者认为对于腰椎间盘适应证和禁忌证的选择,还应考虑如下内容:手术节段数对临床结果的影响:在许多临床实验报道中,单节段、双节段腰椎间盘退行性疾病都是腰椎间盘置换的理想适应证[5,7,15,18]。但Siepe等[19]进行ProDisc Ⅱ假体单、双节段置换实验中,双节段置换组患者有更多的并发症,患者满意度也较差。虽然FDA只批准了Charité Ⅲ在单节段置换术中的应用,然而对于ProDisc Ⅱ假体允许进行双节段置换术。而3节段腰椎间盘病变则很少采用单独的腰椎间盘置换治疗,可进行置换术与融合术的联合应用。 小关节退变对临床结果的影响:椎间盘退变但没有继发小关节改变和腰椎不稳是现阶段临床实验中普遍认可的适应证,严格排除了小关节病变的临床实验也得到了很好的疗效[4,6,11-12]。而实际上,许多实验仅将有明显的小关节退变(Ⅲ-Ⅳ度)列为腰椎间盘置换术的禁忌证,即纳入轻症的小关节退变患者,相应随访结果中出现了较多的并发症[8-10]。因此作者认为,术前严格排除小关节退变,是人工腰椎间盘置换取得良好疗效的保障。 既往有腰椎间盘手术史患者的选择:许多临床实验中对腰椎融合后有相邻节段椎间盘退变的患者和腰椎间盘切除后复发的患者行腰椎间盘置换[6,20-21],均得到了较好的临床效果,与首次行腰椎间盘置换患者临床结果上没有显著差异。然而,其他临床实验中却得到了不同的结论。Lemaire等[8]发现经历过多次腰椎间盘手术的患者,Charité假体置换术后有较多的并发症,Blondel等[22]也发现既往有后路腰椎间盘切除术的患者术后临床效果较差。实际上既往有前路腰椎手术的患者,由于瘢痕组织的影响,极易发生术中并发症,所以不适合再进行前路的腰椎间盘置换手术。只要手术前仔细排除禁忌证,其他情况下的腰椎手术史则对置换术的疗效没有显著影响。 患者年龄:一直以来,许多学者认为腰椎间盘置换仅适合18-45岁的患者。Sott等[23]在一次评估Charité假体置换结果中发现,大于45岁的患者在临床结果上没有明显差异。Bertagnoli等[18]对大于60岁患者进行腰椎间盘置换得到了较好的临床结果。尽管如此,在60岁以上患者的置换患者选择上要十分慎重,确定患者的骨质良好并没有中央型椎管狭窄。 椎间盘置换前休息时间:Rohan等[24]对232例行Charité、ProDisc假体置换或融合手术的患者进行了统计,得到了一个有趣的结论:椎间盘置换前离开工作时间为0-13周的患者比大于13周的患者在术后有更好的目测类比评分和ODI改善。这一研究结论提示,椎间盘置换前适当的工作一段时间对术后的临床结果有促进作用。这种现象的原因可能是患者的心理因素对手术疗效有一定影响。 在判断患者是否适合进行腰椎间盘置换手术前,需要对腰椎间盘退变进行分级,详细询问病史、体格检查、影像学检查、诊断性注射药物和椎间盘造影。术后患者疼痛缓解的程度、假体的结构设计以及材料的缺陷、患者的心理因素等都可能影响手术结果。腰椎间盘置换在扩大的适应证中可应用于多个节段、有轻微的小关节退化、既往有后路椎间盘切除手术史,已融合部位的邻近节段,45岁以上无骨质疏松的患者,但也应注意这些情况也有降低术后临床效果的风险。 2.2.2 人工腰椎间盘置换围手术期经济学考量 评价腰椎间盘置换是否优于传统的腰椎融合,还可以从术中出血量、手术时间、术后住院时间等方面进行考量,这对于评价腰椎手术的安全性以及患者、医院在腰椎手术期间的经济性等都有重要意义。 Zigler等[11]和Sasso等[24]分别报道了在手术时间和出血量这两个指标上,腰椎间盘置换组都明显优于360°腰椎融合组。然而,与腰椎前路融合或后路融合术相比,有报道显示腰椎间盘置换术在手术时间和出血量上没有显著差别[12]。在评价患者术后住院时间这一指标时,临床报道结果较一致,腰椎间盘置换术较传统融合术具有更短的住院时间[11,27],FDA对Charité假体的器械豁免实验结果显示,Charité置换组在两个主要经济方面显示出明显优势,并有统计学意义:住院时间减少1 d,再手术率更低(5.4% vs. 9.1%)[12]。Guyer等[14]从患者和医院两个角度比较了一节段Charité腰椎间盘置换和腰椎融合在术中和术后两年内医院和患者的经济费用比较,腰椎间盘置换术较传统融合术更加经济。 虽然在手术技术上腰椎间盘置换术更复杂,但是临床实验结果并没有显示其在手术中更大的出血量、更长的手术时间,所以腰椎间盘置换术在术中的经济性和安全性方面值得肯定。另外,值得考虑的是与脊柱融合术相比,人工腰椎间盘置换潜在优点之一是患者可以尽快参加康复训练。从现有的结果来看,腰椎间盘置换术与融合术相比,没有增加患者和医院双方的经济负担,但是对于全腰椎间盘置换手术的脊柱外科医生的训练、置换术后翻修手术的花费等还需更多的临床数据加以补充,才能确定其经济性是否与传统融合手术相仿。 2.2.3 远期并发症 临床实验中腰椎间盘置换后短、中期疗效值得肯定,但是远期疗效尚有很多不尽如意的地方。腰椎间盘置换后较常见的并发症有异位骨化、植入物机械故障、相邻节段和小关节退变,下面分别进行介绍。 异位骨化:腰椎间盘置换术后异位骨化导致手术节段的椎间隙自动融合,文献报道异位骨化的发生率为0.5%-15.2%。尽管人工腰椎间盘置换后异位骨化与其保留节段运动功能的初衷相悖,但大部分的异位骨化不影响疗效,只影响腰椎的活动度。通常,McAfee[27]定义的Ⅲ级以上的异位骨化腰椎活动度有所降低,但不影响患者的目测类比评分和ODI评分,也不影响临床疗效[28]。 植入物机械故障:包括植入物磨损、移位、脱位、沉降等。Punt等[29]总结了1 000例Charité腰椎间盘置换术后10年随访资料,进行再手术的患者中76%是由植入物机械故障引起的,所以这类并发症受到越来越多的重视。随着脊柱外科医师行腰椎间盘置换术的熟练性增强、假体更大的终板面和即刻固定装置的发展,假体的移位、脱位、沉降等并发症已经明显减少。 相邻节段和小关节退变:Trouillier等[30]用计算机断层扫描吸收法测定人工腰椎间盘置换术后对相邻节段和小关节的应力变化,结果显示相邻节段所受应力没有增加,在手术节段小关节所受应力明显减小。然而,在临床实验中相邻节段和小关节退变的发生率随着随访时间的增加而不断上升,一般在术后两年内较少发现相邻节段和小关节退变,而长期随访结果不容乐观。Tierry David等[10]在10年以上的随访中,发现有5%的患者发生了小关节退化,3%患者出现相邻节段病变。Putzier等[9]进行的17年随访中,有17%的患者出现了明显的相邻节段退变,这个结论与融合术后长达30年随访中相邻节段退变的发生率(14.2%)相近。Siepe等[31]也在置换术后发现20%患者出现小关节退变现象,尤以L5-S1节段为多。所以,腰椎间盘置换术对小关节和相邻节段的应力影响还需要进一步临床实验和观察。 2.2.4 人工腰椎间盘置换与融合术的混合使用 由于采取人工腰椎间盘置换对腰椎融合后相邻节段退变的患者进行治疗得到较好的疗效[6,20],有学者提出,可以灵活运用融合和置换手术,将两种手术同时用于治疗多节段腰椎间盘病变,使两种手术干预方法互补不足,得到优于单独使用的手术疗效。Grauer等[32]通过有限元方法分别在L4-S1节段进行双节段置换和混合手术,发现对于L3-L4节段,双节段置换组中运动度减小,在混合组中运动度增大。Qingan等[33]对尸体标本施行胸腰长脊柱融合术后,L4-L5和L5-S1节段活动度明显增大,在脊柱融合的尾端相邻节段施行Maverick假体单、双节段置换术后,这两个节段的活动度趋于正常。Cunningham等[34]发现Charité双节段置换组在屈伸运动时相邻节段的椎间盘内压力明显增大,而Charité与椎弓根螺钉混合手术组相邻节段的运动更接近正常生理状态。显然,腰椎融合术后相邻节段运动范围变大会对椎间盘和小关节产生一定的损伤,而混合手术则较好的矫正了这种现象。 如今在同一次手术中不同节段行混合手术还少有报道,混合手术可用于多节段腰椎间盘退变,其中某些节段适合行腰椎间盘置换,而其他节段则不适合行腰椎间盘置换的情况(如该节段有骨赘、小关节已有病变、椎间隙过小不适合假体置换等)。施行混合手术的适应证、禁忌证、术后的康复训练、评价方式、翻修手术方法等问题还需更多的体外辅助实验和临床实验进行探索。"

| [1] Blondel B, Tropiano P, Gaudart J, et al.Clinical Results of Total Lumbar Disc Replacement Regarding Various Aetiologies of the Disc Degeneration: A Study With a 2-Year Minimal Follow-up. Spine.2011;36(5): E313-E319. [2] Van Steen brugghe MH.Improvements in joint prosthesis. French Patent. 1956:122-128. [3] Fernstrom U. Arthroplasty with intercorporal endoprothesis in herniated disc and in painful disc. Acta Chir Scand.1966; 357:154-159. [4] Bertagnoli R, Kumar S. Indications for full prosthetic disc arthroplasty: a correlation of clinical outcome against a variety of indications. Eur spine J.2002;11(2): S131-S136. [5] Tropiano P, Huang RC, Girardi FP, et al. Lumbar disc replacement: Preliminary results with ProDisc II after a minimum follow-up period of one year. J Spinal Disord Tech. 2003;16(4):362-368. [6] Tropiano P, Huang RC, Girardi FP, et al. Lumbar total disc replacement.Seven to eleven-year follow-up. J Bone Joint Surg Am. 2005;87(3):490-496. [7] Bertagnoli R, Yue JJ, Shah RV, et al. The treatment of disabling single-level lumbar discogenic low back pain with total disc arthroplasty utilizing the Prodisc prosthesis: a prospective study with 2-year minimum follow-up. Spine.2005; 30(19): 2230-2236. [8] Lemaire J, Ali ES, Skalli W. Clinical and Radiological Outcomes With the Charite Artificial Disc. 2005;18(4): 353-359. [9] Putzier M,Funk JF,Schneider SV, et al. Charité total disc replacement--clinical and radiographical results after an average follow-up of 17 years. Eur Spine J.2006;15(2): 183-195. [10] Thierry David MD. Long-term Results of One-Level Lumbar Arthroplasty: Minimum 10-Year Follow-up of the CHARITE Artificial Disc in 106 Patients. Spine.2007; 32(6):661-666. [11] Zigler J, Delamarter R, Spivak JM, et al. Results of the prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of the ProDisc-L total disc replacement versus circumferential fusion for the treatment of 1-level degenerative disc disease. Spine. 2007; 32(11):1155-1162. [12] Blumenthal S, McAfee PC, Guyer RD, et al. A prospective, randomized, multicenter Food and Drug Administration investigational device exemptions study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part I: evaluation of clinical outcomes. Spine.2005; 30(14):1565-1575. [13] McAfee PC,Cunningham B,Holsapple G,et al.A prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part II: evaluation of radiographic outcomes and correlation. Spine.2005;30(14):1576-1583. [14] Guyer RD, McAfee PC, Banco RJ, et al. Prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: five-year follow-up. Spine J.2009;9(5): 374-386. [15] Berg S, Tropp HT, Leivseth G. Disc height and motion patterns in the lumbar spine in patients operated with total disc replacement or fusion for discogenic back pain. Results from a randomized controlled trial. Spine J.2011; 11(11): 991-998. [16] Berg S, Tullberg T, Branth B, et al. Total disc replacement compared to lumbar fusion: a randomized controlled trial with 2-year follow-up. Eur Spine J. 2009;18:1512-1519. [17] 詹姆斯.J.Y..脊柱功能重建外科学:高级理论和技巧[M].邹德威,译. 北京:人民军医出版社,2008. [18] Bertagnoli R, Yue JJ. Lumbar total disc arthroplasty in patients older than 60 years of age: a prospective study of the ProDisc prosthesis with 2-year minimum follow-up period. J Neurosurg Spine.2006;4(2):85-90. [19] Siepe CJ, Mayer HM, Wiechert K, et al. Clinical results of total lumbar disc replacement with ProDisc II: three-year results for different indications. Spine.2006;31(17):1923-1932. [20] Bertagnoli R,YueJJ,Fenk-Mayer A,et al.Treatment of symptomatic adjacent-segment degeneration after lumbar fusion with total disc arthroplasty by using the prodisc prosthesis: a prospective study with 2-year minimum follow up. J Neurosurg Spine.2006;4(2):91-97. [21] Glenn JS,Yaker J,Guyer RD, et al. Anterior discectomy and total disc replacement for three patients with multiple recurrent lumbar disc herniations. Spine J.2011;11(9): e1-e6. [22] Blondel B, Tropiano P, Gaudart J, et al.Clinical Results of Total Lumbar Disc Replacement Regarding Various Aetiologies of the Disc Degeneration: A Study With a 2-Year Minimal Follow-up. Spine.2011;36(5): E313-E319. [23] Sott AH , Harrison DJ. Increasing age does not affect good outcome after lumbar disc replacement. International orthopaedics.2000;24(1):50-53. [24] Rohan MX, Ohnmeiss DD, Guyer RD, et al. Relationship between the length of time off work preoperatively and clinical outcome at 24-month follow-up in patients undergoing total disc replacement or fusion. Spine J.2009; 9(5):360-365. [25] Sasso RC, Foulk DM,Hahn M,et al.Prospective, randomized trial of metal-on-metal artificial lumbar disc replacement: initial results for treatment of discogenic pain. Spine.2008;33(2):123-131. [26] Richard D, Guyer SG, Tromanhauser, et al. An economic model of one-level lumbar arthroplasty versus fusion. Spine J.2007;7(5):558-562. [27] McAfee PC,Cunningham BW,Devine J,et al.Classification of heterotopic ossification(HO) in artificial disc replacement. J Spine Disord Tech.2003; 16(4):384-389. [28] Park SJ, Kang KJ, Shin SK, et al. Heterotopic ossification following lumbar total disc replacement. Int Orthop.2011;35(8): 197-201. [29] Punt IM, Visser VM, van Rhijn LW, et al. Complications and reoperations of the SB Charité lumbar disc prosthesis: experience in 75 patients. Eur Spine J.2008;17(1):36-43. [30] Trouillier H, Kern P, Refior HJ, et al. A prospective morphological study of facet joint integrity following intervertebral disc replacement with the charite artificial disc. Eur Spine J.2006;15(2):174-182. [31] Siepe CJ, Zelenkov P, Sauri-Barraza JC, et al. The fate of facet joint and adjacent level disc degeneration following total lumbar disc replacement: A prospective clinical, X-ray, and magnetic resonance imaging investigation. Spine.2010; 35(22): 1991-2003. [32] Grauer JN,Biyani A, Faizan A,et al.Biomechanics of two-level Charité artificial disc placement in comparison to fusion plus single-level disc placement combination. Spine J.2006;6(6): 659-666. [33] Qingan Z, Timothy S, Eyal I, et al. Kinematic evaluation of one- and two-level Maverick lumbar total disc replacement caudal to a long thoracolumabar spinal fusion. Eur Spine J.2012;21(5):S599-611. [34] Cunningham BW, Nianbin H, Hassan S, et al. Revision strategies for single- and two-level total disc arthroplasty procedures: a biomechanical perspective. Spine J.2009;9(9): 735-743. |
| [1] | Shi Bin, An Jing, Chen Long-gang, Zhang Nan, Tian Ye . Influencing factors for pain after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 993-997. |
| [2] | Lu Yao-jia, Xiong Chuan-zhi, Li Xiao-lei, Hu Han-sheng, Chen Gang, Wang Qiang, Lu Zhi-hua. Comparison of two methods for reducing blood loss during total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(7): 1004-1008. |
| [3] | Hu Jun, Zhang De-qiang, Tang Xin. Postoperative quality of life of internal fixation versus hemiarthroplasty for femoral neck fractures in the elderly [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(19): 2953-2960. |
| [4] | Sun Hao, Wei Jun-qiang, Liu Li-rui, Yan Shi, Jin Yu, Feng Zhen. Time of lower extremity deep venous thrombosis after hip arthroplasty in senile patients with osteoporotic femoral neck fractures [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(19): 2961-2965. |
| [5] |
Gao Wei-lu, Li Hong, Liu Bi-quan, Hu Yong, Liu Jing-jun, Yin Li, Liu Hu, Mei Bin, Yin Zong-sheng.
Analgesic effect of femoral and sciatic nerve block under multimodal analgesia in total knee arthroplasty
|
| [6] | Bai Zhao-hui, Zhang Ying, Yin Qing-shui, Xia Hong, Wang Jian-hua, Xu Jun-jie. Navigational template applied in the orthopaedic field in China: a bibliometric analysis [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(19): 3023-3030. |
| [7] | Chen De-long, Chen Peng, Zhou Chi, Huo Shao-chuan, Liu Yong, Wang Hai-bin, He Wei. Risk factors for hidden blood loss after total hip arthroplasty in patients with ankylosing spondylitis [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(11): 1669-1674. |
| [8] | Qin Di, Han Yong-tai, Li Hui-jie. Effect of periprosthetic fracture on hip function after femoral neck-preserving total hip arthroplasty: study protocol for a prospective, single-center, self-controlled trial with 2-year follow-up [J]. Chinese Journal of Tissue Engineering Research, 2016, 20(53): 7985-7991. |
| [9] | Qiu Xiao-ming, Zhen Ping, Li Guang-yong. Effects of different wear particles on multiple systems after artificial joint replacement [J]. Chinese Journal of Tissue Engineering Research, 2016, 20(53): 8051-8056. |
| [10] | Zhang Yang-chun, Xiao Jian-hong, Zhang Zi-ji, Yang Xing, Yu Shi-ming, Sheng Pu-yi . Vacuum sealing drainage combined with iodophor douche for the prosthesis infection after artificial joint replacement [J]. Chinese Journal of Tissue Engineering Research, 2016, 20(44): 6549-6556. |
| [11] | Xu Jie, Li Deng, Zhang Ying-bin, Huang Yu-lin, Cai Zhi-qing, Ma Ruo-fan. Accuracy of analog two-dimensional and digital three-dimensional preoperative templating for predicting implant size in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2016, 20(35): 5173-5179. |
| [12] | Gao Ji-hai, Wang Jiang-quan, Lv Dong-wei . Influencing factors of knee function in osteoarthritis patients after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2016, 20(31): 4582-4588. |
| [13] | Jiang Yuan-tao, Jiao Jian-bao, Xue Jin-wei, Wang Yun-fei . Biomechanical characteristics of bipolar femoral head prosthesis replacement and internal fixation for femoral neck fractures in the elderly [J]. Chinese Journal of Tissue Engineering Research, 2016, 20(26): 3805-3810. |
| [14] | Tang Zhi, Gui Bin-jie, Ding Nan, Rong Gen-xiang, Gao Jie, Wang Si-sheng. Changes of acetabular angle at different positions after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2016, 20(26): 3817-3822. |
| [15] | Sun Xiao-liang, Wu Liang, Wu Guo-feng, Zhou Jian, Wang Kun, Zhang Jian-wei, Zhou Li-ping,Gong Zong-ming, Tang Zhen-yu. Adult bilateral Crowe type-IV developmental dysplasia of the hip: is the prosthesis an optimal therapeutic strategy? [J]. Chinese Journal of Tissue Engineering Research, 2014, 18(40): 6408-6412. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||