Chinese Journal of Tissue Engineering Research ›› 2024, Vol. 28 ›› Issue (12): 1907-1913.doi: 10.12307/2024.029
Previous Articles Next Articles
Stepwise treatment strategy for spontaneous osteonecrosis of the medial femoral condyle of the knee joint
Pan Jianke1, Yang Meiping2, Han Yanhong1, Zhao Di2, Huang Hetao1, Cao Houran1, Liu Jun1, 2, 3, Luo Minghui1, Li Xiang1, Chen Hongyun1, Yang Weiyi1
- 1Department of Sports Medicine, Second Affiliated Hospital of Guangzhou University of Chinese Medicine (Guangdong Provincial Hospital of Chinese Medicine), Guangzhou 510120, Guangdong Province, China; 2Second Clinical Medical College of Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China; 3Guangdong Second Hospital of Chinese Medicine, Guangzhou 510095, Guangdong Province, China
-
Received:2023-01-28Accepted:2023-03-29Online:2024-04-28Published:2023-08-23 -
Contact:Yang Weiyi, MD, Chief physician, Department of Sports Medicine, Second Affiliated Hospital of Guangzhou University of Chinese Medicine (Guangdong Provincial Hospital of Chinese Medicine), Guangzhou 510120, Guangdong Province, China -
About author:Pan Jianke, MD, Associate chief physician, Department of Sports Medicine, Second Affiliated Hospital of Guangzhou University of Chinese Medicine (Guangdong Provincial Hospital of Chinese Medicine), Guangzhou 510120, Guangdong Province, China -
Supported by:National Natural Science Foundation of China (Youth Program), No. 82004386 (to PJK); Natural Science Foundation of Guangdong Province (General Project), No. 2022A15150117000 (to PJK)
CLC Number:
Cite this article
Pan Jianke, Yang Meiping, Han Yanhong, Zhao Di, Huang Hetao, Cao Houran, Liu Jun, Luo Minghui, Li Xiang, Chen Hongyun, Yang Weiyi. Stepwise treatment strategy for spontaneous osteonecrosis of the medial femoral condyle of the knee joint[J]. Chinese Journal of Tissue Engineering Research, 2024, 28(12): 1907-1913.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
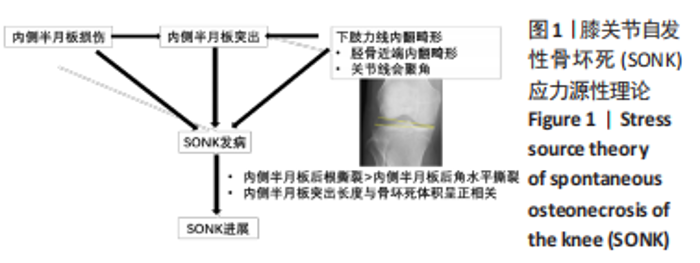
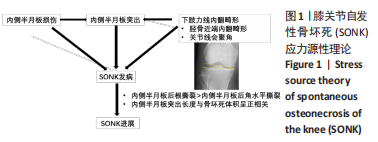
2.1 发病机制 2.1.1 血管源性理论 各种原因导致微循环的继发性血栓形成,导致血管闭塞引起骨髓水肿,致使骨内压力增高和骨缺血,继而出现骨坏死[9-11]。 2.1.2 创伤源性理论 认为由创伤因素导致的软骨下微骨折;进而造成水肿引起骨髓腔的压力增高,继而导致局部缺血,最终引起骨坏死,文献报道只有不到10%的患者有创伤史[1]。 2.1.3 应力源性理论 应力源性理论认为长期反复的应力负荷作用于骨质疏松的软骨下骨,可引起软骨下骨的微骨折,进而导致骨坏死[6,12]。该理论主要针对膝关节股骨内侧髁的SONK,涉及内侧半月板损伤、内侧半月板外突和下肢力线内翻畸形的问题,见图1。"
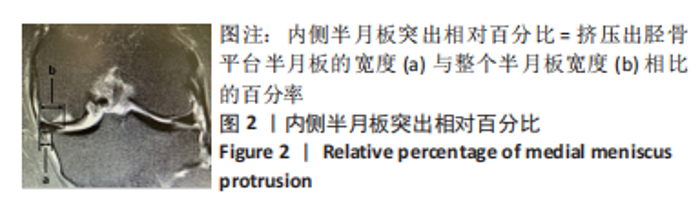
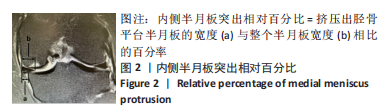
(1)内侧半月板损伤:最早NORMAN等[3]于1978年利用关节造影检查 27个SONK膝关节中有21个 (78%) 半月板撕裂,提出内侧半月板碎片边缘的应力集中可能导致股骨髁缺血性坏死,老年患者通过关节造影早期发现内侧半月板撕裂并及时治疗,对于避免“自发性”骨坏死的晚期变化可能很重要。HUSSAIN等[6]纳入26篇关于SONK病因分析的文献,26 篇文献中有 21 篇(80.7%)涉及半月板在SONK发展中的作用,SONK与半月板撕裂或半月板切除术后的发展有关,以内侧半月板撕裂、后根撕裂最为常见。ROBERTSON等[5]通过MRI及关节镜检查,发现在SONK患者中常可合并内侧半月板后根部的撕裂,该发生率可达到80%(24/30),15 例完全撕裂,9例部分撕裂,提出SONK可能与内侧半月板后根部撕裂后,导致股骨负重区的应力集中、软骨下骨髓水肿有关。FUJISAWA等[13]是对98例诊断为股骨内侧髁SONK患者的102膝进行了内侧开放楔形胫骨高位截骨术 (high tibial osteotomy,HTO),发现所有病例均有内侧半月板撕裂,包括2个退化、2个水平撕裂、40个放射状撕裂、4个复杂撕裂和54个内侧半月板后根撕裂,99%(101/102)的膝关节内侧半月板突出超过3 mm;SONK病例半月板撕裂率较高,导致环向应变中断,如内侧半月板后根撕裂(52.9%)或放射状撕裂(39.2%),内侧半月板突出的严重程度与SONK体积显著正相关(P < 0.001)。SUNG等[14]观察半月板损伤类型对SONK的影响:内侧半月板后根部撕裂组的半月板突出率为46.1%,平均坏死面积为423.1 mm2,内侧半月板后角水平裂组的半月板突出率为35.3%,平均坏死面积为175.8 mm2;与内侧半月板后角水平撕裂相比,后根撕裂将导致更大程度的突出和更广泛的骨坏死。 (2)内侧半月板突出:ODA等[15]发现100%(104)SONK患者中都存在内侧半月板突出,4 个SONK在发病前因膝关节疼痛体检发现内侧半月板突出,几个月后通过MRI检查显示存在SONK,提出内侧半月板突出是SONK的病因之一,内侧半月板突出的进展可能与SONK的发展有关。刘新光等[12]通过病例回顾发现SONK患者中内侧半月板突出(94.1%)和半脱位(52.9%)的发生率高,提出内侧半月板突出与 SONK 的发生有关,而且突出长度与骨坏死体积呈正相关。而膝内翻、内侧半月板根部撕裂是造成内侧半月板突出的主要危险因素[16]。HASHIMOTO等[17]随访78例SONK患者1年,其中48例行单髁置换术,30例保守治疗成功,通过患者发病3个月内的膝关节MR测量内侧半月板突出的绝对值(a)和内侧半月板突出相对百分比(挤压出胫骨平台半月板的宽度a与整个半月板宽度b相比的百分率,图2),发现单髁置换组内侧半月板突出(P=0.001)、相对突出百分比(P=0.001)及放射状撕裂发生率(P=0.021)均高于保守组,相对突出百分比是SONK患者发病后1年内行单髁置换的预测因子,相对突出百分比33%的患者是SONK进展的高危人群,早期(发病3个月内)内侧半月板相对挤压百分比≥33%是SONK 发病1年后预后不良的预测指标。"
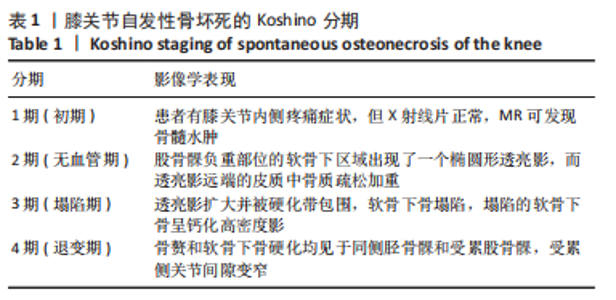
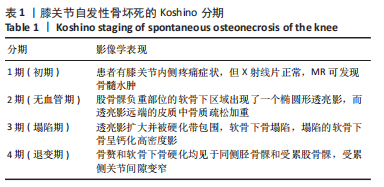
(3)下肢力线内翻畸形:AKAMATSU等[18]对分别进行保守和手术治疗的两组SONK患者(n=27膝)随访1年,发现手术组的股胫角明显大于保守组的股胫角,提出股胫角> 180°(下肢力线内翻> 6°)预示着该早期SONK患者保守治疗效果欠佳。GOSHIMA等[19]报道12例患者接受开放楔HTO治疗胫骨内侧平台SONK,其手术指佂为:①症状性骨关节炎和内侧间室的骨坏死;②存在内翻畸形(股胫角> 176°/下肢力线内翻> 2°);③活跃患者(没有年龄限制),其中11例仅胫骨内侧坏死,1例同时股骨和胫骨坏死,9例患者(75%)观察到有半月板后根撕裂,3例有水平撕裂,所有患者均有内侧半月板外突,术后所有患者膝关节活动度和临床评分皆获得显著改善,11例患者在取出钢板时接受二次关节镜检查时有9例(81.8%)观察到软骨再生。TSUKAMOTO等[4]分析Kellgren-Lawrence 1级或2级的SONK组(31膝)、骨关节炎组(32膝)病例资料,发现SONK组胫骨近端内侧角畸形(85.25±1.58)°比骨关节炎组(83.76±2.37)°更大(P=0.005),SONK组关节线会聚角(2.50±1.67)°显著大于骨关节炎组(1.66±1.39)°,SONK软骨下坏死区域的大小受胫骨近端内翻畸形的影响(呈负相关),胫骨近端内翻畸形和存在关节线会聚角有助于诱发SONK,提出胫骨近端内侧角小于84°伴有急性膝关节疼痛应尽快MRI检查。正常的膝关节线是平行的,关节线会聚角为0°,关节线会聚角的存在将引起间隙狭窄处间室的关节软骨过大的剪切应力。NAKAYAMA等[20]使用有限元模型分析发现,与正常膝关节线相比,如果关节线会聚角为5°,对关节软骨的剪切应力增加1.5倍,如果关节线会聚角为10°,剪切力增加2倍。 2.2 临床分期 最常用的分期方法是1979年Koshino分期[21- 22],见表1。Koshino分期基于临床和正位X射线影像学的结果,将SONK分为4个阶段。Koshino 1期和2期的影像在X射线片下较难区分,作者认为临床实际工作中可借助MR检查图像进行区分,Koshino1期MR图像主要以骨髓水肿为主,尚未形成边界清晰的骨坏死区(如Case1),而Koshino 2期MR上可见边界清晰的坏死区(如Case2,Case3,Case4)。此外,AGLIETTI等[23]对Koshino分期法进行了修改,将Koshino分期法的3,4期进一步细分,共分为5期。一些学者还参考继发性骨坏死的分期方法Mont分期和改良股骨头坏死的分期方法Ficat分期来对SONK进行分期[24-25]。"
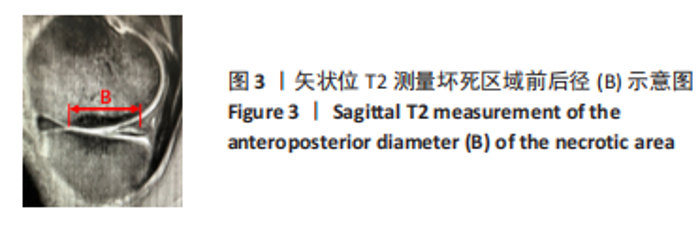
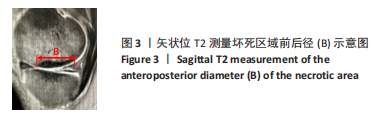
2.3 X射线检查对坏死区域的评估及对预后的影响 MUHEIM等[26]率先提出测量正位X射线片坏死区域长度A和侧位X射线片病变长度B,二者乘积为坏死区域面积大小,小于3.5 cm2的小病变区域可进行保守治疗,如果病变坏死面积大于5 cm2,应考虑胫骨截骨术和同时关节切开术移除软骨板并刮除软骨下的病灶[26]。LOTKE等[27]还进一步将病变面积分为小病变( < 3.5 cm2)、中等病变(3.5-5.0 cm2)和大病变( > 5 cm2)。AGLIETTI等[28]认为当坏死病灶面积大于5 cm2,保守治疗效果不佳。 LOTKE等[29]提出在正位X射线片上测算坏死区域的宽度占股骨髁的百分比以确定骨坏死病灶大小的方法,他们发现在累及32%的股骨内侧髁病变患者中,23个膝只有6个需要手术治疗,而超过50%股骨内侧髁坏死损伤的患者均需要人工关节置换术。AGLIETTI等[28]认为当坏死病灶宽度超过40%所累及的股骨髁时,保守治疗效果不佳。JURéUS等[30]使用LOTKE等[29]的测量方法对40例SONK患者研究发现当患者前后位X射线片病变坏死范围累及40%髁时,意味着存在骨关节炎,最终需行关节置换或截骨矫形术;提出病变范围很大(≥40%髁/前后位X射线片)或有早期骨关节炎的影像表现时,SONK保守治疗欠佳。SOUCACOS等[31]发现年龄< 65岁和病变小于股骨髁宽度50%的SONK患者行HTO治疗效果更好。 此外,KERBOUL等[32]提出在正位和侧位X射线片上勾勒出骨坏死区的轮廓,并用测角仪测量坏死所涉及弧的角度,这两个角度加在一起就得到了合并坏死角,≤150°的区域归为小病变,151°-249°的区域归为中等病变,≥250°的区域归类为大病变。MONT等[24]将MUHEIM等[26]和LOTKE等[27]的方法进行了改良,在X射线片和磁共振图像冠状面上测量病变的宽度(A)和高度(C),在矢状面上测量病变长度(B),然后用A×B×C来近似计算病变体积,并分为小(0-10 cm3)、中(11-20 cm3)和大( > 20 cm3)。但这两种测量方法均未报道能预测SONK预后。 2.4 MR检查对病变区域的评估及对预后的影响 AKAMATSU等[18]对分别进行保守和手术治疗的两组SONK患者(n=27膝)随访1年,发现手术组的坏死区域MRI上深度(15.8-21.6 mm,平均18.7 mm)明显小于保守组的MRI上深度(21.8-26.5 mm,平均24.2 mm),提出MRI上深度(矢状位坏死区域前后径,图3) > 20 mm预示该早期SONK患者保守治疗效果欠佳。"
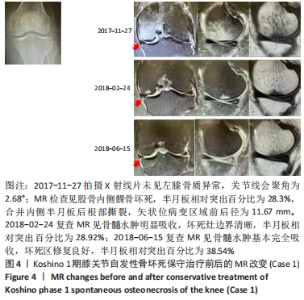
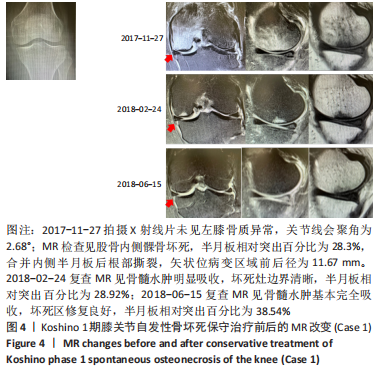
2.5 典型病例 Case 1:女,65岁,主诉:左膝关节疼痛2个月余。诊断为Koshino 1期SONK,予消炎止痛药物口服、静滴唑来膦酸钠注射液,避免负重6周,后改部分负重,12周后全负重。动态复查MR见骨髓水肿明显吸收,半年后患者临床症状消失。见图4。"
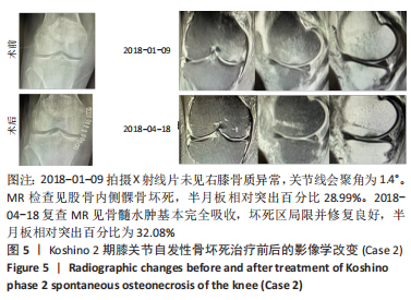
Case 2:女,65岁,主诉:右膝关节内侧疼痛1周。诊断为Koshino 2期SONK,予切开行克氏针钻孔减压,口服消炎止痛药物、钙剂及骨化三醇,不负重6周,后改部分负重至3个月,治疗3个月后患者临床症状消失。见图5。"

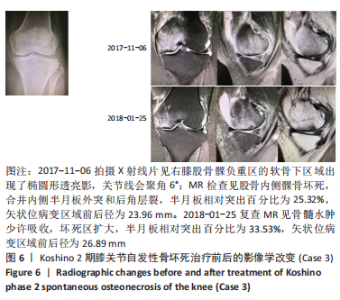
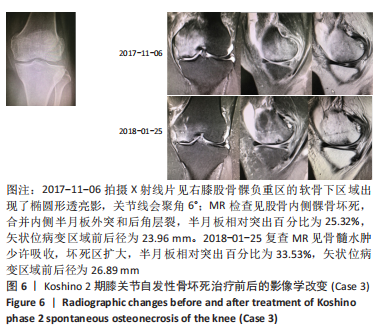
Case 3:女,69岁,主诉:左膝关节内侧疼痛1个月余。诊断为Koshino 2期SONK,MRI上深度(矢状位坏死区域前后径) > 20 mm,予克氏针钻减压,消炎止痛药物口服、静滴唑来膦酸钠注射液,嘱患者避免负重6周,后改部分负重至3个月,但患者依从性差。治疗2个月余复查MR见骨髓水肿少许吸收、坏死区扩大,患者仍有膝关节疼痛症状,建议行手术治疗,患者拒绝手术后失访。见图6。"

Case 4:男性,70岁,主诉:右膝关节内侧疼痛1年余,诊断为Koshino 2期SONK。根据LOTKE法计算已经累及44%的股骨内侧髁病变[29],MRI上深度(矢状位坏死区域前后径)> 20 mm,下肢力线内翻> 6°。予消炎止痛药物口服、静滴唑来膦酸钠注射液,避免负重6周,后改部分负重至4个月,患者右膝内侧疼痛无明显缓解,保守治疗4个月后复查MR见骨髓水肿少许吸收,坏死区扩大,内侧半月板突出较前加重,遂行右膝关节镜检查+HTO术,术后患者右膝内侧疼痛消失,行走和下蹲活动正常。术后2年拆除HTO钢板后复查MR见骨髓水肿基本完全吸收,坏死区修复良好,虽仍存在内侧半月板后角水平撕裂,但内侧半月板突出无进展,且患者右膝关节内侧无疼痛。见图7。"

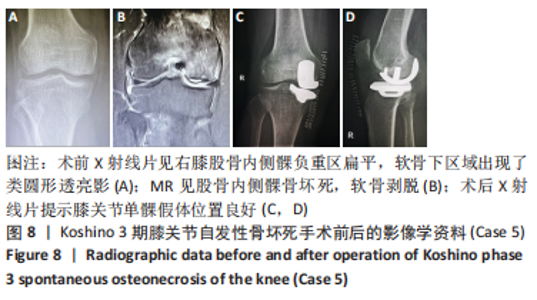
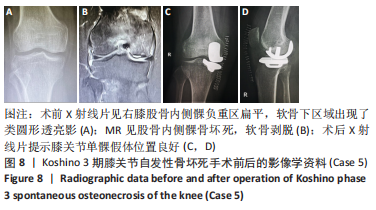
Case 5:女,61岁,右膝关节诊断为Koshino 3期SONK,行右膝内侧单髁手术治疗,术后恢复良好。见图8。"
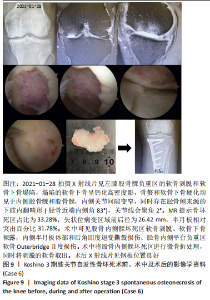
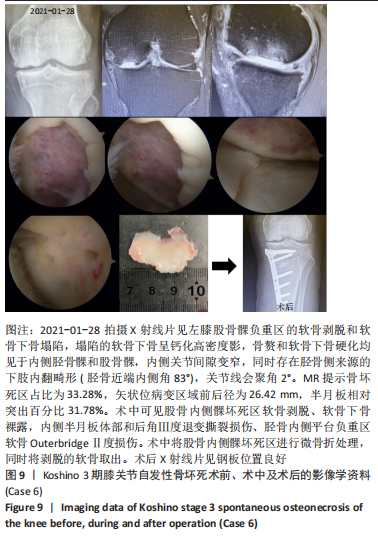
Case 6:男,64岁,主诉:左膝关节内侧疼痛6年余。诊断为Koshino 4期SONK,予关节镜检查+软骨摘除+微骨折+HTO术,术后随访2年恢复良好,行走时无左膝关节疼痛不适。见图9。"
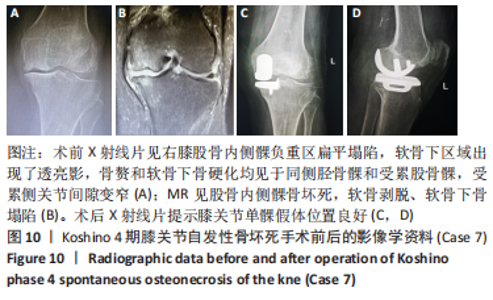
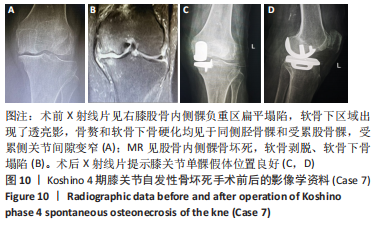
Case 7:女,81岁,诊断为Koshino 4期SONK,行内侧单髁手术治疗,术后恢复良好。见图10。"

2.6 影响保守治疗效果的重要因素 从文献和临床典型病例中可以总结得到导致膝关节股骨内侧髁SONK保守治疗效果欠佳的5个因素:①坏死区面积> 5 cm2;②坏死区占比超过髁的40%;③内侧半月板相对挤压百分比≥33%(伴或不伴随内侧半月板损伤、软骨下骨髓水肿);④MRI上坏死区深度(矢状位坏死区域前后径) > 20 mm;⑤下肢力线内翻> 6°(股胫角> 180°)。如果保守治疗3个月后症状没有减轻或MR上没有改善时,患者同时存在5个因素中的任一个,则应考虑行手术治疗。"

| [1] WILMOT AS, RUUTIAINEN AT, BAKHRU PT, et al. Subchondral insufficiency fracture of the knee: A recognizable associated soft tissue edema pattern and a similar distribution among men and women. Eur J Radiol. 2016;85(11):2096-2103. [2] AKAMATSU Y, MITSUGI N, HAYASHI T, et al. Low bone mineral density is associated with the onset of spontaneous osteonecrosis of the knee. Acta Orthop. 2012;83(3):249-255. [3] NORMAN A, BAKER ND. Spontaneous osteonecrosis of the knee and medial meniscal tears. Radiology. 1978;129(3):653-656. [4] TSUKAMOTO H, SAITO H, SAITO K, et al. Radiographic deformities of the lower extremity in patients with spontaneous osteonecrosis of the knee. Knee. 2020;27(3):838-845. [5] ROBERTSON DD, ARMFIELD DR, TOWERS JD, et al. Meniscal root injury and spontaneous osteonecrosis of the knee: an observation. J Bone Joint Surg Br. 2009;91(2):190-195. [6] HUSSAIN ZB, CHAHLA J, MANDELBAUM BR, et al. The Role of Meniscal Tears in Spontaneous Osteonecrosis of the Knee: A Systematic Review of Suspected Etiology and a Call to Revisit Nomenclature. Am J of Sports Med. 2019;47(2):501-507. [7] 沈茂荣,王平,沈欣欣,等. 膝关节自发性骨坏死相关机制的研究进展[J]. 中医临床研究,2021,13(18):113-116. [8] OCHI J, NOZAKI T, NIMURA A, et al. Subchondral insufficiency fracture of the knee: review of current concepts and radiological differential diagnoses. Jpn J Radiol. 2022;40(5):443-457. [9] MAROM N, KOCH JE, BEER Y, et al. Thrombophilia-Associated Factors in Patients with Spontaneous Osteonecrosis of the Knee. Cartilage. 2019;10(1):53-60. [10] BJÖRKMAN A, BURTSCHER IM, SVENSSON PJ, et al. Factor V Leiden and the prothrombin 20210A gene mutation and osteonecrosis of the knee. Arch Orthop Trauma Surg. 2005;125(1):51-55. [11] GLUECK CJ, FREIBERG RA, WANG P. Medical Treatment of Osteonecrosis of the Knee Associated With Thrombophilia-Hypofibrinolysis. Orthopedics. 2014;37(10):e911-e916. [12] 刘新光,王卫国,张念非,等. 膝关节自发性骨坏死与内侧半月板突出相关性的MRI观察[J]. 中国矫形外科杂志,2016,24(5):421-426. [13] FUJISAWA T, CHOE H, KUSABA Y, et al. Medial meniscus extrusion and stage are related to the size of spontaneous osteonecrosis of the knee in patients who underwent high tibial osteotomy. Knee. 2022;36:72-79. [14] SUNG JH, HA JK, LEE DW, et al. Meniscal Extrusion and Spontaneous Osteonecrosis With Root Tear of Medial Meniscus: Comparison With Horizontal Tear. Arthroscopy. 2013;29(4):726-732. [15] ODA S, FUJITA A, MORIUCHI H, et al. Medial meniscal extrusion and spontaneous osteonecrosis of the knee. J Orthop Sci. 2019;24(5):867-872. [16] 黄竞敏,李昱鸿,李冬超,等. 内侧半月板外突与半月板损伤及膝内翻的相关性研究[J]. 中华骨科杂志,2016,36(3):156-161. [17] HASHIMOTO S, TERAUCHI M, HATAYAMA K, et al. Medial meniscus extrusion as a predictor for a poor prognosis in patients with spontaneous osteonecrosis of the knee. Knee. 2021;31:164-171. [18] AKAMATSU Y, KOBAYASHI H, KUSAYAMA Y, et al. Predictive factors for the progression of spontaneous osteonecrosis of the knee. Knee Surg Sports Traumatol Arthrosc. 2017;25(2):477-484. [19] GOSHIMA K, SAWAGUCHI T, SHIGEMOTO K, et al. Open-wedge high tibial osteotomy for spontaneous osteonecrosis of the medial tibial plateau shows excellent clinical outcomes. J Exp Orthop. 2020;7(1):14. [20] NAKAYAMA H, ISEKI T, KANTO R, et al. Analysis of risk factors for poor prognosis in conservatively managed early-stage spontaneous osteonecrosis of the knee. Knee. 2016;23(1):25-28. [21] KOSHINO T, OKAMOTO R, TAKAMURA K, et al. Arthroscopy in spontaneous osteonecrosis of the knee. Orthop Clin North Am. 1979; 10(3):609-618. [22] KOSHINO T. The treatment of spontaneous osteonecrosis of the knee by high tibial osteotomy with and without bone-grafting or drilling of the lesion. J Bone Joint Surg Am.1982;64(1):47-58. [23] AGLIETTI P, BUZZI R. Idiopathic osteonecrosis of the knee. Ital J Orthop Traumatol. 1984;10(2):217-226. [24] MONT MA, BAUMGARTEN KM, RIFAI A, et al. Atraumatic osteonecrosis of the knee. J Bone Joint Surg Am. 2000;82(9):1279-1290. [25] DUANY NG, ZYWIEL MG, MCGRATH MS, et al. Joint-preserving surgical treatment of spontaneous osteonecrosis of the knee. Arch Orthop Trauma Surg. 2010;130(1):11-16. [26] MUHEIM G, BOHNE WH. Prognosis in spontaneous osteonecrosis of the knee. Investigation by radionuclide scintimetry and radiography. J Bone Joint Surg Br. 1970;52(4):605-612. [27] LOTKE PA, ECKER ML. Osteonecrosis of the knee. J Bone Joint Surg Am. 1988;70(3):470-473. [28] AGLIETTI P, INSALL JN, BUZZI R, et al. Idiopathic osteonecrosis of the knee. Aetiology, prognosis and treatment. J Bone Joint Surg Br. 1983;65(5):588-597. [29] LOTKE PA, ABEND JA, ECKER ML. The treatment of osteonecrosis of the medial femoral condyle. Clin Orthop Relat Res. 1982;(171):109-116. [30] JURÉUS J, LINDSTRAND A, GEIJER M, et al. The natural course of spontaneous osteonecrosis of the knee (SPONK): a 1- to 27-year follow-up of 40 patients. Acta Orthop. 2013;84(4):410-414. [31] SOUCACOS PN, JOHNSON EO, SOULTANIS K, et al. Diagnosis and management of the osteonecrotic triad of the knee. Orthop Clin North Am. 2004;35(3):371-381. [32] KERBOUL M, THOMINE J, POSTEL M, et al. The conservative surgical treatment of idiopathic aseptic necrosis of the femoral head. J Bone Joint Surg Br. 1974;56(2):291-296. [33] PAPE D, SEIL R, FRITSCH E, et al. Prevalence of spontaneous osteonecrosis of the medial femoral condyle in elderly patients. Knee Surg Sports Traumatol Arthrosc. 2002;10(4):233-240. [34] 王浩浩,张民,席刚,等.膝关节自发性骨坏死的保膝治疗研究进展[J]. 实用骨科杂志,2020,26(12):1127-1131. [35] FORST J, FORST R, HELLER KD, et al. Spontaneous osteonecrosis of the femoral condyle: causal treatment by early core decompression. Arch Orthop Trauma Surg. 1998;117(1-2):18-22. [36] TÍRICO L, EARLY SA, MCCAULEY JC, et al. Fresh Osteochondral Allograft Transplantation for Spontaneous Osteonecrosis of the Knee: A Case Series. Orthop J Sports Med. 2017;5(10):1808777964. [37] 侯威宇,段圆慧,孙云波,等.自体骨软骨移植联合开放楔形胫骨高位截骨术治疗膝关节自发性骨坏死的临床疗效[J]. 实用骨科杂志,2021,27(8):753-757. [38] TAKEUCHI R, ARATAKE M, BITO H, et al. Clinical results and radiographical evaluation of opening wedge high tibial osteotomy for spontaneous osteonecrosis of the knee. Knee Surg Sports Traumatol Arthrosc. 2009;17(4):361-368. [39] 叶培,董志兴,王立晖,等. 全膝关节置换术治疗晚期膝关节自发性骨坏死[J]. 中国骨与关节损伤杂志,2021,36(8):837-839. [40] CHOY WS, KIM KJ, LEE SK, et al. Medial unicompartmental knee arthroplasty in patients with spontaneous osteonecrosis of the knee. Clin Orthop Surg. 2011;3(4):279-284. |
| [1] | Guo Yingqi, Gong Xianxu, Zhang Yan, Xiao Han, Wang Ye, Gu Wenguang. Meniscus extrusion and patellofemoral joint cartilage injury and bone marrow lesions: MRI semi-quantitative score [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 600-605. |
| [2] | Zhong Hehe, Jin Ying, Liu Xiuqi, Xiang Kuan, Wu Shuhong, Peng Jiachen, Liu Yi. High tibial osteotomy combined with arthroscopy to treat degenerative tear in the posterior horn of medial meniscus combined with varus deformity of the knee [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(22): 3531-3536. |
| [3] | Chen Yiyan, Fan Zhiying, Song Honghui, Lu Aming, Zhou Haibin. Pain intensity influences the movement patterns of patients with lateral meniscus injury [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(35): 5639-5645. |
| [4] | Du Chaozheng, Zhi Jiajia, Wang Yue, Wang Xinjun, Yuan Yinpeng, Wang Yuze. Alternative strategies for tissue engineering repair of meniscus injury [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(34): 5553-5561. |
| [5] | Wang Hairuo, Liu Xi, Li Mingjin, Chen Xiaohua, Liang Ting, Ding Yongqing, Tang Xiaoli, Wang Ji, Ma Huixu. Effects of intravenous tranexamic acid infusion combined with articular cavity injection on pain and early rehabilitation after knee arthroscopy [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(36): 5766-5771. |
| [6] | Yang Yuan, Zhang Kaibo, Fu Weili, Li Jian. Epidemiology of sports-induced meniscus injury: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(31): 5079-5084. |
| [7] | Li Shuzhen, Wang Hao, Han Jie, Liang Haibo, Qin Zhi, Sun Ke, Yin Dong. Early versus late reconstruction of anterior cruciate ligament with tendon autografts under arthroscopy [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(26): 4170-4174. |
| [8] | Feng Lei, Wang Jing-xue, Wang Guo-hua, Song Xiu-feng, Zhang Ting-ting, Zhang Tong. Knee meniscus injury evaluated with magnetic resonance imaging [J]. Chinese Journal of Tissue Engineering Research, 2013, 17(30): 5545-5550. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||