Chinese Journal of Tissue Engineering Research ›› 2026, Vol. 30 ›› Issue (17): 4457-4471.doi: 10.12307/2026.084
Previous Articles Next Articles
Effects of central and peripheral rehabilitation therapies on upper extremity function and activities of daily living in stroke patients: a network meta-analysis
Chen Jinhui1, Yu Zifu2, Gao Shiai1, Cao Xinyan1, Leng Xiaoxuan1, Liu Xihua3
- 1School of Rehabilitation Medicine, Shandong University of Traditional Chinese Medicine, Jinan 250355, Shandong Province, China; 2Shandong Provincial Center for Disease Control and Prevention, Jinan 250014, Shandong Province, China; 3Department of Rehabilitation, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan 250014, Shandong Province, China
-
Received:2025-02-26Accepted:2025-05-19Online:2026-06-18Published:2025-12-03 -
Contact:Liu Xihua, MD, Chief physician, Master’s supervisor, Department of Rehabilitation, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan 250014, Shandong Province, China -
About author:Chen Jinhui, MS candidate, School of Rehabilitation Medicine, Shandong University of Traditional Chinese Medicine, Jinan 250355, Shandong Province, China -
Supported by:National Natural Science Foundation of China, No. 81802239 (to LXH); Shandong Province Traditional Chinese Medicine Science and Technology Project, No. M-2023142 (to LXH); Shandong Province Medical Workers Science and Technology Innovation Program, No. SDYWZGKCJH2022024 (to LXH)
CLC Number:
Cite this article
Chen Jinhui, Yu Zifu, Gao Shiai, Cao Xinyan, Leng Xiaoxuan, Liu Xihua. Effects of central and peripheral rehabilitation therapies on upper extremity function and activities of daily living in stroke patients: a network meta-analysis[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(17): 4457-4471.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
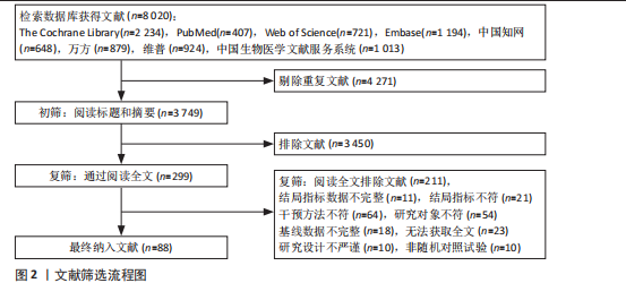
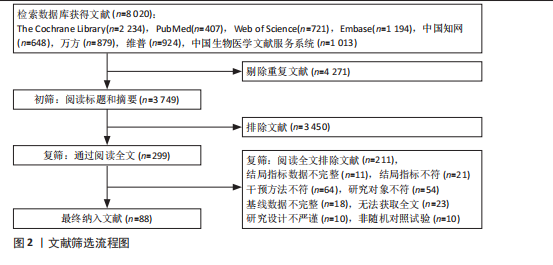
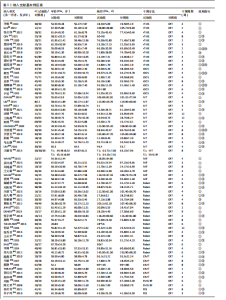
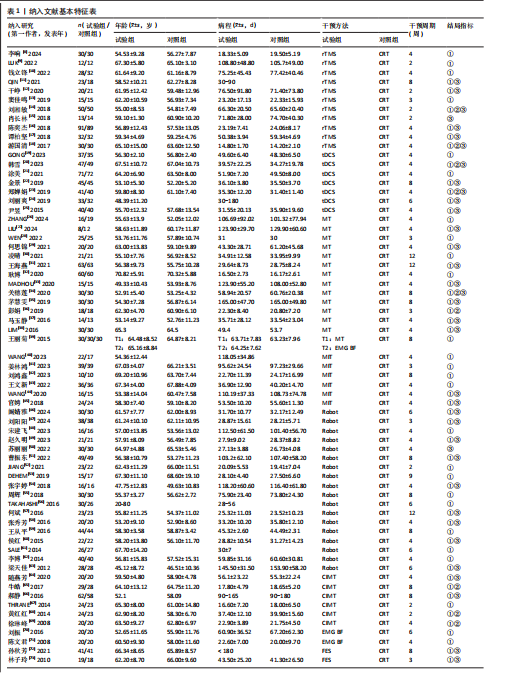
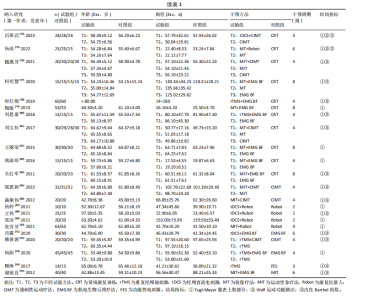
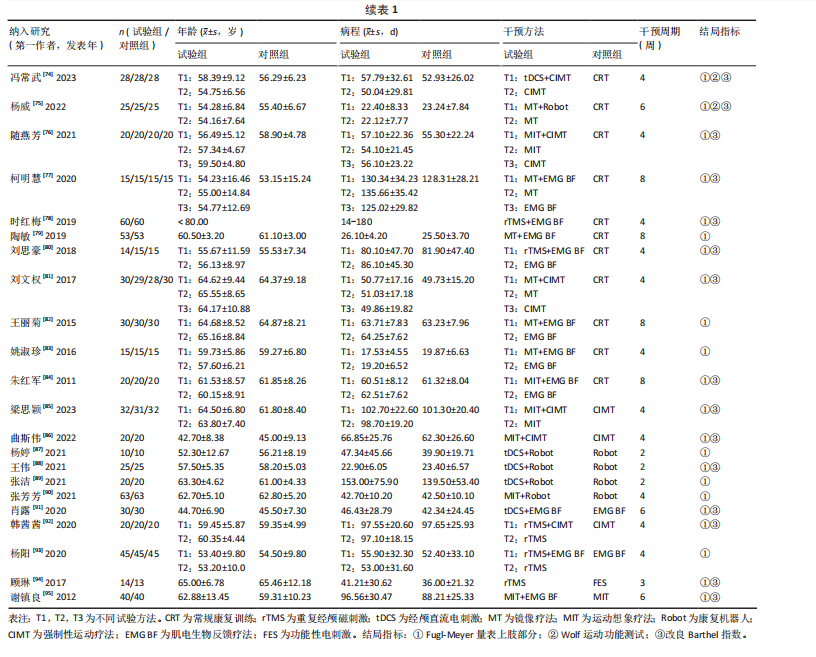
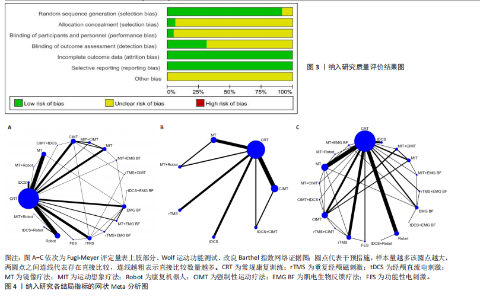
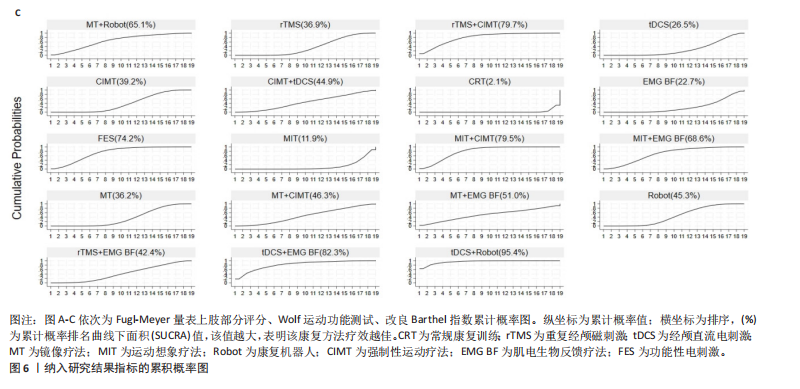
2.1 文献检索结果 通过检索数据库获得文献8 020篇,导入EndNoteX9自动去重、2名研究人员独立进行手工去重、初筛及复筛后最终纳入文献88篇,具体筛选流程见图2。 2.2 纳入文献的基本特征 共纳入88篇文献[8-95],包含5 561例脑卒中伴上肢运动功能障碍患者,涉及19种康复方案,发表年份为2012-2024年,干预周期为2-12周,见表1。 2.3 文献的质量评价 88项研究均提及分组方式,其中7项研究仅提及随机分组[11,23,34,65,70-71,80];5项研究提及分配隐藏[9,40,50,53,61];4项研究对治疗师与患者实施双盲[9,19,23,40],8项研究对患者实施单盲[8,10,12-15,25,89];27项研究对结局指标评估者设盲[9,15,18-19,22-23,25-28,33,40,44,49-50,53-57,61,67,74-75,86,92,94];"
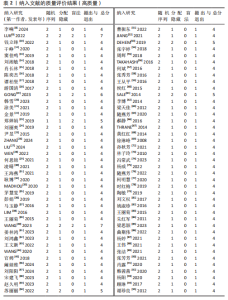
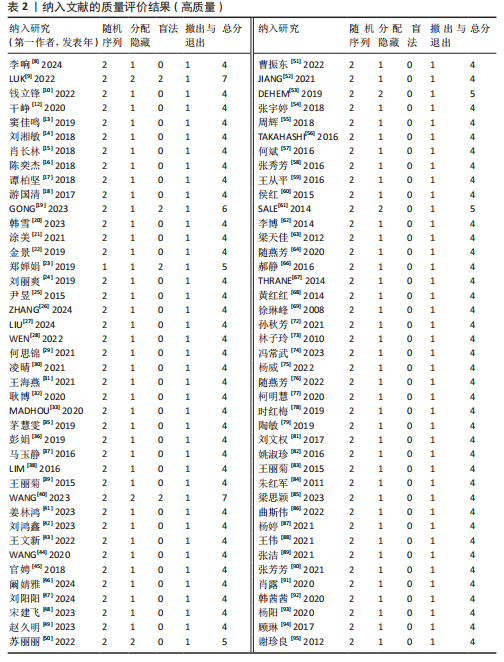
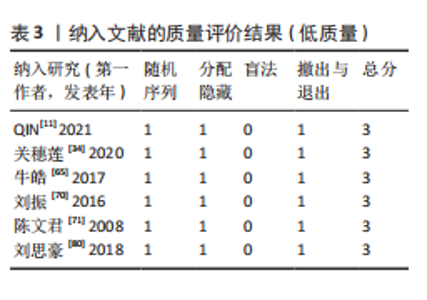
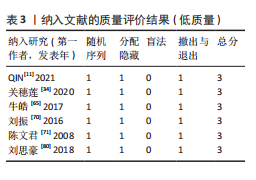
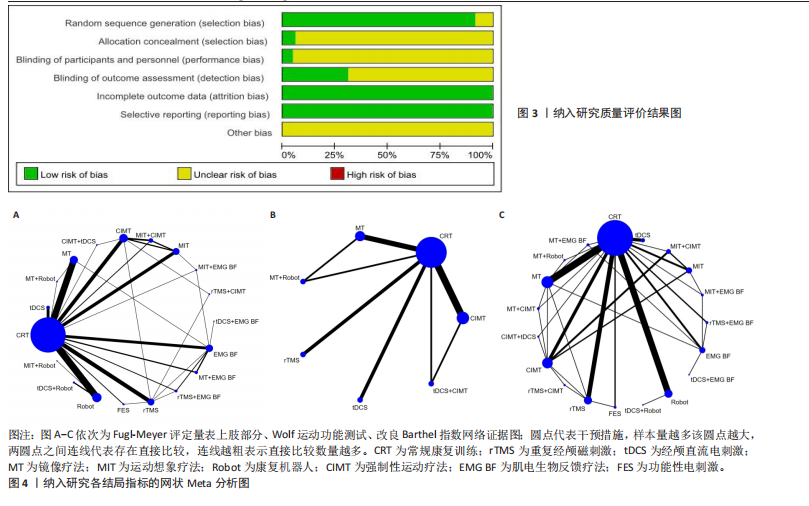
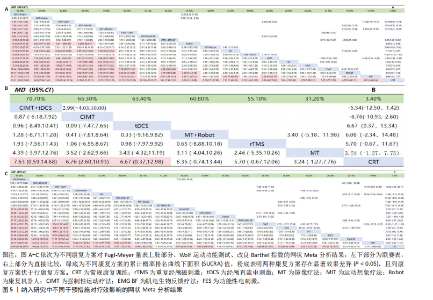
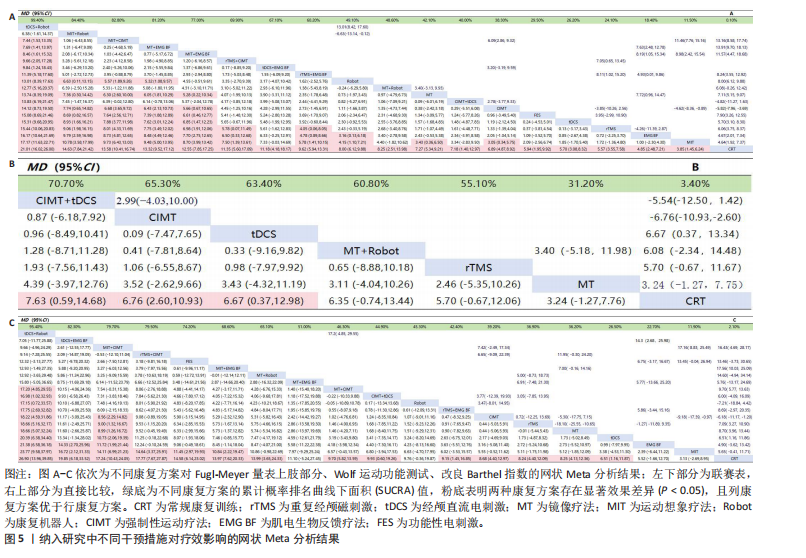
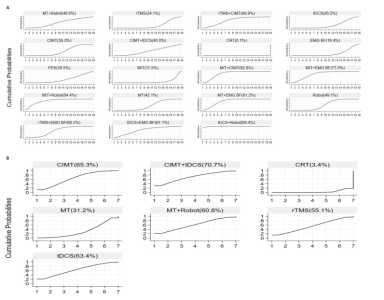
88项研究结局数据均完整,不确定是否存在其他偏倚,纳入文献的偏倚风险见图3。 采用修订版Jadad量表评估纳入研究方法学质量,结果显示:高质量研究82项[8-10,12-33,35-64,66-69,72-79,81-95],见表2,低质量研究6项[11,34,65,70-71,80],见表3,88项研究总分为3-7分,平均4.07分,纳入研究总体质量较高。 2.4 Meta分析结果 2.4.1 Fugl-Meyer量表上肢部分评分 共86项研究评估Fugl-Meyer量表上肢部分评分[8-14,16-49,51-95],包括5 474例脑卒中患者,涉及19种康复方案,网络证据图形成17个闭合环,见图4A,除常规康复疗法外,镜像疗法与Robot应用的患者最多,而常规康复疗法、强制性运动疗法、运动想象及运动想象+强制性运动疗法之间直接比较次数最多;整体不一致性检验P=0.74,表明Fugl-Meyer量表上肢部分评分整体直接与间接比较结果较一致,故采用一致性模型,通过节点分裂法进行局部不一致检验,发现强制性运动疗法与常规康复疗法比较存在局部不一致性,直接Meta结果显示:强制性运动疗法提高脑卒中患者Fugl-Meyer量表上肢部分评分显著优于常规康复疗法(MD=5.4,95%CI:3.80±7.89,P < 0.000 01)。 网状Meta分析结果表明,在19种康复方案中,与常规康复疗法对比,18种不同中枢与外周康复疗法单独或联合应用的治疗方案均可有效提高脑卒中患者Fugl-Meyer量表上肢部分评分(P < 0.05);两两比较结果显示:经颅直流电刺激+Robot提高脑卒中患者Fugl-Meyer量表上肢部分评分显著优于除运动想象+Robot以外的17种治疗方案(P < 0.05),其他两两比较详见图5A。 累计概率排序结果见图6A,19种康复方案对提高脑卒中患者Fugl-Meyer量表上肢部分评分的最佳排序依次为:经颅直流电刺激+Robot >运动想象+Robot>运动想象+强制性运动疗法>镜像疗法+肌电生物反馈疗法>运动想象+肌电生物反馈疗法>经颅磁刺激+强制性运动疗法>经颅直流电刺激+肌电生物反馈疗法>经颅磁刺激+肌电生物反馈疗法> Robot >镜像疗法+Robot >镜像疗法>强制性运动疗法+经颅直流电刺激>强制性运动疗法>功能性电刺激>经颅直流电刺激>经颅磁刺激>肌电生物反馈疗法>运动想象>常规康复疗法。 2.4.2 Wolf运动功能测试 共11项研究评估该指标[14,18,20,23,34,36,65,68-69,74-75],包括736例脑卒中患者,涉及7种康复方案,网络证据图形成2个闭合环,见图4B,除常规康复疗法外,应用镜像疗法与强制性运动疗法的患者最多,而常规康复疗法、镜像疗法、镜像疗法+Robot及常规康复疗法、强制性运动疗法、经颅直流电刺激+强制性运动疗法之间直接比较次数最多;整体不一致性检验P=0.46,采用"
"
节点分裂法进行局部不一致检验,未发现局部不一致性,使用一致性模型进行分析。 网状Meta分析结果表明:强制性运动疗法+经颅直流电刺激、强制性运动疗法、经颅直流电刺激对提高患者Wolf运动功能测试评分优于常规康复疗法(P < 0.05),其余两两比较差异无显著意义(P > 0.05),见图5B。 累计概率排序结果见图6B,7种康复方案对提高脑卒中患者Wolf运动功能测试的最佳排序依次为:强制性运动疗法+经颅直流电刺激>强制性运动疗法>经颅直流电刺激>镜像疗法+Robot >经颅磁刺激>镜像疗法>常规康复疗法。 2.4.3 改良Barthel指数 共51项研究评估该指标[11-12,14-18,20,22-25,27,29,31,33-35,37-38,44-47,49-51,54,57-58,60,63-64,66,72-78,80-81,84-86,88,91-92,94-95],包括3 349例脑卒中患者,涉及19种康复方案,网络证据图形成22个闭合环,见图4C,常规康复疗法、运动想象、强制性运动疗法之间直接比较次数最多;整体不一致性检验P=0.17,节点分裂法行局部不一致检验,结果显示功能性电刺激与常规康复疗法、镜像疗法与常规康复疗法、功能性电刺激与经颅磁刺激之间两两比较存在局部不一致性,直接比较结果显示:镜像疗法提高患者改良Barthel指数评分显著优于常规康复疗法(MD=6.10,95%CI:4.12-8.09,P < 0.000 01),其余直接比较结果差异无显著意义(P=0.09)。 网状Meta分析结果表明:除镜像疗法+肌电生物反馈疗法、Robot、肌电生物反馈疗法及运动想象,14种康复方案对于提高脑卒中患者改良Barthel指数均显著优于常规康复疗法(P < 0.05);两两比较结果显示:经颅直流电刺激+ Robot与运动想象+强制性运动疗法明显优于其他康复方案(P < 0.05),但两种康复方案对比差异无显著意义(P > 0.05),见图5C。 累计概率排序结果见图6C,19种康复方案对提高脑卒中患者改良Barthel指数的最佳排序依次为:经颅直流电刺激+Robot >经颅直流电刺激+肌电生物反馈疗法>运动想"
"
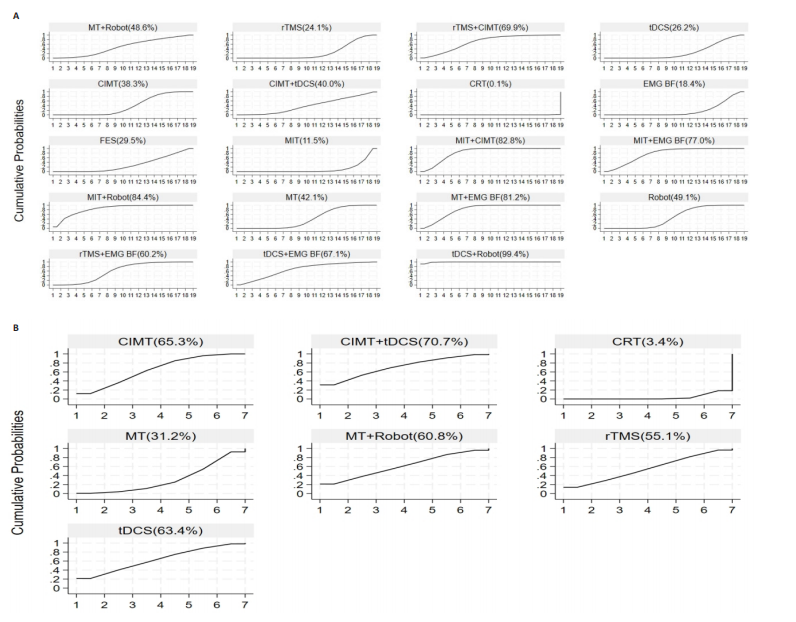
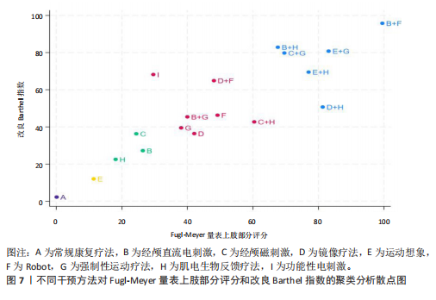
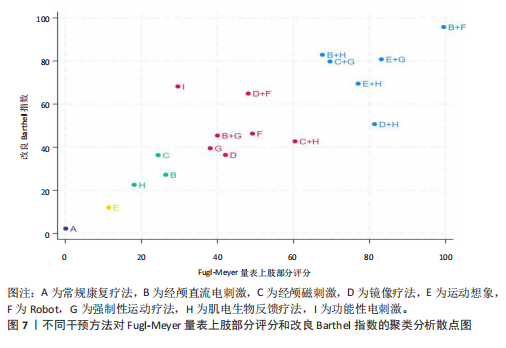
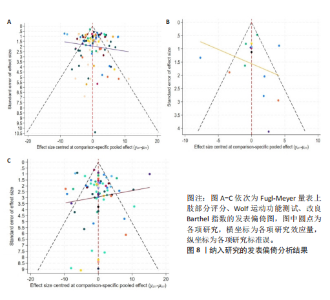
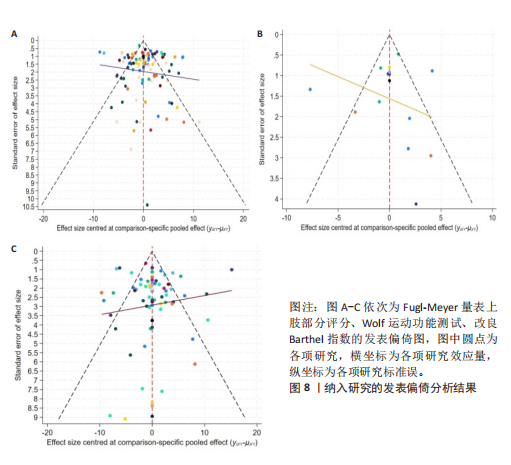
象+强制性运动疗法>经颅磁刺激+强制性运动疗法>功能性电刺激>运动想象+肌电生物反馈疗法>镜像疗法+Robot>镜像疗法+肌电生物反馈疗法>镜像疗法+强制性运动疗法>强制性运动疗法+经颅直流电刺激> Robot >经颅磁刺激+肌电生物反馈疗法>强制性运动疗法>经颅磁刺激>镜像疗法>经颅直流电刺激>肌电生物反馈疗法>运动想象>常规康复疗法。 2.4.4 聚类分析散点图 共18种康复方案同时评估Fugl-Meyer量表上肢部分评分与改良Barthel指数2个结局指标,通过整合不同康复方案对2个结局指标的SCUCRA值绘制聚类分析图,结果显示:综合改善脑卒中患者上肢运动功能及日常生活活动能力的最优康复方案为经颅直流电刺激+Robot,见图7。 2.5 敏感性分析 对Fugl-Meyer量表上肢部分评分与改良Barthel指数进行敏感性分析,鉴于功能性电刺激纳入文献数量较少,可能导致选择性偏倚,故剔除功能性电刺激后重新进行网状Meta分析。结果显示:Fugl-Meyer量表上肢部分评分的SUCRA排序为经颅直流电刺激+Robot(99.4%) >运动想象+Robot(83.9%) >运动想象+强制性运动疗法(82.0%) >镜像疗法+肌电生物反馈疗法(80.7%) >运动想象+肌电生物反馈疗法 (76.0%) >经颅磁刺激+强制性运动疗法(67.2%) >经颅直流电刺激+肌电生物反馈疗法(66.1%) >经颅磁刺激+肌电生物反馈疗法(58.2%) Robot (47.5%) >镜像疗法+ Robot(47.2%) >镜像疗法(40.8%) >强制性运动疗法+经颅直流电刺激(38.8%) >强制性运动疗法(36.7) >经颅直流电刺激(25.8%)经颅磁刺激(20.7%) >肌电生物反馈疗法(17.6%) >运动想象(11.1%) >常规康复疗法(0.1%),排序与未剔除前未发生变化,表明结果稳健;改良Barthel指数的SUCRA排序为经颅直流电刺激+Robot(97.5%) >经颅直流电刺激+肌电生物反馈疗法(85.8%) >运动想象+强制性运动疗法(81.6%) >经颅磁刺激+强制性运动疗法(80.7%) >运动想象+肌电生物反馈疗法(72.1%) >镜像疗法+Robot(69.1%) >镜像疗法+肌电生物反馈疗法(52.6%) >镜像疗法+强制性运动疗法(50.1%) >强制性运动疗法+经颅直流电刺激(48.5%) > Robot (47.4%) >经颅磁刺激+肌电生物反馈疗法(44.9%) >强制性运动疗法(40.1%) >经颅磁刺激(37.9%) >镜像疗法(29.9%) >经颅直流电刺激(27.8%) >肌电生物反馈疗法(22.8%) >运动想象(9.8%) >常规康复疗法(1.6%), 排序较前未发生变化,表明结果较稳定。 2.6 发表偏倚 3个结局指标漏斗图见图8,Fugl-Meyer量表上肢部分评分(图8A)与改良Barthel指数漏斗图(图8C)左右基本对称,大部分圆点位于漏斗图上方,表明发表偏倚可能性较小;Wolf运动功能测试漏斗图(图8B)左右对称性欠佳,提示可能存在一定发表偏倚,可能与评估Wolf运"
"
"

"
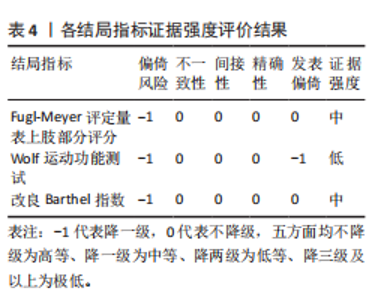
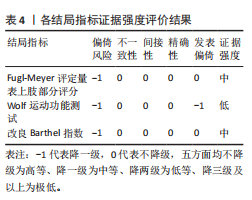
动功能测试指标的文献数量较少、导致小样本效应有关,且鉴于阳性结果更易发表,进一步导致了发表偏倚的风险,该研究结果需谨慎看待。 2.7 GRADE证据等级 鉴于纳入文献中大多数未提及分配隐藏及盲法情况,无法判断是否存在研究对象和研究人员的主观因素影响试验分组和结果评估的情况,降低证据的可靠性,可能存在偏倚风险,故对3个结局指标予以降级,另Wolf运动功能测试漏斗图对称性欠佳,可能存在小样本效应导致发表偏倚风险,予以降级。GRADE证据等级结果:Fugl-Meyer量表上肢部分评分与改良Barthel指数证据等级推荐为中等强度,Wolf运动功能测试证据等级推荐为低等强度,见表4。"
"
"
| [1] GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795-820. [2] 国家心血管病中心,中国心血管健康与疾病报告编写组.中国心血管健康与疾病报告2023概要[J].中国循环杂志,2024, 39(7):625-660. [3] PURTON J, SIM J, HUNTER SM. The experience of upper-limb dysfunction after stroke: a phenomenological study. Disabil Rehabil. 2021;43(23):3377-3386. [4] 彭通,赵雅宁,刘瑶,等.三种类型经颅直流电刺激对脑卒中上肢偏瘫患者干预效果的网状Meta分析[J].中国循证医学杂志,2022,22(12):1436-1444. [5] AHMED I, MUSTAFAOGLU R, ROSSI S, et al. Non-invasive Brain Stimulation Techniques for the Improvement of Upper Limb Motor Function and Performance in Activities of Daily Living After Stroke: A Systematic Review and Network Meta-analysis. Arch Phys Med Rehabil. 2023;104(10):1683-1697. [6] 贾杰.“中枢-外周-中枢”闭环康复:脑卒中后手功能康复新理念[J].中国康复医学杂志,2016,31(11):1180-1182. [7] 王帅,王东岩,郑应康,等.基于脑-肢协同调控治疗卒中后肢体运动功能障碍的研究进展[J].华西医学,2023,38(1): 140-146. [8] 李响,张洪蕊,曹海杰,等.重复经颅磁刺激对脑卒中后上肢运动功能影响的功能性近红外光谱研究[J].中华物理医学与康复杂志,2024,46(2):123-128. [9] LUK KY, OUYANG HX, PANG MYC. Low-Frequency rTMS over Contralesional M1 Increases Ipsilesional Cortical Excitability and Motor Function with Decreased Interhemispheric Asymmetry in Subacute Stroke: A Randomized Controlled Study. Neural Plast. 2022;2022:3815357. [10] 钱立锋,金文杰,朱鑫鑫,等.低频重复经颅磁刺激对脑卒中患者上肢运动功能及脑血流的影响[J].中国现代医生, 2022,60(9):88-92. [11] QIN Y, LIU X, GUO X, et al. Low-Frequency Repetitive Transcranial Magnetic Stimulation Restores Dynamic Functional Connectivity in Subcortical Stroke [published correction appears in Front Neurol. 2023;14:1272223. [12] 干峥,缪永娟,沈显山,等.1 Hz重复经颅磁刺激对脑卒中偏瘫病人上肢功能的疗效研究[J].安徽医药,2020,24(12):2377-2382. [13] 窦佳鸣,李春光,眭演祥,等.重复经颅磁刺激对脑卒中后上肢功能影响的近红外脑功能成像研究[J].中华物理医学与康复杂志,2019,41(6):418-423. [14] 刘湘敏,李光宁,陈伟英,等.低频重复经颅磁刺激对脑卒中后手部运动功能康复的疗效[J].中国慢性病预防与控制, 2018,26(12):933-935. [15] 肖长林,潘翠环,陈艳,等.高频重复经颅磁刺激对脑卒中患者手功能康复的疗效[J].中国康复理论与实践,2018,24(2): 179-183. [16] 陈奕杰,余茜,崔微,等.重复经颅磁刺激联合躯体感觉诱发电位及运动诱发电位在脑卒中治疗中的应用[J].实用医学杂志,2018,34(24):4115-4119. [17] 谭柏坚,卢艳湘.低频重复经颅磁刺激结合康复训练在脑卒中患者上肢运动功能康复中的疗效评价[J].癫痫与神经电生理学杂志,2018,27(2):101-103. [18] 游国清,梁慧英,游桂娟,等.重复经颅磁刺激改善亚急性期缺血性脑卒中患者上肢运动功能的随机对照研究[J].中国医药科学,2017,7(7):187-189213. [19] GONG Q, YAN R, CHEN H, et al. Effects of cerebellar transcranial direct current stimulation on rehabilitation of upper limb motor function after stroke. Front Neurol. 2023;14:1044333. [20] 韩雪,李欣,宋桂芹.经颅直流电刺激对亚急性期缺血性脑卒中患者上肢运动功能和体感诱发电位的影响[J].中国康复, 2023,38(5):272-276. [21] 涂美,向仕东,王海涛.康复训练结合阳极经颅直流电刺激对脑梗死后恢复期患者日常生活的影响[J].中国医师杂志, 2021,23(4):582-585. [22] 金景,蒋苏,潘晓励,等.经颅直流电刺激联合康复训练对脑卒中偏瘫患者认知功能及肢体运动功能的影响[J].中华物理医学与康复杂志,2019,41(6):415-417. [23] 郑婵娟,夏文广,段璨,等.经颅直流电刺激对脑卒中后上肢及手功能恢复的随机对照研究[J].中国康复,2019,34(12): 623-626. [24] 刘丽爽,杜文军,刘爱贤. 经颅直流电刺激对脑卒中患者的影响[J].中国实用护理杂志,2019,35(20):1537-1540. [25] 尹昱,左秀芹,吕艳玲,等.经颅直流电刺激对脑卒中患者上肢运动功能障碍的疗效[J].中国康复理论与实践,2015, 21(7):830-833. [26] ZHANG K, DING L, WANG X, et al. Evidence of mirror therapy for recruitment of ipsilateral motor pathways in stroke recovery: A resting fMRI study. Neurotherapeutics. 2024;21(2):e00320. [27] LIU W, CHENG X, RAO J, et al. Motor imagery therapy improved upper limb motor function in stroke patients with hemiplegia by increasing functional connectivity of sensorimotor and cognitive networks. Front Hum Neurosci. 2024;18: 1295859. [28] WEN X, LI L, LI X, et al. Therapeutic Role of Additional Mirror Therapy on the Recovery of Upper Extremity Motor Function after Stroke: A Single-Blind, Randomized Controlled Trial. Neural Plast. 2022;2022:8966920. [29] 何思锦,陈小霞,罗凯旋,等.镜像疗法联合作业治疗对脑卒中偏瘫上肢运动功能和日常生活活动能力的影响[J].昆明医科大学学报,2021,42(6):129-133. [30] 凌晴,胡世红,王田尧,等.镜像疗法促进脑卒中上肢功能恢复和皮质脊髓束重塑的弥散张量成像研究[J].中国康复理论与实践,2021,27(1):31-36. [31] 王海燕,林莉,蔡桂程,等.镜像疗法对脑卒中偏瘫患者的康复效果观察[J].神经损伤与功能重建,2021,16(7):410-413. [32] 耿博,冯翰超,张健,等.基于镜像视觉反馈的康复训练治疗老年脑卒中偏瘫患者疗效研究[J].康复学报,2020,30(4): 270-274. [33] MADHOUN HY, TAN B, FENG Y, et al. Task-based mirror therapy enhances the upper limb motor function in subacute stroke patients: a randomized control trial. Eur J Phys Rehabil Med. 2020;56(3):265-271. [34] 关穗莲,曹全荣,符汉平,等.镜像疗法对脑卒中偏瘫患者手功能影响的研究[J].按摩与康复医学,2020,11(22):39-41. [35] 茅慧雯,李艳,陈烨,等.镜像视觉反馈训练对脑卒中患者认知及上肢功能的效果[J].中国康复理论与实践,2019, 25(3):284-288. [36] 彭娟,杨仕彬,胥方元,等.早期介入镜像疗法对缺血性脑卒中患者偏瘫肢体功能恢复的影响[J].中华物理医学与康复杂志,2019,41(3):178-183. [37] 马玉静,勾丽洁,王文清,等.镜像视觉反馈疗法对脑卒中后偏瘫患者上肢功能及其日常生活活动能力的影响[J].中华物理医学与康复杂志,2016,38(2):141-143. [38] LIM KB, LEE HJ, YOO J, et al. Efficacy of Mirror Therapy Containing Functional Tasks in Poststroke Patients. Ann Rehabil Med. 2016;40(4):629-636. [39] 王丽菊,陈立早,欧艺,等.镜像视觉反馈和肌电生物反馈对脑卒中偏瘫患者上肢功能的影响[J].中国康复理论与实践, 2015,21(2):202-206. [40] WANG H, XIONG X, ZHANG K, et al. Motor network reorganization after motor imagery training in stroke patients with moderate to severe upper limb impairment. CNS Neurosci Ther. 2023;29(2):619-632. [41] 姜林鸿,刘晓丹,孙萍萍,等.运动想象训练对卒中后患者上肢运动功能恢复的影响及静息态fNIRS脑网络特征研究[J].中国康复医学杂志,2023,38(11): 1505-1513. [42] 刘鸿鑫,刘晓旭,陈志天,等.功能近红外光谱成像技术评估运动想象疗法对脑卒中患者脑功能的影响[J].神经损伤与功能重建,2023,18(6):363-366. [43] 王文新,游小芳.运动想象结合病房日常训练对改善脑卒中患者上肢运动功能的影响[J].深圳中西医结合杂志,2022, 32(17):111-113. [44] WANG X, WANG H, XIONG X, et al. Motor Imagery Training After Stroke Increases Slow-5 Oscillations and Functional Connectivity in the Ipsilesional Inferior Parietal Lobule. Neurorehabil Neural Repair. 2020;34(4):321-332. [45] 官娉,陈妍,张韶辉.作业疗法结合运动想象对脑卒中偏瘫患者的上肢与手功能的影响[J].临床和实验医学杂志,2018, 17(6):647-649。 [46] 阚婧雅,刘曦,刘嘉奕,等.上肢机器人辅助作业疗法对脑卒中偏瘫患者上肢功能及日常生活活动能力的影响[J].机器人外科学杂志(中英文),2024,5(4):548-553. [47] 刘阳阳,徐唱,刘洋.上肢康复机器人辅助康复训练对亚急性期脑卒中偏瘫患者上肢运动功能的影响[J].河北医科大学学报,2024,45(3):321-325 [48] 宋建飞,戴磊,秦郑圆,等.上肢康复机器人辅助训练对脑卒中患者上肢功能的效果:基于功能性近红外光谱[J].中国康复理论与实践,2023,29(11):1339-1345. [49] 赵久明,李月,张佳奇,等.上肢康复机器人治疗脑卒中偏瘫患者上肢功能障碍的疗效[J].机器人外科学杂志(中英文), 2023,4(6):507-511. [50] 苏丽丽,方小养,林玲,等.上肢康复机器人训练对亚急性脑卒中患者认知和上肢运动功能的效果[J].中国康复理论与实践,2022,28(5):508-514. [51] 曹振东,杨彩霞,褚延利,等.上肢康复机器人治疗脑卒中患者上肢功能的临床疗效研究[J].中国疗养医学,2022, 31(1):68-70. [52] JIANG S, YOU H, ZHAO W, et al. Effects of short-term upper limb robot-assisted therapy on the rehabilitation of sub-acute stroke patients. Technol Health Care. 2021; 29(2):295-303. [53] DEHEM S, GILLIAUX M, STOQUART G, et al. Effectiveness of upper-limb robotic-assisted therapy in the early rehabilitation phase after stroke: A single-blind, randomised, controlled trial. Ann Phys Rehabil Med. 2019;62(5):313-320. [54] 张宇婷,黄颖珺,马佼佼,等.上肢智能反馈机器人训练对脑卒中患者上肢功能及日常生活活动能力的影响[J].江苏医药,2018,44(10):1206-1208. [55] 周辉,伊传建.上肢机器人联合作业疗法对脑卒中恢复期上肢功能的临床疗效[J].按摩与康复医学,2018,9(6):24-26. [56] TAKAHASHI K, DOMEN K, SAKAMOTO T, et al. Efficacy of Upper Extremity Robotic Therapy in Subacute Poststroke Hemiplegia: An Exploratory Randomized Trial. Stroke. 2016;47(5):1385-1388. [57] 何斌,张超,刘璇.上肢机器人辅助疗法对急性期脑卒中患者上肢运动功能的效果[J].中国康复理论与实践,2016, 22(6):688-692 [58] 张秀芳,高晓盟,赵娜,等.上肢康复机器人训练对脑卒中偏瘫患者上肢功能恢复的影响.中华物理医学与康复杂志, 2016,38(3):180-182. [59] 王从平,曾艳,贾敏,等.上肢机器人在脑梗死偏瘫患者康复治疗中的应用[J].神经损伤与功能重建,2016,11(6): 558-559. [60] 侯红,范亚蓓,吴玉霞,等.康复机器人辅助训练对偏瘫患者上肢功能及日常生活活动能力的影响[J].中国康复医学杂志,2015,30(10):1013-1016. [61] SALE P, FRANCESCHINI M, MAZZOLENI S, et al. Effects of upper limb robot-assisted therapy on motor recovery in subacute stroke patients. J Neuroeng Rehabil. 2014; 11:104. [62] 李博,欧阳玉娟.上肢机器人结合常规康复训练对偏瘫患者上肢功能影响的临床观察[J].中国医学装备,2014,11(B12): 260-261. [63] 梁天佳,吴小平,莫明玉.上肢康复机器人训练对偏瘫患者上肢功能恢复的影响[J].中国康复医学杂志,2012, 27(3):254-256. [64] 随燕芳,林夏妃,王悦,等.改良强制性运动疗法对脑梗死患者上肢功能及表面肌电信号的影响[J].海南医学,2020, 31(9):1106-1109. [65] 牛皓,于少平,姜斌,等.改良强制性运动疗法对早期脑卒中偏瘫上肢运动功能的影响[J].青岛大学医学院学报, 2017,53(6):672-675. [66] 郝静,李萌.强制性运动方案对脑卒中偏瘫上肢功能障碍患者的疗效[J].神经损伤与功能重建,2016,11(1):84-85. [67] THRANE G, ASKIM T, STOCK R, et al. Efficacy of Constraint-Induced Movement Therapy in Early Stroke Rehabilitation: A Randomized Controlled Multisite Trial. Neurorehabil Neural Repair. 2015; 29(6):517-525. [68] 黄红红,王凌星,张泉香,等.强制性运动疗法对脑卒中亚急性早期偏瘫患者上肢功能恢复的影响[J].中华物理医学与康复杂志,2014,36(11):838-841. [69] 徐琳峰,宋水江,杨丹丹,等.强制性运动治疗对脑卒中偏瘫患者上肢功能及日常生活活动能力的影响[J].中华物理医学与康复杂志,2008,30(2):121-123. [70] 刘振,吴建贤.肌电生物反馈治疗脑卒中偏瘫患者肩关节运动功能的疗效研究[J].安徽医学,2016,37(6):662-665. [71] 陈文君,李建华,寿依群,等.表面肌电生物反馈治疗对偏瘫患者上肢功能的影响[J].中华物理医学与康复杂志, 2008,30(8):548-550. [72] 孙秋芳,王卫丽,冯学伟.早期功能性电刺激主导下的床旁作业治疗对脑卒中患者手功能障碍的影响[J].数理医药学杂志,2021,34(10):1554-1556. [73] 林子玲,陈玲,燕铁斌,等.功能性电刺激改善脑卒中患者上肢功能的随机对照研究[J].中国康复医学杂志,2010, 25(2):152-155. [74] 冯常武,朴政文,柯志钢.经颅直流电刺激联合改良强制性使用技术在脑卒中患者中的疗效观察[J].中国康复,2023, 38(8):470-474. [75] 杨威,曾杜纯,周航帆,等.镜像疗法联合上肢康复机器人训练对脑卒中患者上肢功能的影响[J].护理与康复,2022, 21(8):7-11. [76] 随燕芳,林夏妃,王悦,等.改良强制性运动联合运动想象对脑梗死患者上肢运动功能及表面肌电信号影响的研究[J]. 中国医学装备,2021,18(10):92-96. [77] 柯明慧,金星,孟兆祥,等.镜像疗法结合肌电生物反馈对脑卒中恢复期患者上肢功能的影响[J].中国康复,2020, 35(4):183-186. [78] 时红梅,李依芃,徐玉丽,等.重复经颅磁刺激联合生物反馈对脑卒中上肢运动功能的康复评价[J].中国实用神经疾病杂志,2019,22(8):847-852. [79] 陶敏,钟诚,彭冠铭,等.生物反馈结合镜像疗法治疗脑卒中对上肢功能产生的影响分析[J].当代医学,2019,25(15):152-153. [80] 刘思豪,李哲,刘骞豪,等.低频重复经颅磁刺激联合肌电生物反馈疗法对脑卒中患者上肢功能的临床研究[J].中国康复,2018,33(6):451-454. [81] 刘文权,曾德良,梁宇健,等.镜像视觉反馈联合改良强制性运动治疗对脑卒中偏瘫患者上肢功能的疗效观察[J].广州医药,2017,48(5):19-23 [82] 王丽菊,陈立早,欧艺,等.镜像视觉反馈和肌电生物反馈对脑卒中偏瘫患者上肢功能的影响[J].中国康复理论与实践, 2015,21(2):202-206. [83] 姚淑珍,勾丽洁,刘旭东,等.镜像疗法结合肌电生物反馈疗法促进脑卒中偏瘫患者上肢功能重建的临床观察[J].中华物理医学与康复杂志,2016,38(10):746-749. [84] 朱红军,何怀,刘传道,等.运动想象疗法结合肌电生物反馈对脑卒中偏瘫患者上肢功能恢复的影响[J].中华物理医学与康复杂志,2011,33(6):443-446. [85] 梁思颖,李灵晓. 运动想象训练联合强制性运动疗法对脑卒中偏瘫患者上肢运动功能的影响[J]. 中华物理医学与康复杂志,2023,45(2):128-130. [86] 曲斯伟,朱琳,严莉,等.运动想象联合改良强制性运动疗法对脑卒中患者上肢运动功能的影响[J].中国康复,2022, 37(3):131-135. [87] 杨婷,陈慧柚,高政,等.经颅直流电刺激联合上肢机器人训练对脑卒中后偏瘫上肢运动功能影响的磁共振弥散张量成像研究[J].中华物理医学与康复杂志, 2021,43(9):781-786 [88] 王伟,宋为群,张艳明,等.经颅直流电刺激对脑卒中患者上肢运动功能康复的效果[J].中国康复理论与实践,2021, 27(9):1082-1086 [89] 张洁,王春方,杨飞,等.阴极经颅直流电刺激联合机器人治疗对脑卒中后上肢功能障碍的影响[J].中华物理医学与康复杂志,2021,43(3):235-238 [90] 张芳芳,周磊,朱慧姗.运动想象联合康复机器人在卒中偏瘫上肢运动功能恢复中的应用效果观察[J].北京医学,2021, 43(6):525-529 [91] 肖露,代菁,樊巍,等. tDCS联合肌电生物反馈改善脑卒中上肢运动功能障碍的疗效观察[J].中国康复,2020,35(9):459-462 [92] 韩茜茜,徐宁,王秀秀,等. 强制性运动疗法联合重复经颅磁刺激对脑卒中患者上肢运动功能的影响[J]. 中华物理医学与康复杂志,2020,42(12):1067-1071. [93] 杨阳,胡利杰,邹丽丽,等. 重复经颅磁刺激联合肌电生物反馈对脑卒中患者上肢功能恢复的影响[J]. 中华物理医学与康复杂志,2020,42(5):415-418. [94] 顾琳,高怡,查丽偲,等. 重复经颅磁刺激与功能性电刺激对脑梗死后上肢运动功能的影响比较[J]. 中国医学前沿杂志(电子版),2017,9(3):77-80. [95] 谢镇良,冯尚武,黄顺仪,等. 运动想象联合生物反馈治疗对脑卒中患者上肢功能障碍的疗效观察[J]. 中华物理医学与康复杂志,2012,34(4):272-274. [96] TAUCHI Y, KYOUGOKU M, TAKAHASHI K, et al. Dimensionality and item-difficulty hierarchy of the Fugl-Meyer assessment of the upper extremity among Japanese patients who have experienced stroke. Top Stroke Rehabil. 2022;29(8):579-587. [97] 吴娱倩,张玉梅,孟霞,等.Wolf运动功能测试量表评定卒中患者偏瘫侧上肢功能的效度和信度研究[J].中国卒中杂志, 2022,17(3):244-250. [98] 金冬梅,曾鑫鑫,薛晶晶,等.中文版改良躯干损伤量表在脑卒中患者中的信度与效度研究[J].中国康复医学杂志, 2021,36(7):787-792. [99] O’BRIEN AT, BERTOLUCCI F, TORREALBA-ACOSTA G, et al. Non-invasive brain stimulation for fine motor improvement after stroke: a meta-analysis. Eur J Neurol. 2018;25(8):1017-1026. [100] STRAUDI S, FREGNI F, MARTINUZZI C, et al. tDCS and Robotics on Upper Limb Stroke Rehabilitation: Effect Modification by Stroke Duration and Type of Stroke. Biomed Res Int. 2016;2016:5068127. [101] CERASA A, PIGNOLO L, GRAMIGNA V, et al. Exoskeleton-Robot Assisted Therapy in Stroke Patients: A Lesion Mapping Study. Front Neuroinform. 2018;12:44. [102] 眭有昕,郭川,朱仕哲,等.经颅直流电刺激联合虚拟现实康复机器人对脑梗死后上肢功能影响的临床研究[J].中国脑血管病杂志,2022,19(12):801-808. [103] REIS J, SCHAMBRA HM, COHEN LG, et al. Noninvasive cortical stimulation enhances motor skill acquisition over multiple days through an effect on consolidation. Proc Natl Acad Sci U S A. 2009;106(5):1590-1595. [104] ARIAS P, CORRAL-BERGANTIÑOS Y, ROBLES-GARCÍA V, et al. Bilateral tDCS on Primary Motor Cortex: Effects on Fast Arm Reaching Tasks [published correction appears in PLoS One. 2016 ;11(9):e0163714. [105] GIACOBBE V, KREBS HI, VOLPE BT, et al. Transcranial direct current stimulation (tDCS) and robotic practice in chronic stroke: the dimension of timing. NeuroRehabilitation. 2013;33(1): 49-56. [106] 燕铁斌.积极开展“脑-肢协同治疗技术”的临床应用研究[J].中国康复医学杂志, 2021,36(10):1195-1197. [107] 徐硕,贾杰.“中枢-外周-中枢”闭环康复:脑卒中后手功能康复新理念的临床应用进展[J].中国康复医学杂志, 2024,39(10):1537-1541. [108] LI LL, WU JJ, LI KP, et al. Comparative efficacy of different noninvasive brain stimulation protocols on upper-extremity motor function and activities of daily living after stroke: a systematic review and network meta-analysis. Neurol Sci. 2024;45(8): 3641-3681. [109] BAI X, GUO Z, HE L, et al. Different Therapeutic Effects of Transcranial Direct Current Stimulation on Upper and Lower Limb Recovery of Stroke Patients with Motor Dysfunction: A Meta-Analysis. Neural Plast. 2019;2019: 1372138. [110] 柯嘉洽,邹晓佩,王春燕,等.经颅直流电刺激和经颅磁刺激在脑卒中上肢运动功能恢复的应用进展[J].中国神经精神疾病杂志,2021,47(1):50-55. [111] 陈波,孟兆祥,苏敏,等. 镜像疗法在脑卒中偏瘫患者早期康复中的应用进展[J]. 中华物理医学与康复杂志,2020,42(1): 90-94. [112] 赵艳,唐迪,李月,等.康复机器人结合运动想象疗法对脑卒中患者上肢运动功能康复的效果[J].海军医学杂志,2024, 45(10):1035-1040. [113] 姚玉峰,裴硕,郭军龙,等.上肢康复机器人研究综述[J].机械工程学报,2024, 60(11):115-134. [114] 田安妮,杨晶,孙晶,等.康复机器人辅助训练对不同阶段脑卒中患者手运动功能恢复效果的meta分析[J/OL].中国全科医学,1-11[2025-02-02].http://kns.cnki.net/kcms/detail/13.1222.R.20241031.1019.002.html. [115] DEE M, LENNON O, O’SULLIVAN C. A systematic review of physical rehabilitation interventions for stroke in low and lower-middle income countries. Disabil Rehabil. 2020;42(4):473-501. [116] BORZUOLA R, LAUDANI L, LABANCA L, et al. Superimposing neuromuscular electrical stimulation onto voluntary contractions to improve muscle strength and mass: A systematic review. Eur J Sport Sci. 2023; 23(8):1547-1559. [117] MARQUEZ-CHIN C, POPOVIC MR. Functional electrical stimulation therapy for restoration of motor function after spinal cord injury and stroke: a review. Biomed Eng Online. 2020;19(1):34. [118] 余梦婷,李壮苗,燕文娟,等.肌电生物反馈治疗脑卒中后病人上肢运动功能障碍效果的Meta分析[J].护理研究,2021, 35(10):1697-1710. |
| [1] | Leng Xiaoxuan, Yu Zifu, Cao Xinyan, Gao Shiai, Chen Jinhui, Liu Xihua. Balance function and its influencing factors in patients with post-stroke hemiplegia [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(18): 4611-4617. |
| [2] | Gao Zan, Liu Yixuan, Zhang Lichen, Hou Bing, Tang Yalei, Li Shumei, Che Pengcheng, Dou Na. Network meta-analysis of robot-assisted gait training interventions on lower limb motor function in stroke patients [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(16): 4219-4228. |
| [3] | Ma Shanxin, Zheng Jianling, Cheng Jian, Lin Xi, Li Qiuyuan, Wang Li, Zeng Yangkang, Song Luping. Early intelligent active assistance in walking for hemiplegic patients under suspension protection: #br# a randomized controlled trial [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(12): 3075-3082. |
| [4] | Gao Shiai, Chen Jinhui, Cao Xinyan, Leng Xiaoxuan, Liu Xihua. Abdominal electrical stimulation combined with core stabilization training improves balance and cough function in patients with stroke pseudobulbar palsy [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(11): 2736-2744. |
| [5] | Yang Yuanyuan, Zhou Shanshan, Cheng Xiaofei, Feng Luye, Tang Jiqin. Network meta-analysis of non-invasive brain stimulation in the treatment of lower limb motor dysfunction after stroke [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(4): 1008-1018. |
| [6] | Wang Xuesong, Wang Yue, Xu Yan, Zeng Wenhui, Lu Wenming, Tang Xingkun, Chen Wenjie, Ye Junsong. Brain-computer interface combined with different therapies for limb dysfunction in stroke patients: effectiveness and mechanism analysis [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(30): 6538-6546. |
| [7] | Cao Haijie, Song Huijie, Sun Yalu, Zhang Guangyou, Li Xiang. A wearable exoskeleton with posture feedback improves abnormal gait in patients with stroke [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(24): 5127-5133. |
| [8] | Zou Mengyao, Wang Junhua, Qin Pengfei, Zhong Weihua. Knowledge graph analysis of virtual reality technology in stroke treatment [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(26): 4224-4233. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||