Chinese Journal of Tissue Engineering Research ›› 2025, Vol. 29 ›› Issue (30): 6574-6582.doi: 10.12307/2025.911
Previous Articles Next Articles
Association between neuroimaging changes and osteonecrosis: a large sample analysis from UK Biobank and FinnGen databases
Zhang Bochun1, Li Wei1, Li Guangzheng1, Ding Haoqin1, Li Gang2, Liang Xuezhen1, 2
- 1First College of Clinical Medicine, Shandong University of Traditional Chinese Medicine, Jinan 250355, Shandong Province, China; 2Department of Orthopaedic Microsurgery, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan 250014, Shandong Province, China
-
Received:2024-10-18Accepted:2024-11-26Online:2025-10-28Published:2025-03-29 -
Contact:Liang Xuezhen, MD, Associate professor, Master’s supervisor, First College of Clinical Medicine, Shandong University of Traditional Chinese Medicine, Jinan 250355, Shandong Province, China; Department of Orthopaedic Microsurgery, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan 250014, Shandong Province, China -
About author:Zhang Bochun, MS, First College of Clinical Medicine, Shandong University of Traditional Chinese Medicine, Jinan 250355, Shandong Province, China -
Supported by:National Natural Science Foundation of China, No. 82074453 (to LG); National Natural Science Foundation of China (Youth Project), No. 82205154 (to LXZ); Shandong Natural Science Foundation (Youth Project), No. ZR2021QH004 (to LXZ); Shandong Natural Science Foundation of China (General Project), No. ZR2024MH156 (to LXZ)
CLC Number:
Cite this article
Zhang Bochun, Li Wei, Li Guangzheng, Ding Haoqin, Li Gang, Liang Xuezhen, . Association between neuroimaging changes and osteonecrosis: a large sample analysis from UK Biobank and FinnGen databases[J]. Chinese Journal of Tissue Engineering Research, 2025, 29(30): 6574-6582.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
"
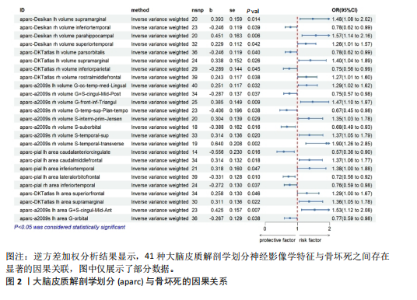
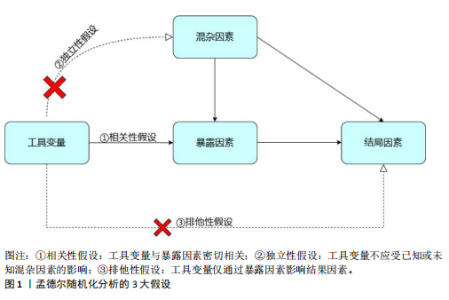
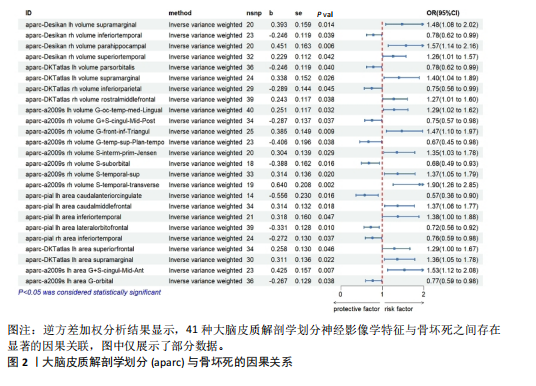
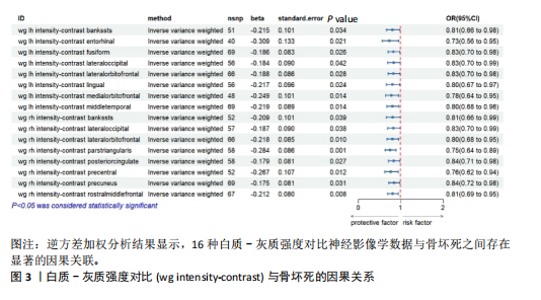
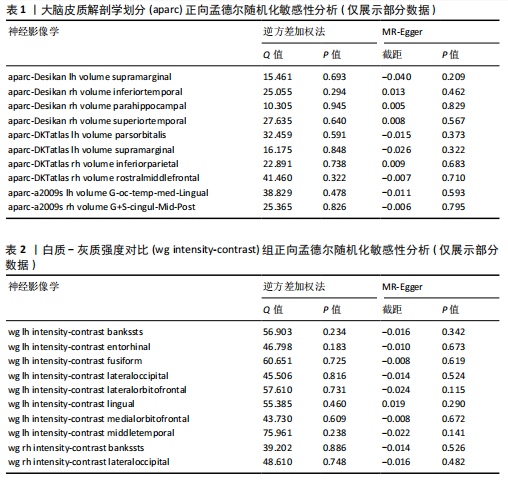
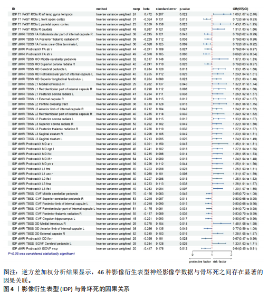
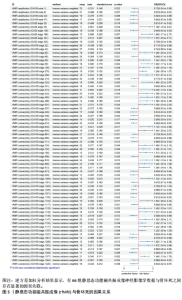
2.1 正向工具变量的筛选 此次研究对检测到的神经影像学特征数据进行了工具变量筛选,所得到的工具变量数据F值均 > 10,未发现F < 10的弱工具变量,证明因弱工具变量带来偏倚的可能性较小。 2.2 神经影像学变化对骨坏死的因果效应 在进行两样本孟德尔随机化分析时,采用Cochran’s Q检验来评估不同研究间的异质性,结果显示研究间没有显著的异质性(P > 0.05),因此选用固定效应模型来估算神经影像学变化与骨坏死之间的因果关系。结果显示共192种神经影像学特征与骨坏死存在可靠的潜在因果关系,其中97种神经影像学特征可以提高骨坏死的发病率(OR > 1,P < 0.05),而其余的95种则是骨坏死的保护因素,可以降低骨坏死的发生率(OR < 1,P < 0.05)。对所得到的数据进行整理分类,主要依据数据的首个单词进行划分,首个单词相同的数据被归为同一组,而数量较少的数据则被归入一组,最终共形成了5组数据:大脑皮质的解剖学划分(anatomical parcellation of the cerebral cortex,aparc)41种,白质-灰质强度对比[white-Grey(wg)intensity-contrast]16种,影像衍生表型(imaging- derived phenotypes,IDP)48种,静息态功能磁共振成像(resting-state functional magnetic resonance imaging,rfMRI)70种,剩余17种数据编为一组,对这5组数据进行逐一分析。 2.2.1 大脑皮质解剖学划分与骨坏死 两样本孟德尔随机化和逆方差加权分析结果显示,41种大脑皮质的解剖学划分神经影像学特征与骨坏死之间存在显著的因果关联(P均< 0.05),见图2。敏感性分析结果显示数据不存在异质性,但发现有两种数据存在水平多效性(aparc-pial lh area caudalmiddlefrontal,aparc-a2009s rh volume G-front-inf-Triangul),为确保结果的准确性,避免对结果产生影响,故除去这两组数据,共得到39组具有显著因果关系的数据,其中aparc-DKTatlas rh thickness medialorbitofrontal是最显著的潜在保护因素(逆方差加权分析结果OR=0.471,95%CI:0.317- 0.700,P=0.000 191 909),其他孟德尔随机化分析方法也得到了相似结果。潜在危险因素有:aparc-Desikan lh volume supramarginal、aparc-Desikan rh volume parahippocampal、aparc-Desikan rh volume superiortemporal等,潜在保护因素有:aparc-DKTatlas lh volume parsorbitalisaparc-DKTatlas rh volume inferiorparietal、aparc-a2009s rh volume G+S-cingul-Mid-Post等,见表1。 除了少数神经影像学数据的分析结果在不同方法间有所差异之外,大多数特征的分析结果在多种方法中显示出高度一致性。逆方差加权法相对简单高效,以每个遗传工具变量与暴露因素的关联效应大小和标准误为主要参数,通过对多个遗传工具变量估计值进行加权合并,得到总体因果效应的估计[30-31]。在没有异质性或水平多效性问题的情况下,以逆方差加权法为金标准,其余方法作为补充[32]。 2.2.2 白质-灰质强度对比与骨坏死 两样本孟德尔随机化和逆方差加权分析结果显示,16种白质-灰质强度对比神经影像学数据与骨坏死之间存在显著的因果关联(P均< 0.05),见图3。白质-灰质强度对比数据全部为潜在的保护因素,其中最显著的潜在保护因素是wg rh intensity-contrast"
"
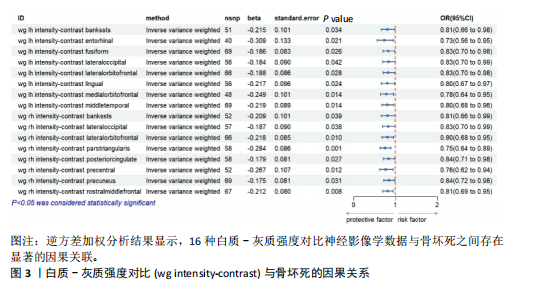
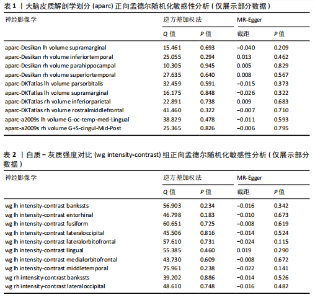
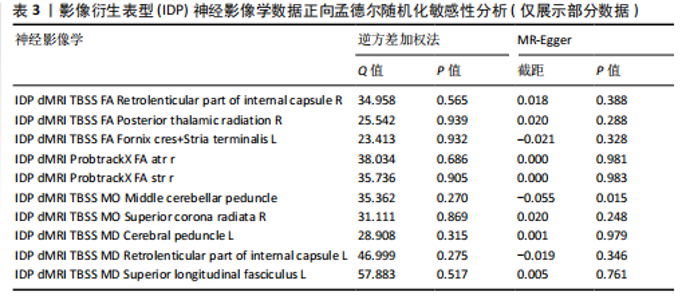
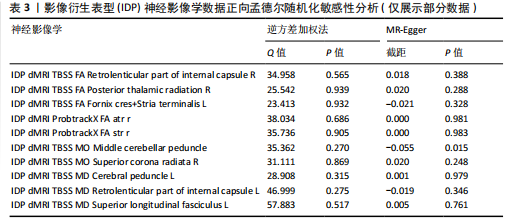
parstriangularis(逆方差加权分析结果OR=0.753,95%CI:0.636-0.891,P= 0.001),其他孟德尔随机化分析结果与逆方差加权法相似。逆方差加权法法是孟德尔随机化的主要研究方法,其余4种方法也有很重要的统计意义,当各种统计方法之间数据存在差异时以逆方差加权法为准。 Cochran’s Q检验结果显示数据没有显著的异质性(P > 0.05),故选择固定效应模型来处理数据。利用MR-Egger回归和MR-presso方法对数据进行水平多效性检验,结果显示所有神经影像学特征数据中不存在显著的水平多效性问题(P均> 0.05),见表2,进一步确认了因果分析结果的稳定性。 2.2.3 影像衍生表型与骨坏死 两样本孟德尔随机化和逆方差加权分析结果显示,48种影像衍生表型神经影像学数据与骨坏死之间存在显著的因果关联(P均< 0.05)。敏感性分析结果显示数据不存在异质性,但发现有两种数据存在水平多效性(IDP dMRI TBSS MO Middle cerebellar peduncle,IDP T1 FAST ROIs R caudate)为确保结果的准确性,避免对结果产生影响,故除去这两组数据,共得到46种具有显著因果关系的数据,见图4、表3。IDP dMRI ProbtrackX FA str r是其中最显著的的保护性因素(逆方差加权分析结果OR=0.686,95%CI:0.559-0.843,P=0.000 3),其他孟德尔随机化分析结果与逆方差加权法相似。潜在的保护"
"
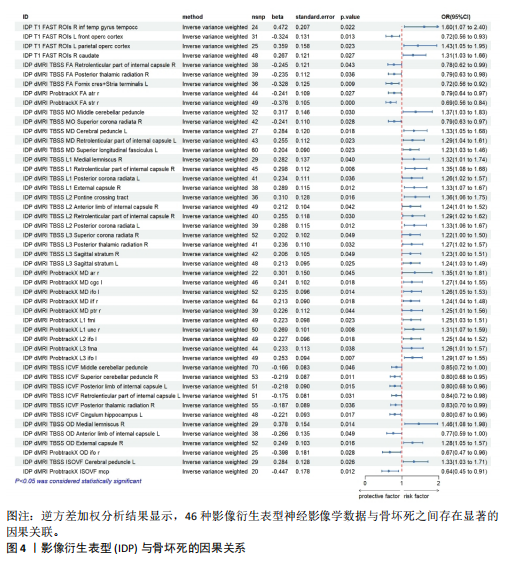
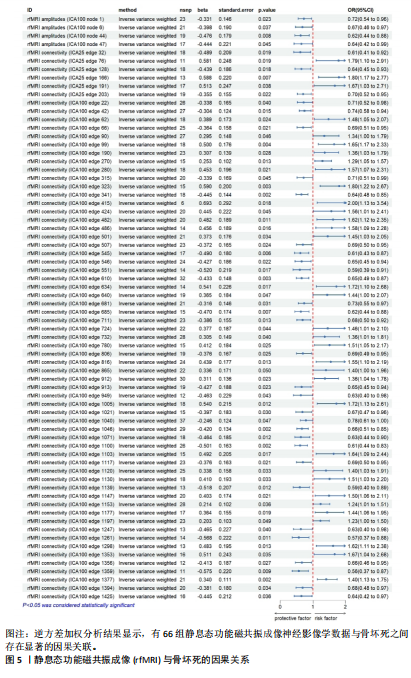
因素有:IDP dMRI ProbtrackX FA str r、IDP dMRI TBSS FA Fornix cres+Stria terminalis L、IDP dMRI TBSS ICVF Superior cerebellar peduncle R,潜在的危险因素有:IDP dMRI ProbtrackX L3 ifo l、IDP dMRI ProbtrackX L1 unc r,IDP dMRI TBSS L1 Retrolenticular part of internal capsule R。 2.2.4 静息态功能磁共振成像与骨坏死 共检测到70种静息态功能磁共振成像神经影像学数据,敏感性分析结果显示有两种神经影像学数据存在异质性[rfMRI connectivity (ICA100 edge 724),rfMRI connectivity (ICA100 edge 681)],两种数据存在水平多效性 [rfMRI connectivity (ICA100 edge 1247),rfMRI amplitudes (ICA100 node 47)],出于对结果稳定性和准确性的考虑,剔除这4组数据,从而得到了66组具有显著因果关系的数据,见图5、 表4。最显著的前三均为保护因素,分别是rfMRI connectivity (ICA100 edge 1046)、rfMRI connectivity (ICA100 edge 341)、rfMRI connectivity (ICA100 edge 1100)。 2.2.5 其他组别数据与骨坏死 最后因剩余的数据较少,所以归为一组进行分析。经过对数据进行筛选,发现共有17组数据与骨坏死存在显著的因果关联(P均< 0.05),见图6、表5。敏感性分析结果显示数据不存在异质性和水平多效性,其中最显著的潜在保护因素为HippSubfield lh volume Whole-hippocampus(逆方差加权分析结果OR=0.727,95%CI:0.581-0.909,P=0.005),最显著的潜在危险因素为aseg rh volume Pallidum(逆方差加权分析结果OR=1.359,95%CI:1.086-1.701,P=0.007)。 2.3 骨坏死对神经影像学的影响 基于上述神经影像学与骨坏死的因果关系结果,将骨坏死作为暴露因素进行反向孟德尔随机化分析,以深入了解骨坏死与神经影像学之间的因果关系。根据P < 5×10-5的临界值选择单核苷酸多态性,经过反向孟德尔随机化分析共得出147组数据,对数据进行敏感性分析,有5组数据存在异质性,有9组数据存在水平多效性,有2组数据(ThalamNuclei rh volume Whole-thalamus,rfMRI connectivity"
"
| [1] ZHAO Y, LI S, FENG M, et al. Effects of Puerarin-Loaded Tetrahedral Framework Nucleic Acids on Osteonecrosis of the Femoral Head. Small. 2023;19(41): e2302326. [2] GUO P, GAO F, WANG Y, et al. The use of anticoagulants for prevention and treatment of osteonecrosis of the femoral head: A systematic review. Medicine (Baltimore). 2017;96(16):e6646. [3] SHAH KN, RACINE J, JONES LC, et al. Pathophysiology and risk factors for osteonecrosis. Curr Rev Musculoskelet Med. 2015;8(3):201-209. [4] STEFFEN RT, ATHANASOU NA, GILL HS, et al. Avascular necrosis associated with fracture of the femoral neck after hip resurfacing: histological assessment of femoral bone from retrieval specimens. J Bone Joint Surg Br. 2010;92(6):787-793. [5] MOTTA F, TIMILSINA S, GERSHWIN ME, et al. Steroid-induced osteonecrosis. J Transl Autoimmun. 2022;5:100168. [6] SCAGLIONE M, FABBRI L, CELLI F, et al. Hip replacement in femoral head osteonecrosis: current concepts. Clin Cases Miner Bone Metab. 2015;12 (Suppl 1):51-54. [7] SEVERYNS M, GAYET LE. Aseptic osteonecrosis of the femoral head in patients with sickle cell anemia. Morphologie. 2021;105(349):94-101. [8] PASCARELLA R, FANTASIA R, SANGIOVANNI P, et al. Traumatic hip fracture-dislocation: A middle-term follow up study and a proposal of new classification system of hip joint associated injury. Injury. 2019;50 Suppl 4: S11-S20. [9] LI Z, YANG B, WENG X, et al. Emerging roles of MicroRNAs in osteonecrosis of the femoral head. Cell Prolif. 2018;51(1): e12405. [10] DONG H, ZHU T, ZHANG M, et al. Polymer Scaffolds-Enhanced Bone Regeneration in Osteonecrosis Therapy. Front Bioeng Biotechnol. 2021;9:761302. [11] YEN C, LIN CL, CHIANG MC. Exploring the Frontiers of Neuroimaging: A Review of Recent Advances in Understanding Brain Functioning and Disorders. Life (Basel). 2023;13(7):1472. [12] HUANG Y, TANG C, WANG S, et al. Acupuncture regulates the glucose metabolism in cerebral functional regions in chronic stage ischemic stroke patients--a PET-CT cerebral functional imaging study. BMC Neurosci. 2012;13:75. [13] MAKARY MM, LEE J, LEE E, et al. Phantom Acupuncture Induces Placebo Credibility and Vicarious Sensations: A Parallel fMRI Study of Low Back Pain Patients. Sci Rep. 2018;8(1):930. [14] HAUCK M, SCHRÖDER S, MEYER-HAMME G, et al. Acupuncture analgesia involves modulation of pain-induced gamma oscillations and cortical network connectivity. Sci Rep. 2017;7(1):16307. [15] FULLANA MA, CARDONER N, ALONSO P, et al. Brain regions related to fear extinction in obsessive-compulsive disorder and its relation to exposure therapy outcome: a morphometric study. Psychol Med. 2014; 44(4):845-856. [16] HASHMI JA, BARIA AT, BALIKI MN, et al.Brain networks predicting placebo analgesia in a clinical trial for chronic back pain. Pain. 2012;153(12):2393-2402. [17] WHITFIELD-GABRIELI S, GHOSH SS, NIETO-CASTANON A, et al. Brain connectomics predict response to treatment in social anxiety disorder. Mol Psychiatry. 2016;21(5): 680-685. [18] LIU J, MU J, LIU Q, et al. Brain structural properties predict psychologically mediated hypoalgesia in an 8-week sham acupuncture treatment for migraine. Hum Brain Mapp. 2017;38 (9): 4386-4397. [19] MA J, WU JJ, HUA XY, et al. Alterations in brain structure and function in patients with osteonecrosis of the femoral head: a multimodal MRI study. PeerJ. 2021;9: e11759. [20] FENG S, LI B, LI G, et al. Abnormal Spatial Patterns of Intrinsic Brain Activity in Osteonecrosis of the Femoral Head: A Resting-State Functional Magnetic Resonance Imaging Study. Front Hum Neurosci. 2020;14:551470. [21] BOWDEN J, HOLMES MV. Meta-analysis and Mendelian randomization: A review. Res Synth Methods. 2019;10(4):486-496. [22] BIRNEY E. Mendelian Randomization. Cold Spring Harb Perspect Med. 2022;12(4): a041302. [23] LIU JZ, VAN SOMMEREN S, HUANG H, et al. Association analyses identify 38 susceptibility loci for inflammatory bowel disease and highlight shared genetic risk across populations. Nat Genet. 2015;47(9): 979-986. [24] EMDIN CA, KHERA AV, KATHIRESAN S. Mendelian Randomization. JAMA. 2017; 318(19):1925-1926. [25] ZOCCALI C, TESTA A, SPOTO B, et al. Mendelian randomization: a new approach to studying epidemiology in ESRD. Am J Kidney Dis. 2006;47(2):332-341. [26] MARCH L, SMITH EU, HOY DG, et al. Burden of disability due to musculoskeletal (MSK) disorders. Best Pract Res Clin Rheumatol. 2014;28(3):353-366. [27] BURGESS S, BUTTERWORTH A, THOMPSON SG. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658-665. [28] BURGESS S, THOMPSON SG. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. 2011;40(3):755-764. [29] LI W, XU JW, CHAI JL, et al. Complex causal association between genetically predicted 731 immunocyte phenotype and osteonecrosis: a bidirectional two-sample Mendelian randomization analysis. Int J Surg. 2024;110(6):3285-3293. [30] XU J, ZHANG S, TIAN Y, et al. Genetic Causal Association between Iron Status and Osteoarthritis: A Two-Sample Mendelian Randomization. Nutrients. 2022;14(18): 3683. [31] MOUNIER N, KUTALIK Z. Bias correction for inverse variance weighting Mendelian randomization. Genet Epidemiol. 2023; 47(4):314-331. [32] MANOUSAKI D, HARROUD A, MITCHELL RE, et al. Vitamin D levels and risk of type 1 diabetes: A Mendelian randomization study. PLoS Med. 2021;18(2):e1003536. [33] LIU N, ZHENG C, WANG Q, et al. Treatment of non-traumatic avascular necrosis of the femoral head (Review). Exp Ther Med. 2022;23(5):321. [34] CHUGHTAI M, PIUZZI NS, KHLOPAS A, et al. An evidence-based guide to the treatment of osteonecrosis of the femoral head. Bone Joint J. 2017;99-b(10):1267-1279. [35] XING XX, HUA XY, ZHENG MX, et al. High-order Brain Networks Abnormalities in Osteonecrosis of the Femoral Head Patients: An Independent Component Analysis of Resting-state fMRI. Pain Physician. 2022; 25(9):E1475-e1484. [36] MA J, HUA XY, ZHENG MX, et al. Surface-based map plasticity of brain regions related to sensory motor and pain information processing after osteonecrosis of the femoral head. Neural Regen Res. 2022;17(4):806-811. [37] MICHAEL JW, SCHLÜTER-BRUST KU, EYSEL P. The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee. Dtsch Arztebl Int. 2010;107(9):152-162. [38] 李民仆,胡佳琦,温春蕾,等.膝关节骨性关节炎射频治疗研究进展[J].中国疼痛医学杂志,2020,26(1):61-65. [39] 徐清榜,郑小岚,陈永兵,等.艾瑞昔布片联合加巴喷丁用于膝关节骨性关节炎病人镇痛研究[J].中国疼痛医学杂志, 2020,26(5):389-392. [40] “中医推拿治疗膝骨关节炎技术规范研究”课题组,张政,谢利民,等.膝骨关节炎中医推拿治疗技术规范专家共识[J]中医杂志,2020,61(16):1469-1472. [41] SONI A, WANIGASEKERA V, MEZUE M, et al. Central Sensitization in Knee Osteoarthritis: Relating Presurgical Brainstem Neuroimaging and PainDETECT-Based Patient Stratification to Arthroplasty Outcome. Arthritis Rheumatol. 2019;71(4): 550-560. [42] 郭光昕,朱清广,徐善达,等.基于脑功能磁共振成像技术探讨中医推拿镇痛脑机制[J].中华中医药杂志,2020,35(12): 6268-6271. [43] KANG BX, MA J, SHEN J, et al. Altered brain activity in end-stage knee osteoarthritis revealed by resting-state functional magnetic resonance imaging. Brain Behav. 2022;12(1):e2479. [44] 石爱军,李春雷,吴媛,等.膝骨性关节炎患者慢性疼痛静息态脑功能局部一致性研究[J].局解手术学杂志,2017, 26(6):419-422. |
| [1] | Zhang Yibo, Lu Jianqi, Mao Meiling, Pang Yan, Dong Li, Yang Shangbing, Xiao Xiang. Exploring the causal relationship between rheumatoid arthritis and coronary atherosclerosis: a Mendel randomized study involving serum metabolites and inflammatory factors [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(在线): 1-9. |
| [2] | Chen Jiayong, Tang Meiling, Lu Jianqi, Pang Yan, Yang Shangbing, Mao Meiling, Luo Wenkuan, Lu Wei, Zhou Jiatan. Based on Mendelian randomization, the causal relationship between 1400 metabolites and sarcopenia and the correlation analysis of cardiovascular disease were investigated [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(在线): 1-11. |
| [3] | Jin Jiming, Hao Yangquan, Zhao Rushun, Zhang Yuting, Jiang Yonghong, Xu Peng, Lu Chao. Application of bilateral hip magnetic resonance imaging to predict risk of osteonecrosis of femoral head [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(9): 1890-1896. |
| [4] | Dong Tingting, Chen Tianxin, Li Yan, Zhang Sheng, Zhang Lei. Causal relationship between modifiable factors and joint sports injuries [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(9): 1953-1962. |
| [5] | Chen Shuai, Jin Jie, Han Huawei, Tian Ningsheng, Li Zhiwei . Causal relationship between circulating inflammatory cytokines and bone mineral density based on two-sample Mendelian randomization [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(8): 1556-1564. |
| [6] |
Zhao Wensheng, Li Xiaolin, Peng Changhua, Deng Jia, Sheng Hao, Chen Hongwei, Zhang Chaoju, He Chuan.
Gut microbiota and osteoporotic fractures #br#
#br#
[J]. Chinese Journal of Tissue Engineering Research, 2025, 29(6): 1296-1304.
|
| [7] | Ma Haoyu, Qiao Hongchao, Hao Qianqian, Shi Dongbo. Causal effects of different exercise intensities on the risk of osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(6): 1305-1311. |
| [8] | Li Jiatong, Jin Yue, Liu Runjia, Song Bowen, Zhu Xiaoqian, Li Nianhu . Association between thyroid function levels and phenotypes associated with sarcopenia [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(6): 1312-1320. |
| [9] | Wu Guangtao, Qin Gang, He Kaiyi, Fan Yidong, Li Weicai, Zhu Baogang, Cao Ying . Causal relationship between immune cells and knee osteoarthritis: a two-sample bi-directional Mendelian randomization analysis [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(5): 1081-1090. |
| [10] | Yu Qinghe, Cai Ziming, Wu Jintao, Ma Pengfei, Zhang Xin, Zhou Longqian, Wang Yakun, Lin Xiaoqin, Lin Wenping. Vanillic acid inhibits inflammatory response and extracellular matrix degradation of endplate chondrocytes [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(30): 6391-9397. |
| [11] | Fan Jiaxin, Jia Xiang, Xu Tianjie, Liu Kainan, Guo Xiaoling, Zhang Hui, Wang Qian . Metformin inhibits ferroptosis and improves cartilage damage in osteoarthritis model rats [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(30): 6398-6408. |
| [12] | Zhou Ying, Tian Yong, Zhong Zhimei, Gu Yongxiang, Fang Hao. Inhibition of tumor necrosis factor receptor associated factor 6 regulates mTORC1/ULK1 signaling and promotes autophagy to improve myocardial injury in sepsis mice [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(30): 6434-6440. |
| [13] | Wang Wanchun, , Yi Jun, Yan Zhangren, Yang Yue, Dong Degang, Li Yumei. 717 Jiedu Decoction remodels homeostasis of extracellular matrix and promotes repair of local injured tissues in rats after Agkistrodon halys bite [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(30): 6457-6465. |
| [14] | Zhang Xin, Guo Baojuan, Xu Huixin, Shen Yuzhen, Yang Xiaofan, Yang Xufang, Chen Pei. Protective effects and mechanisms of 3-N-butylphthalide in Parkinson’s disease cell models [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(30): 6466-6473. |
| [15] | Zhang Songjiang, Li Longyang, Zhou Chunguang, Gao Jianfeng. Central anti-inflammatory effect and mechanism of tea polyphenols in exercise fatigue model mice [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(30): 6474-6481. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||