Chinese Journal of Tissue Engineering Research ›› 2021, Vol. 25 ›› Issue (23): 3746-3751.doi: 10.12307/2021.049
Previous Articles Next Articles
Interpretation of diagnostic criteria for cervicogenic headache: challenges and understandings in diagnosis and differential diagnosis
Liu Zhiwei1, 2, Xie Rui1, Sun Kai1, Li Kaiming1, Wang Xiongwei1, 2, Zhan Jiawen1, 3, Zhu Liguo1, 3
- 1Department of Spine, Wangjing Hospital, China Academy of Chinese Medical Sciences, Beijing 100102, China; 2Beijing University of Chinese Medicine, Beijing 100029, China; 3Beijing Key Laboratory of TCM Bone Setting, Beijing 100102, China
-
Received:2020-05-11Revised:2020-05-16Accepted:2020-08-04Online:2021-08-18Published:2021-02-24 -
Contact:Zhu Liguo, MD, Chief physician, Doctoral supervisor, Department of Spine, Wangjing Hospital, China Academy of Chinese Medical Sciences, Beijing 100102, China; Beijing Key Laboratory of TCM Bone Setting, Beijing 100102, China Co-corresponding author: Zhan Jiawen, MD, Associate chief physician, Department of Spine, Wangjing Hospital, China Academy of Chinese Medical Sciences, Beijing 100102, China; Beijing Key Laboratory of TCM Bone Setting, Beijing 100102, China -
About author:Liu Zhiwei, MD candidate, Attending physician, Department of Spine, Wangjing Hospital, China Academy of Chinese Medical Sciences, Beijing 100102, China; Beijing University of Chinese Medicine, Beijing 100029, China -
Supported by:National Administration of Traditional Chinese Medicine: International Cooperation Base of Traditional Chinese Medicine for Rehabilitation Medical Treatment, No. GZYYGJ2018032 (to ZLG); the National Natural Science Foundation of China, No. 81674005 and 81774330 (both to ZLG); the Special Research Project of Traditional Chinese Medicine Industry, No. 201407001 (to ZLG)
CLC Number:
Cite this article
Liu Zhiwei, Xie Rui, Sun Kai, Li Kaiming, Wang Xiongwei, Zhan Jiawen, Zhu Liguo. Interpretation of diagnostic criteria for cervicogenic headache: challenges and understandings in diagnosis and differential diagnosis[J]. Chinese Journal of Tissue Engineering Research, 2021, 25(23): 3746-3751.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
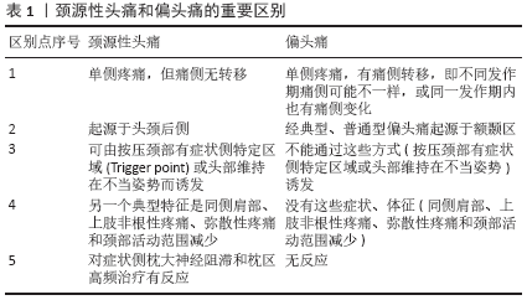
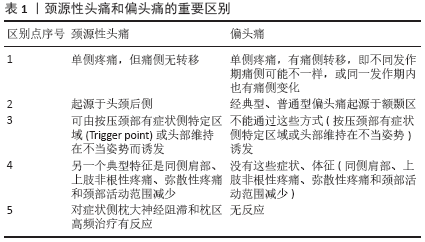
2.1 颈源性头痛CHISG标准 1983年SJAASTAD等[2]提出了颈源性头痛(Cervicogenic Headache)的概念,并特别说明“cervical headache”“migraine cervicale”这样的描述是不准确的。当时有很多经验丰富的高年资神经病学专家提出了质疑,认为“颈源性头痛”描述的应该是一类普通偏头痛。颈源性头痛与偏头痛存在很多共同特征,以至于将二者清晰诊断鉴别变得非常困难。针对这一质疑,SJAASTAD[3]对颈源性头痛与偏头痛的区别进行了整理,对颈源性头痛给出了定义。颈源性头痛是起源于颈部或头后部,并在数分钟内蔓延到眼区和额颞区,在眼区和额颞区疼痛达到最大程度的头痛;具体起源于颈部哪些区域尚未有明确的证据。单次发作一般持续数小时到数天,单次发作会逐渐发展为慢性、波动性发作头痛,发作期的不可预测性也是颈源性头痛的一个特点。SJAASTAD认为颈源性头痛患者女性较多,约占75%,多数患者都有挥鞭样损伤史;枕大神经阻滞作为一项重要的诊断试验,可以减轻眼区和额颞区等未被麻醉区域的疼痛,也部分揭示了颈源性头痛的发病机制;疼痛为中到重度,并和丛集性头痛、慢性阵发性偏头痛一样为单侧头痛无痛侧转移。在持续时间长重度发作的患者,疼痛可能超过中线,但原发病侧疼痛程度更重。颈源性头痛和偏头痛的重要区别见表1。 "
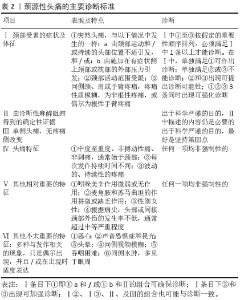
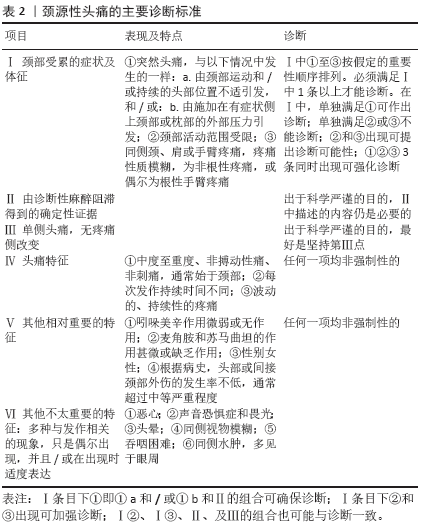
1990年在以SJAASTAD等为首的颈源性头痛国际研究小组(The Cervicogenic Headache International Study Group,CHISG)提出了颈源性头痛诊断标准,由于当时局部麻醉阻滞尚未被医师普遍掌握,该标准未将局部麻醉阻滞定为必备条目。1998年CHISG再次更新该诊断标准[4](表2),将局部麻醉阻滞定为颈源性头痛科学诊断评估必备条目,尤其在双侧疼痛(可能与紧张型头痛混淆)中;此外,原版本所强调疼痛为单侧的标准也被弱化,认为作为科学工作(For scientific work),单侧疼痛应被作为准则,作为常规工作(For routine work),双侧疼痛也可被接受,但仍认为单侧疼痛做出诊断更可靠。VINCENT等[5]对SJAASTAD诊断标准进行临床研究,经统计,招募的颈源性头痛患者均为单侧头痛,而偏头痛患者中仅6.5%为单侧头痛,紧张型头痛患者中无一满足“单侧头痛,无疼痛侧改变”这一标准。同时,吲哚美辛、麦角胺和苏马曲坦等药物也被列出,认为虽然“这些药物无效”尚不足以做出颈源性头痛的诊断,但若这些药物完全有效(完全消除疼痛)则应排除颈源性头痛的诊断。CHISG标准强调不要认为只有骨质结构是发病原因,而神经、神经节、钩椎关节、椎间盘、关节突关节、骨质、骨膜、肌肉、韧带甚至神经节周围的静脉池都可能是病源。"
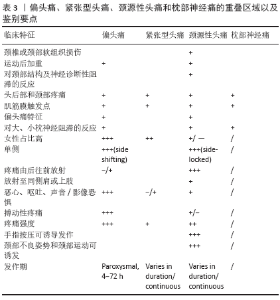
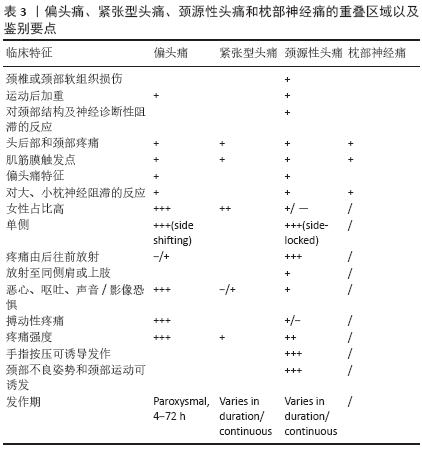
颈源性头痛国际研究小组提出的诊断标准,较详细地阐述了颈源性头痛的概念及鉴别要点,为临床医师提供了学习蓝本,但也存在一些具有争议的地方。 CHISG标准特别说明颈源性头痛不仅起源于上颈段,也起源于中颈段甚至下颈段。MICHLER等[6]报告1例C6-C7椎间盘突出患者,长期患有一侧头痛,在C7神经根减压术后症状消失,为这一点提供了证据。DIENER等[7]报告12例C4以下节段颈椎间盘脱出患者,均新发颈部疼痛伴头痛,其中7例符合颈源性头痛诊断标准,椎间盘摘除术后1周,8例疼痛完全消失,1例明显改善,3例无明显变化;术后3个月随访,7例疼痛完全消失,3例明显改善,2例无明显变化;并通过与对照组比较,推翻了自己之前关于低位颈椎间盘脱出与颈源性头痛无关的假设,并总结为:①低位颈椎间盘脱出患者比对照组有更高的颈部疼痛、头痛发作频率和更多的颈源性头痛频率;②椎间盘摘除术能明显改善颈部疼痛、头痛和颈源性头痛。而BOGDUK等[8]认为目前尚无研究证实下颈节神经分布结构可直接引起头痛,2019年中国疼痛学会发表的专家共识也持同样的观点。 CHISG标准认为局部麻醉阻滞能消除颈源性头痛,不能消除紧张型头痛患者颞区疼痛。SJAASTAD认为局部麻醉阻滞对偏头痛也无效,可以作为鉴别方法。但BARMHERZIG等[9]认为枕部神经痛和颈源性头痛、紧张型头痛、偏头痛对枕大、小神经局部麻醉阻滞都有反应,单独使用神经阻滞不足以区分这些不同类型的头痛。 CHISG标准中列出颈源性头痛特征包含恶心、呕吐、影像/声音恐惧症等特征。VINCENT等[5]研究显示,恶心症状在颈源性头痛患者中占45.5%,在偏头痛患者中占89.2%;呕吐症状在颈源性头痛患者中占21.2%,在偏头痛患者中占60%;影像/声音恐惧症状在颈源性头痛患者中占57.6%,在偏头痛患者中占86.2%。PIKUS等[10]病例系列报告结果提示20%的颈源性头痛患者有恶心呕吐症状,5.7%有影像恐惧。这些研究结果表明恶心、呕吐、影像/声音恐惧等症状在颈源性头痛患者中存在较大比例;同时,恶心、呕吐和影像/声音恐惧也是偏头痛(参照ICHD-3诊断标准)的重要特征,这可能使颈源性头痛与合并有颈部疼痛的偏头痛鉴别变得十分困难。 CHISG的诊断标准中颈源性头痛由颈部运动引发,而根据ICHD-3诊断标准,偏头痛为运动后加重,按照这项条文进行临床鉴别时,患者很难回忆并描述清楚,有可能导致将潜在的偏头痛疾病误诊为颈源性头痛,从而误导治疗。 CHISG强调局部麻醉阻滞对于颈源性头痛诊断的重要性,而另一疾病枕部神经痛对枕大神经麻醉阻滞也有相同效果,过度依赖局部麻醉阻滞可能导致将这两种疾病混淆或误诊。枕部神经痛必须与上颈椎关节引起的牵涉痛(如颈源性头痛)和颈部肌肉肌筋膜触痛点引起的头部牵涉痛(如紧张型头痛或颈源性头痛)区别开。应仔细鉴别由寰枢关节或上颈段关节突关节导致的枕部疼痛,这可能诊断为颈源性头痛更为合适。枕部神经痛无眼眶额颞区牵涉痛,枕大神经出口或C2神经分布区有肌筋膜触发点。轻微按压或叩诊神经有麻刺感(Tinel征),患者躺在床上过伸或旋转颈部引发疼痛(pillow征)也是枕部神经痛的重要特征。 枕部神经痛(ICHD-3)的定义如下:(1)单侧或双侧疼痛,疼痛位于大、小、和/或第三枕神经分布区,并满足标准(2)至(5);(2)疼痛有以下3个特征中的2个:①阵发性发作,持续几秒至几分钟;②疼痛程度严重;③疼痛性质为射击性疼痛、刺痛或锐痛;(3)疼痛与下列2种情况有关:①对头皮和/或头发进行无损伤刺激时有明显的感觉异常和/或异常痛;②以下当中的任1个或2个:a.受累神经分支的压痛;b.枕大神经出口或C2 神经分布区域存在触发点;(4)受影响神经的局部麻醉阻滞可暂时缓解疼痛;(5)另一种ICHD-3诊断不能更好地解释这一现象。 2.2 颈源性头痛ICHD-3诊断标准 作为另一种选择,2013年国际头痛学会(IHS)头痛分类委员会发布了诊断标准The International Classification of Headache Disorders,3rd edition (beta version)(ICHD BETA 3),将头痛详细分型并逐一列出诊断标准。该标准定义更为具体,更加依赖颈椎解剖,条目更加简洁。ICHD BETA 3标准强调颈部疼痛并不是诊断的必要症状。 2018年,经过field testing后,ICHD-3正式发表[11]。ICHD-3强调:①影像学发现只能起到提示作用,而不能确定病因,因为在无头痛患者的上颈椎也可能有同样的影像学表现。②肿瘤、骨折、感染和上颈椎类风湿性关节炎尚未被正式确认为头痛的原因,但在个别病例中已被接受为符合标准B。颈椎病和软骨性骨关节炎可能是也可能不是头痛的原因,是否满足标准B,同样取决于具体病例。③JAEGER[12]为探究颈源性头痛是由肌筋膜疼痛引起的还是由颈椎功能障碍引起的,进行了临床研究,11例颈源性头痛患者中疼痛侧至少有3例筋膜触发点(myofascial trigger points),其中8例患者筋膜触发点触诊可清晰复制出头痛;在疼痛侧有70个筋膜触发点和17个非筋膜压痛点,而非疼痛侧有22个筋膜触发点和19个非筋膜压痛点;所有11例患者都有不同程度颈椎功能障碍,但结论认为筋膜触发点是颈源性头痛的重要发病机制,而节段性颈椎功能障碍是这些患者的一个常见特征。此外,FERNáNDEZ-DE-LAS-PE?AS[13]研究认为,肌筋膜触发点是紧张型头痛发生的潜在病因。鉴于肌筋膜触发点引起头痛应如何诊断尚无统一认识,ICHD-3认为如果某患者颈部肌筋膜疼痛是头痛诱因,则可能诊断为“紧张型头痛”更合适,此外,附录中新增了“颈肌筋膜痛源性头痛”(Headache attributed to cervical myofascial pain)的诊断,等待证据进一步验证。④上颈节神经根性疾病诱发的颈源性头痛已被假定为由上颈节神经和三叉神经会聚作为合理的病因,“上颈节神经根性头痛”(Headache attributed to upper cervical radiculopathy)被列于附录中,等待证据进一步证明。⑤区分颈源性头痛和偏头痛、紧张性头痛的特征包括:侧锁性疼痛、指压颈部肌肉和头部运动刺激出现的典型头痛,以及由后向前的辐射疼痛。虽然这些可能是颈源性头痛的特征,但并不是只在颈源性头痛中出现,它们并不一定互为因果。尽管程度一般小于偏头痛,颈源性头痛患者也可能出现偏头痛的特征如恶心,呕吐和影像/声音恐惧,可以将一些病例同紧张型头痛(影像/声音恐惧中最多有1项,无恶心呕吐或无中重度恶心呕吐)区分开。 颈源性头痛ICHD-3诊断标准如下:A任何符合标准C的头痛;B可能引起头痛的颈椎或颈部软组织紊乱或损伤的临床、实验室和/或影像学证据;C至少被以下中的两条证明的因果关系证据:①头痛的发生与颈椎紊乱或损伤的出现有时间上的关系;②颈椎紊乱或损伤得到改善或解决的同时,头痛明显改善或得到解决;③刺激动作会减少颈椎活动度,使头痛明显加重;④在诊断性阻滞颈椎结构或其神经供应后,头痛完全消失;D另一个ICHD-3诊断也不能更好地解释这一点。 2.3 中华医学会疼痛学分会颈源性头痛专家共识 2019-04-01中华医学会疼痛学分会发表了《The Chinese Association for the Study of Pain (CASP):Expert Consensus on the Cervicogenic Headache》[14]。该共识对颈源性头痛的定义、诊断标准、流行病学、病因、临床特征、鉴别诊断及治疗分别作了详细阐释,其中诊断标准部分沿用了2018年发布的ICHD-3诊断标准;该共识对鉴别诊断和治疗方法作了详细描述,尤其在治疗方法部分详尽具体地说明了每一种治疗方法的适应证,易于学习掌握;虽然为专家共识,但均以文献证据为依据,具有权威性;但该共识未评估报告所依据的证据等级,读者难以了解证据的可靠程度。 2.4 颈源性头痛、枕部神经痛、 紧张型头痛和偏头痛重叠区域及鉴别要点 区别枕部神经痛、颈源性头痛、紧张型头痛和偏头痛经常是困难的,ICHD-3诊断标准尝试对头痛疾病鉴别要点进行描述,但存在部分有重叠特征的病例,表3为偏头痛、紧张型头痛、颈源性头痛, 枕部神经痛的重叠部分以及鉴别要点[15-16]。对于部分病例与此表不符的,仍要单独分析,或等待新的证据进一步证实。 "
| [1] ANARTE E, FERREIRA CARVALHO G, SCHWARZ A, et al. Can physical testing be used to distinguish between migraine and cervicogenic headache sufferers? A protocol for a systematic review. BMJ Open. 2019;9(11):e031587. [2] SJAASTAD O, SAUNTE C, HOVDAHL H, et al. “Cervicogenic headache”. An hypothesis. Cephalalgia. 1983;3(4):249-256. [3] SJAASTAD O. Cervicogenic headache: the controversial headache. Clinical Neurology and Neurosurgery. Clin Neurol Neurosurg. 1992;94:147-149. [4] SJAASTAD O FREDRIKSEN TA, PFAFFENRATH V. Cervicogenic headache: diagnostic criteria. The Cervicogenic Headache International Study Group. Headache. 1998; 38(6):442-445. [5] VINCENT MB, LUNA RA. Cervicogenic headache: a comparison with migraine and tension-type headache.Cephalalgia. 1999;19(25):11-16. [6] MICHLER RP, BOVIM G, SJAASTAD O.Disorders in the lower cervical spine. A cause of unilateral headache? Headache. 1991;31(8):550-551. [7] DIENER H, KAMINSKI M, STAPPERT G,et al. Lower cervical disc prolapse may cause cervicogenic headache:prospective study in patients undergoing surgery. Cephalalgia. 2007;27(9):1050-1054. [8] BOGDUK N, GOVIND J. Cervicogenic headache: an assessment of the evidence on clinical diagnosis,invasive tests, and treatment. Lancet Neurol. 2009;8(10):959-968. [9] BARMHERZIG R, KINGSTON W. Occipital Neuralgia and Cervicogenic Headache: Diagnosis and Management. Curr Neurol Neurosci Rep. 2019;19(5):20. [10] PIKUS HI, PHILLIPS JM. Characteristics of patients successfully treated for cervicogenic headache by surgical decompression of the second cervical root. Headache. 1995;35(10):621-629. [11] Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211. [12] JAEGER B. Are “cervicogenic” headaches due to myofascial pain and cervical spine dysfunction? Cephalalgia. 1989;9(3):157-164. [13] FERNÁNDEZ-DE-LAS-PEÑAS C. Myofascial Head Pain. Curr Pain Headache Rep. 2015;19(7): 28. [14] XIAO H, PENG B, MA K, et al. The Chinese Association for the Study of Pain (CASP): Expert Consensus on the Cervicogenic Headache. Pain Res Manag. 2019; 2019:9617280. [15] BLUMENFELD A, SIAVOSHI S.The Challenges of Cervicogenic Headache. Current Pain and Headache Reports. 2018;22(7):47. [16] VINCENT MB. Cervicogenic Headache: A Review Comparison with Migraine, Tension-Type Headache, and Whiplash. Curr Pain Headache Rep. 2010;14(3):238-243. [17] SJAASTAD O, FREDRIKSEN TA, PFAFFENRATH V. Cervicogenic headache: diagnostic criteria.Headache. 1990;30(11):725-726. [18] D’AMICO D, LEONE M, BUSSONE G. Side-locked unilaterality and pain localization in long-lasting headaches: migraine,tension-type headache, and cervicogenic headache. Headache.1994;34(9):526-530. [19] BING N, TAO D, WEI S, et al. Percutaneous Endoscopic C2-C3 Medial Branches Neurotomy for Cervicogenic Headache. World Neurosurg. 2019;126:498-501. [20] WU B, YUE L, SUN F, et al. The Feasibility and Efficacy of Ultrasound-Guided C2 Nerve Root Coblation for Cervicogenic Headache. Pain Med. 2019;20(6):1219-1226. [21] LI SJ, FENG D. Pulsed radiofrequency of the C2 dorsal root ganglion and epidural steroid injections for cervicogenic headache. Neurol Sci. 2019;40(6):1173-1181. [22] GOADSBY PJ, BARTSCH T. Central Mechanisms of Peripheral Nerve Stimulation in Headache Disorders. Prog Neurol Surg. 2011;24:16-26. [23] PENG B, BOGDUK N. Cervical Discs as a Source of Neck Pain. An Analysis of the Evidence. Pain Med. 2019;20(3):446-455. [24] GOADSBY PJ, RATSCH T. On the functional neuroanatomy of neck pain. Cephalalgia. 2008;28(1):1-7. [25] ASHINA S, BENDTSEN L, LYNGBERG AC, et al. Prevalence of neck pain in migraine and tension-type headache: a population study. Cephalalgia. 2015;35(3):211-219. [26] PEARCE IMS. Cervicogenic headache: a personal view. Cephalalgia. 1995;15(6): 463-469. [27] BOGDUK N.The Neck and Headaches. Neurol Clin. 2014;32(3):471-487. [28] GETSOIAN SL, GULATI SM, OKPAREKE I, et al. Validation of a clinical examination to differentiate a cervicogenic source of headache: a diagnostic prediction model using controlled diagnostic blocks. BMJ Open. 2020;10(5):e035245. [29] RUBIO-OCHOA J, BENÍTEZ-MARTÍNEZ J, LLUCH E, et al.Physical Examination Tests for Screening and Diagnosis of Cervicogenic Headache:Man Ther. 2016;21:35-40. [30] BARMHERZIG R, KINGSTON W. Occipital Neuralgia and Cervicogenic Headache:Diagnosis and Management. Curr Neurol Neurosci Rep. 2019;19(5):20. [31] GE HY, WANG K, MADELEINE P, et al. Simultaneous modulation of the exteroceptive suppression periods in the trapezius and temporalis muscles by experimentalmuscle pain. Clin Neurophysiol. 2004;115(6):1399-1408. [32] POURAHMADI M, MOHSENI-BANDPEI MA, KESHTKAR A,et al.Effectiveness of dry needling for improving pain and disability in adults with tensiontype, cervicogenic, or migraine headaches: protocol for a systematic review. Chiropr Man Therap. 2019;27:43. [33] GILDIR S, TÜZÜN EH, EROĞLU G, et al. A randomized trial of trigger point dry needling versus sham needling for chronic tension-type headache. Medicine. 2019;98(8):1-7. [34] COUPPÉ C, TORELLI P, FUGLSANG-FREDERIKSEN A, et al. Myofascial trigger points are very prevalent in patients with chronic tension-type headache: a double-blinded controlled study. Clin J Pain. 2007;23(1):23-27. [35] FERNÁNDEZ-DE-LAS-PEÑAS C, ALONSO-BLANCO C, CUADRADO ML, et al. Myofascial trigger points and their relationship with headache clinical parameters in chronic tension type headache. Headache. 2006;46(8):1264-1272. [36] FERNÁNDEZ-DE-LAS-PEÑAS C, ALONSO-BLANCO C, CUADRADO ML, et al. Trigger points in the suboccipital musclesand forward head posture in tension type headache. Headache. 2006;46(3):454-460. |
| [1] | Pu Rui, Chen Ziyang, Yuan Lingyan. Characteristics and effects of exosomes from different cell sources in cardioprotection [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(在线): 1-. |
| [2] | Zhang Chao, Lü Xin. Heterotopic ossification after acetabular fracture fixation: risk factors, prevention and treatment progress [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1434-1439. |
| [3] | Zhou Jihui, Li Xinzhi, Zhou You, Huang Wei, Chen Wenyao. Multiple problems in the selection of implants for patellar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1440-1445. |
| [4] | Wang Debin, Bi Zhenggang. Related problems in anatomy mechanics, injury characteristics, fixed repair and three-dimensional technology application for olecranon fracture-dislocations [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1446-1451. |
| [5] | Ji Zhixiang, Lan Changgong. Polymorphism of urate transporter in gout and its correlation with gout treatment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1290-1298. |
| [6] | Yuan Mei, Zhang Xinxin, Guo Yisha, Bi Xia. Diagnostic potential of circulating microRNA in vascular cognitive impairment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1299-1304. |
| [7] | Wang Xianyao, Guan Yalin, Liu Zhongshan. Strategies for improving the therapeutic efficacy of mesenchymal stem cells in the treatment of nonhealing wounds [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1081-1087. |
| [8] | Wan Ran, Shi Xu, Liu Jingsong, Wang Yansong. Research progress in the treatment of spinal cord injury with mesenchymal stem cell secretome [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1088-1095. |
| [9] | Liao Chengcheng, An Jiaxing, Tan Zhangxue, Wang Qian, Liu Jianguo. Therapeutic target and application prospects of oral squamous cell carcinoma stem cells [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1096-1103. |
| [10] | Zhao Min, Feng Liuxiang, Chen Yao, Gu Xia, Wang Pingyi, Li Yimei, Li Wenhua. Exosomes as a disease marker under hypoxic conditions [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1104-1108. |
| [11] | Xie Wenjia, Xia Tianjiao, Zhou Qingyun, Liu Yujia, Gu Xiaoping. Role of microglia-mediated neuronal injury in neurodegenerative diseases [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1109-1115. |
| [12] | Li Shanshan, Guo Xiaoxiao, You Ran, Yang Xiufen, Zhao Lu, Chen Xi, Wang Yanling. Photoreceptor cell replacement therapy for retinal degeneration diseases [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1116-1121. |
| [13] | Jiao Hui, Zhang Yining, Song Yuqing, Lin Yu, Wang Xiuli. Advances in research and application of breast cancer organoids [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1122-1128. |
| [14] | Wang Shiqi, Zhang Jinsheng. Effects of Chinese medicine on proliferation, differentiation and aging of bone marrow mesenchymal stem cells regulating ischemia-hypoxia microenvironment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1129-1134. |
| [15] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||